(UroToday.com) The American Urological Association's 2026 Annual Meeting, was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Paolo Zaurito presented interactive poster IP38-12: Uptake of doublet and triplet therapy for men with de novo metastatic castration sensitive prostate cancer. Population-based study.
Dr. Zaurito began by highlighting that randomized clinical trials have consistently demonstrated improved survival outcomes with treatment intensification strategies in men with de novo metastatic castration-sensitive prostate cancer (mCSPC).1,2 Specifically, both doublet and triplet therapy approaches have shown superiority compared to androgen deprivation therapy alone, leading to incorporation of doublet therapy into clinical guidelines in 2020 and triplet therapy in 2022.2,3 Given the rapidly evolving treatment landscape, the investigators sought to evaluate real-world adoption of upfront doublet and triplet therapy at a population level, as well as associated survival trends among men with de novo mCSPC.
The investigators identified men diagnosed with de novo mCSPC between 2016 and 2024 from the National Prostate Cancer Register of Sweden. Use of docetaxel within 6 months of diagnosis was captured through both the NPCR and regional healthcare information systems, while use of androgen receptor pathway inhibitors was determined using prescription data for abiraterone, enzalutamide, apalutamide, and darolutamide from the national Prescribed Drug Register.
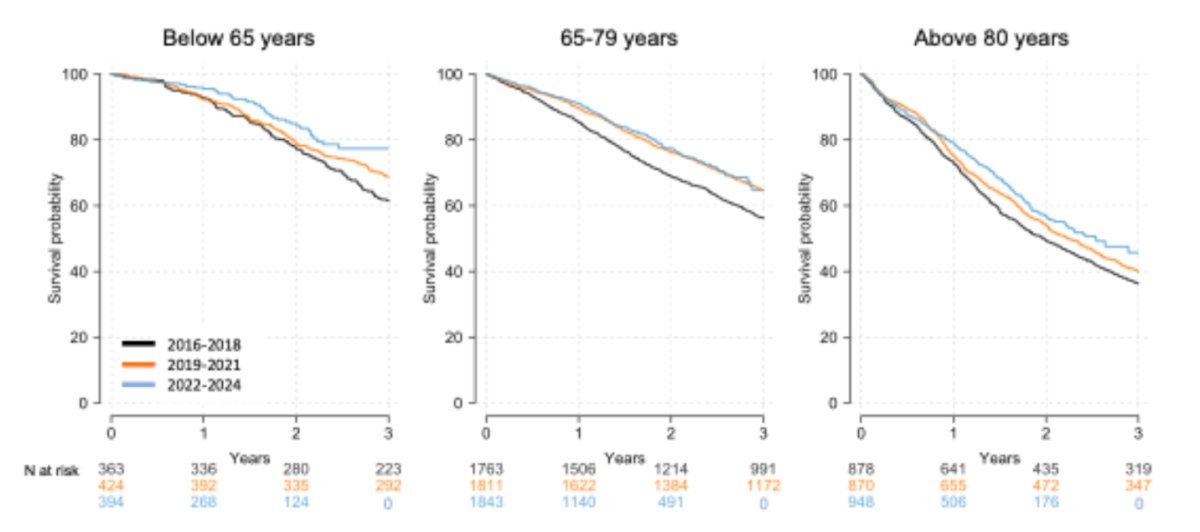
The study evaluated annual uptake of upfront treatment intensification strategies, including doublet therapy consisting of ADT plus either an ARPI or docetaxel, as well as triplet therapy combining ADT, docetaxel, and an ARPI. Survival outcomes were assessed across three treatment eras (2016–2018, 2019–2021, and 2022–2024) using Kaplan-Meier analyses to estimate 3-year overall survival trends over time.
Among 9,294 men diagnosed with de novo mCSPC, median PSA at diagnosis decreased modestly over time, from 104 ng/mL (IQR 28–434) during 2016–2018 to 89 ng/mL (IQR 25–354) during 2022–2024. The investigators observed a marked increase in adoption of treatment intensification strategies over the study period. Use of upfront doublet therapy increased substantially from 19% in 2016 to 66% in 2024, while use of triplet therapy rose from 4% in 2021 to 17% in 2024 following incorporation into clinical guidelines.
