(UroToday.com) The 2026 American Urological Association annual meeting featured practice-changing, paradigm-shifting clinical trials in urology and a presentation by Dr. Mark Garzotto discussing extended follow-up of patients treated with CAN-2409 (aglatimagene) + prodrug in combination with standard of care external beam radiotherapy in men with localized prostate cancer. Currently, there is an unmet need in localized prostate cancer, given that globally there are approximately 1.4 million new cases of prostate cancer annually. The ultimate goal of curative treatment is prevention of cancer recurrence, while minimizing treatment related side effects and maintaining quality of life. Standard of care for intermediate to high-risk localized prostate cancer includes surgery or external beam radiation +/- ADT. However, nearly 30% of men undergoing external beam radiation will experience recurrence requiring ADT and salvage therapies that negatively impact quality of life.
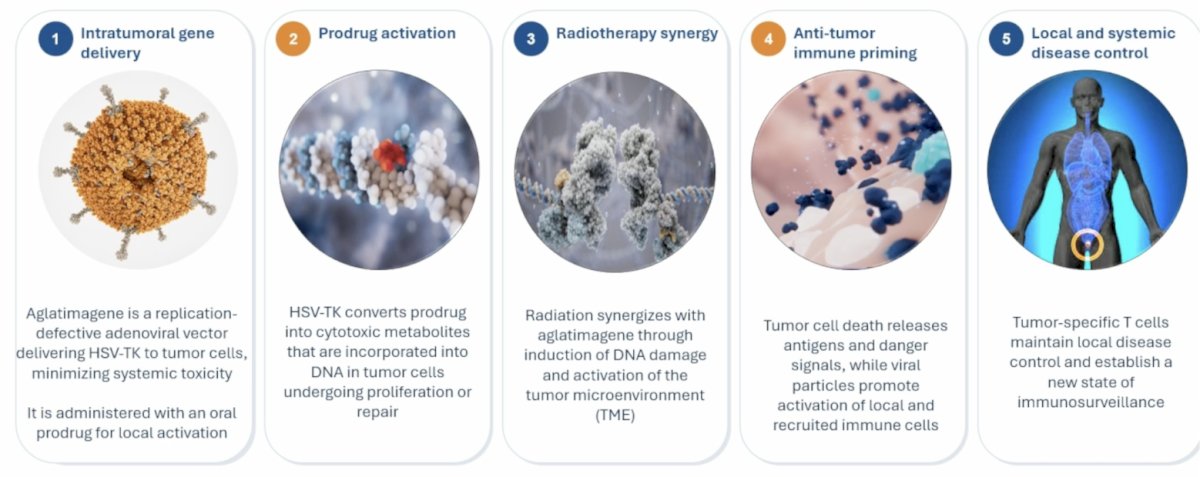
Aglatimagene + the prodrug valacyclovir combined with radiotherapy enhances immune priming, culminating in local disease control and a new state of immuno-surveillance. The mechanism of action includes:
- Intratumoral gene delivery
- Prodrug activation
- Radiotherapy synergy
- Anti-tumor immune priming
- Local and systemic disease control