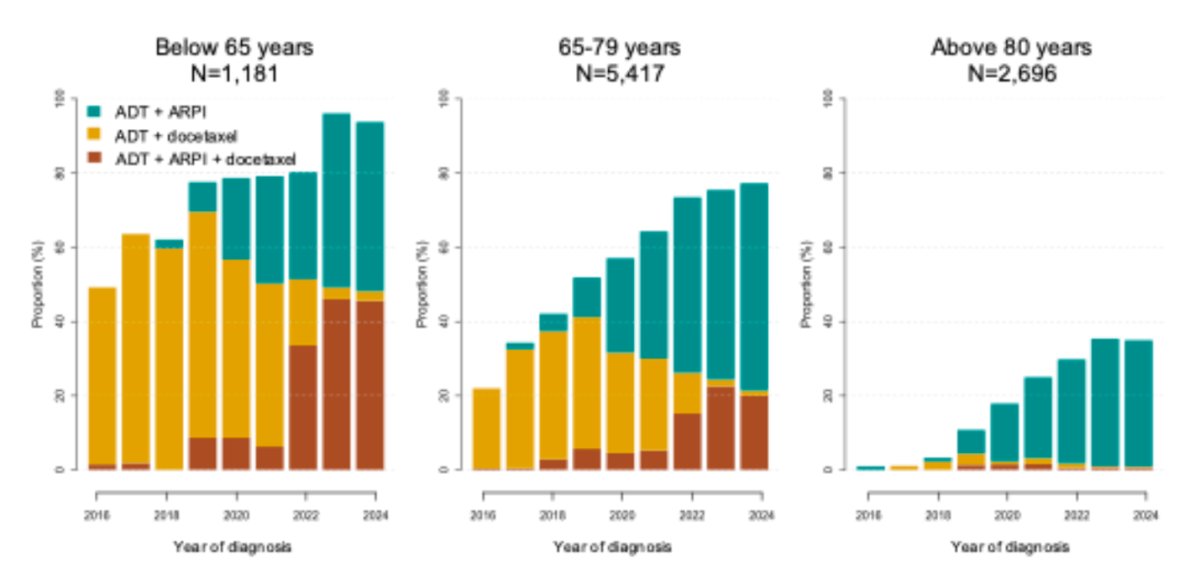
Dr Zaurito highlighted that in the study, patients receiving triplet therapy generally represented a higher-risk population, as these men tended to be younger and demonstrated more advanced disease characteristics, including higher PSA levels, more advanced clinical T stage, and higher Gleason scores.
Importantly, these changes in treatment patterns were accompanied by improvements in survival over time. Three-year overall survival increased from 51% (95% CI 49–52%) during 2016–2018 to 61% (95% CI 58–64%) during 2022–2024.
The survival gains appeared even more pronounced among younger patients, as shown below. In men younger than 65 years, 3-year overall survival improved from 69% (95% CI 65–73) in 2019–2021 to 77% (95% CI 71–84) in 2022–2024, coinciding with increasing adoption of intensified upfront treatment strategies.
Dr. Zaurito concluded with the following key messages:
- Uptake of upfront doublet and triplet therapy increased substantially over the study period, particularly among men younger than 65 years
- In parallel with increased treatment intensification, 3-year overall survival improved across the overall population of men with de novo mCSPC
- These real-world findings support the survival benefit observed with upfront doublet and triplet therapy in randomized clinical trials
- The study provides important population-level evidence that treatment intensification strategies are translating into improved outcomes in routine clinical practice
Presented by: Paolo Zaurito, MD, Urology Resident, IRCSS Ospedale San Raffaele, Milan, Italy
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026
References:
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, Kohli M, Plimack ER, Vogelzang NJ, Picus J, Cooney MM, Garcia JA, DiPaola RS, Sweeney CJ. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018 Apr 10;36(11):1080-1087. doi: 10.1200/JCO.2017.75.3657. Epub 2018 Jan 31. PMID: 29384722; PMCID: PMC5891129.
- Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, Kopyltsov E, Park CH, Alekseev B, Montesa-Pino Á, Ye D, Parnis F, Cruz F, Tammela TLJ, Suzuki H, Utriainen T, Fu C, Uemura M, Méndez-Vidal MJ, Maughan BL, Joensuu H, Thiele S, Li R, Kuss I, Tombal B; ARASENS Trial Investigators. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142. doi: 10.1056/NEJMoa2119115. Epub 2022 Feb 17. PMID: 35179323; PMCID: PMC9844551.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.