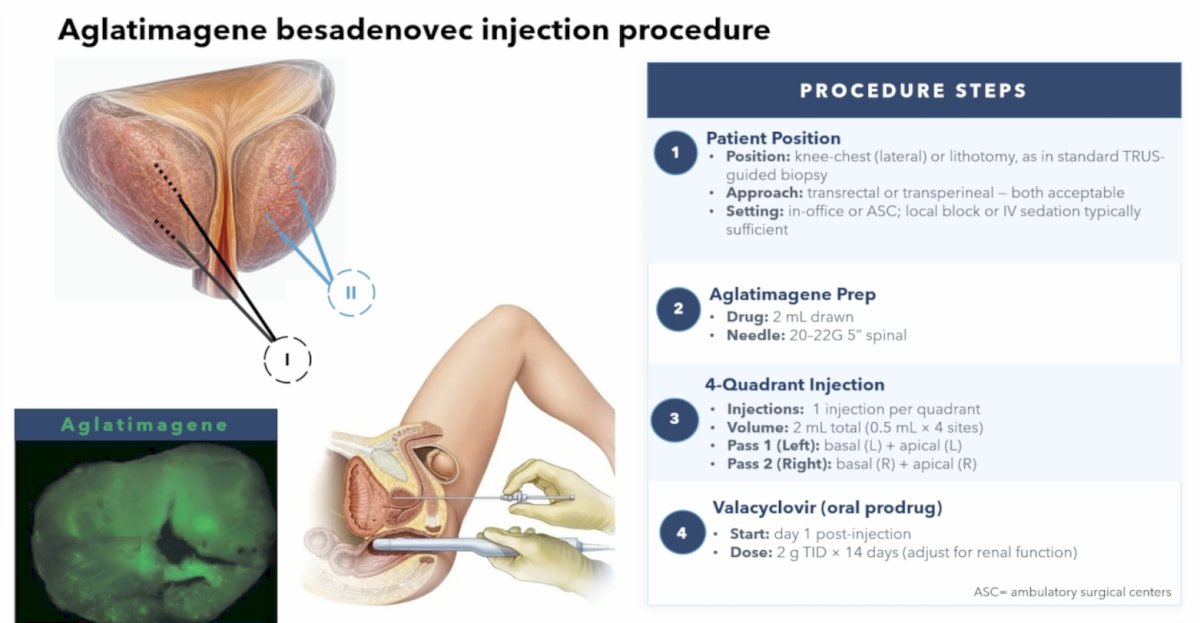
The procedure steps for injecting aglatimagene into the prostate include:
- Patient positioning
- Position: knee-chest (lateral) or lithotomy, as in standard TRUS-guided biopsy
- Approach: transrectal or transperineal – both are acceptable
- Setting: in office or ambulatory surgery center, local block or IV sedation is typically sufficient
- Aglatimagene preparation
- Drug: 2 mL drawn
- Needle: 20-22G 5” spinal
- 4-quadrant injection
- Injections: 1 injection per quadrant
- Volume: 2 mL total (0.5 mL + 4 sites)
- Pass 1 left: basal (left) + apical (left)
- Pass 2 right: basal (right) + apical (right)
- Valacyclovir (oral prodrug)
- Start: day 1 post-injection
- Dose: 2 g TID x 14 days (adjust for renal function)
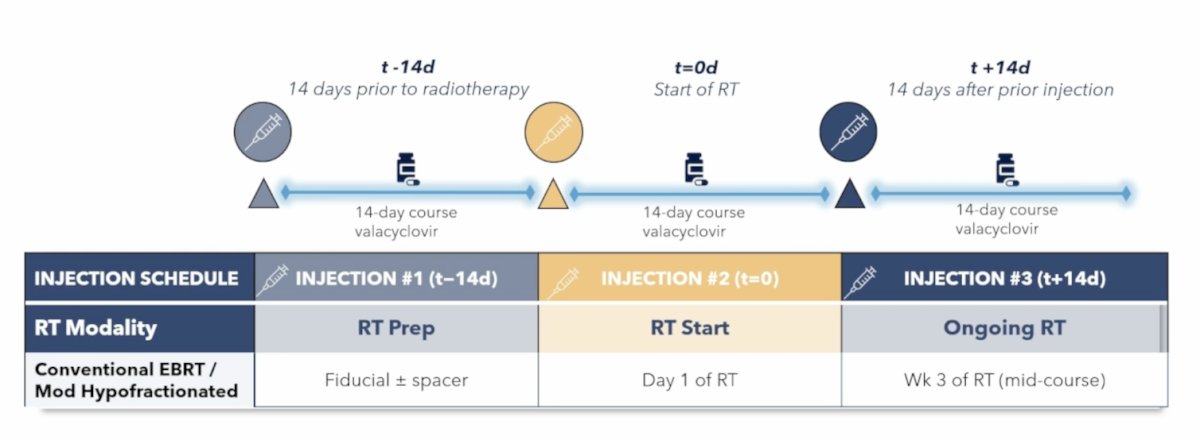
The injection and radiation sequencing schedule are as follows:
This study was a phase 3, multicenter, double-blinded, randomized, placebo-controlled clinical trial in prostate cancer patients planning to receive external beam radiation +/- short course ADT (<6 months) (NCT01436968). There were 745 patients randomized 2:1 (496 in Aglatimagene + valacyclovir and 249 in placebo + valacyclovir) and stratified by NCCN risk group and ADT use. The trial design is as follows:
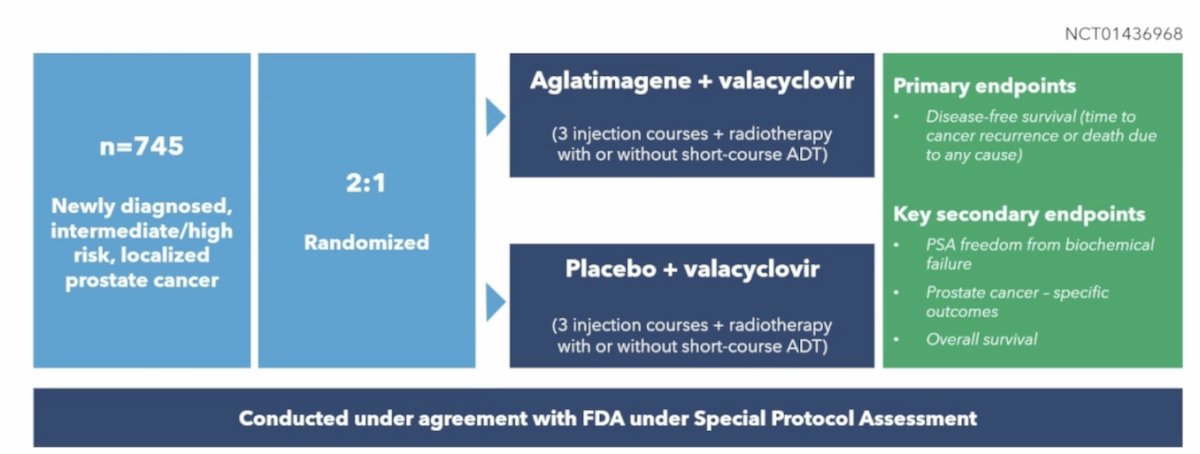
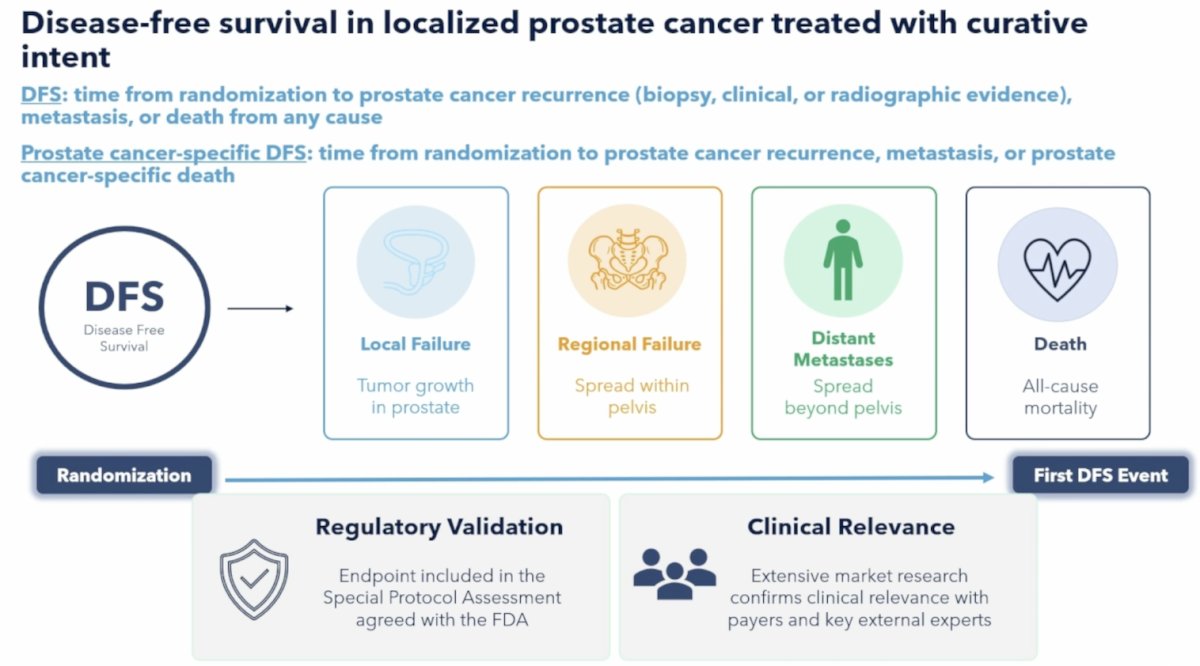
The primary endpoint was disease free survival (time to cancer recurrence or death due to any cause):
The baseline characteristics of randomized patients were well balanced between the two groups:
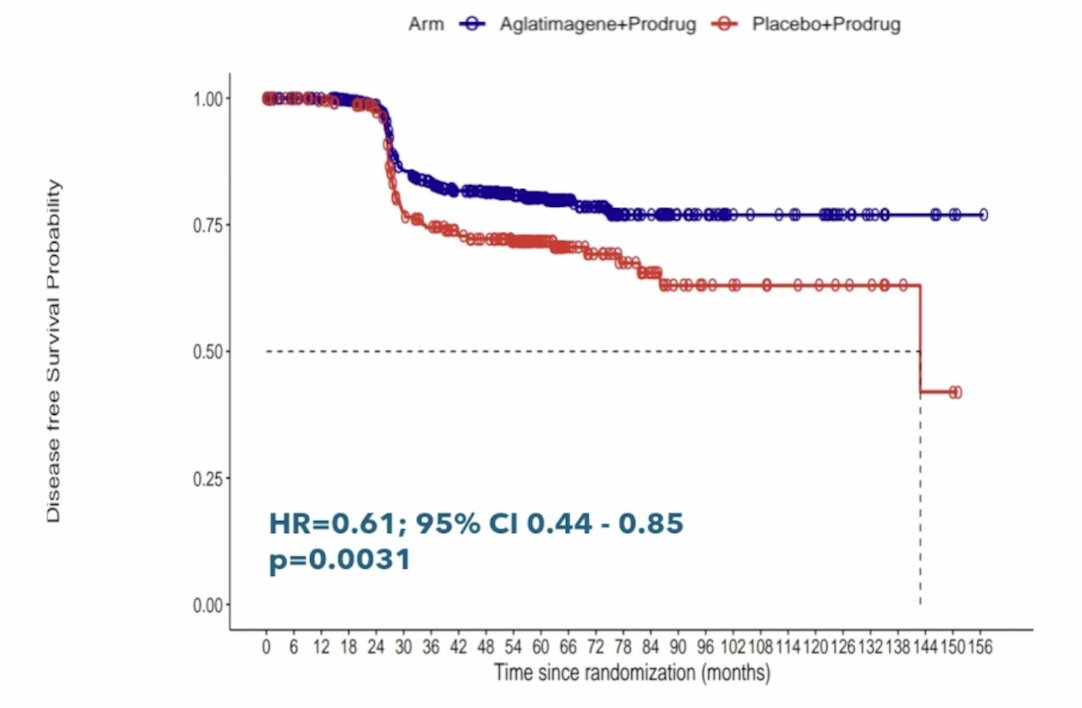
After a median follow-up of 58.0 months (95% CI 56.6 to 60.2), treatment with aglatimagene significantly reduced the risk of prostate cancer recurrence or death by 39% (HR 0.61, 95% CI 0.44 to 0.85):
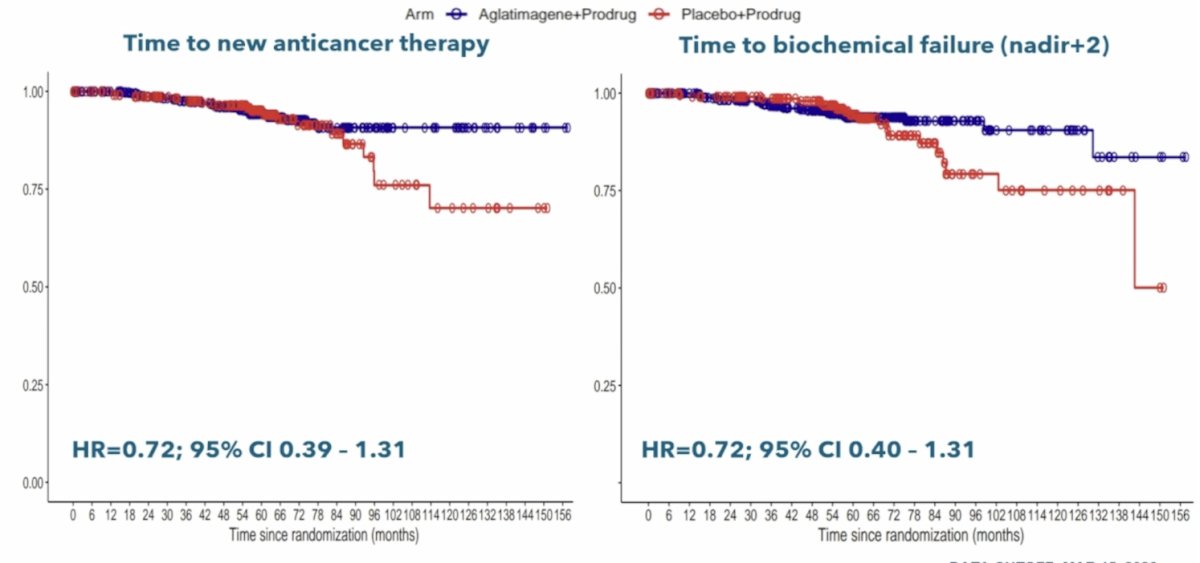
Additionally, there was a longer time to salvage anticancer therapy (HR 0.72, 95% CI 0.39-1.31) and biochemical failure (HR 0.72, 95% CI 0.40-1.31) observed in the aglatimagene arm:
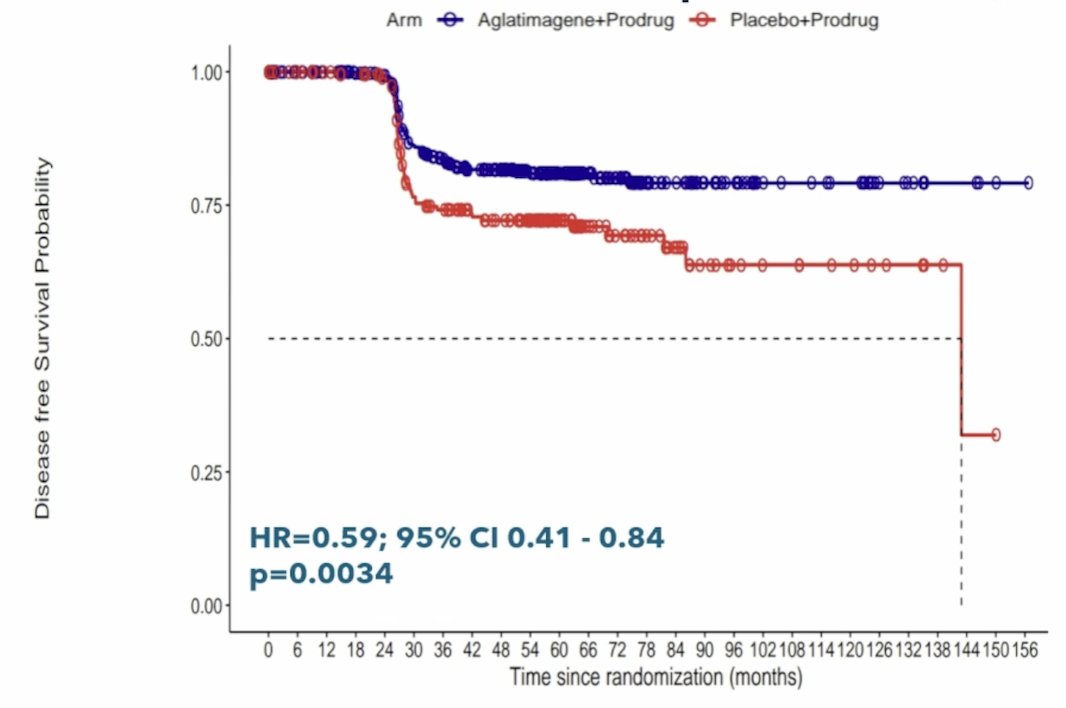
In intermediate risk prostate cancer patients, treatment with aglatimagene significantly reduced the risk of prostate cancer recurrence or death by 41% (HR 0.59, 95% CI 0.41 to 0.84):
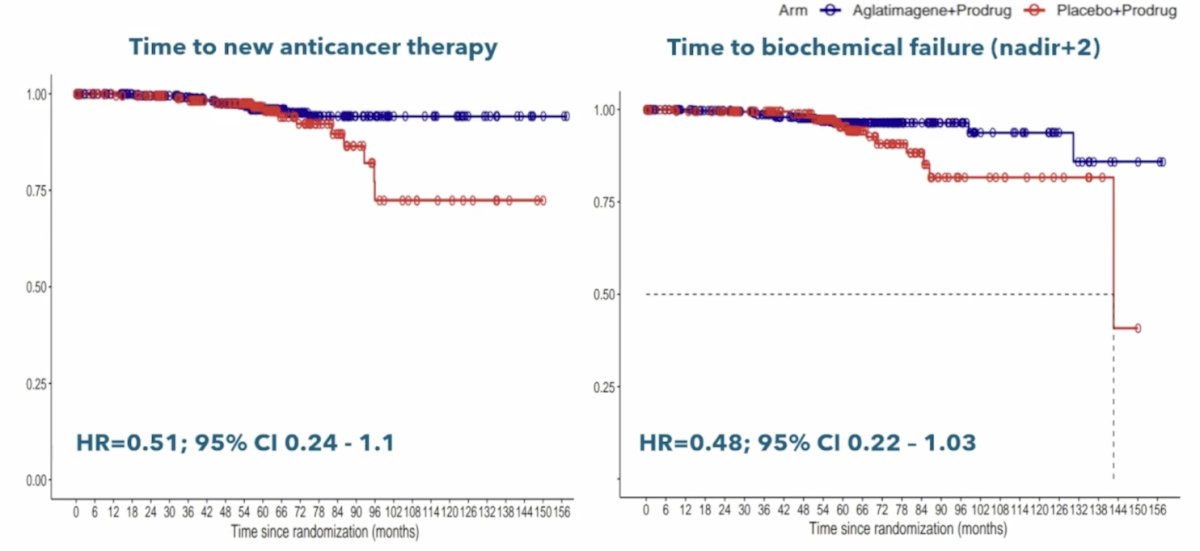
Additionally, among intermediate risk patients, there was a longer time to salvage anticancer therapy (HR 0.51, 95% CI 0.24 – 1.10) and biochemical failure (HR 0.48, 95% CI 0.22-1.03) observed in the aglatimagene arm:
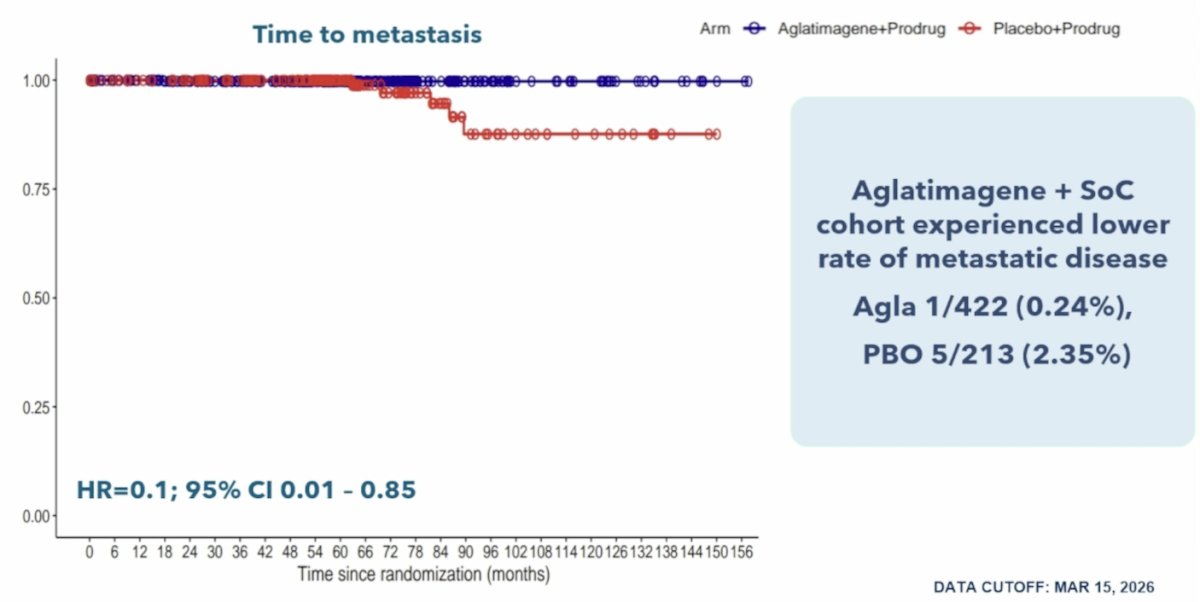
Importantly, there was a lower incidence of and increased time to metastases (HR 0.10, 95% CI 0.01-0.85) observed in the aglatimagene arm in intermediate risk prostate cancer:
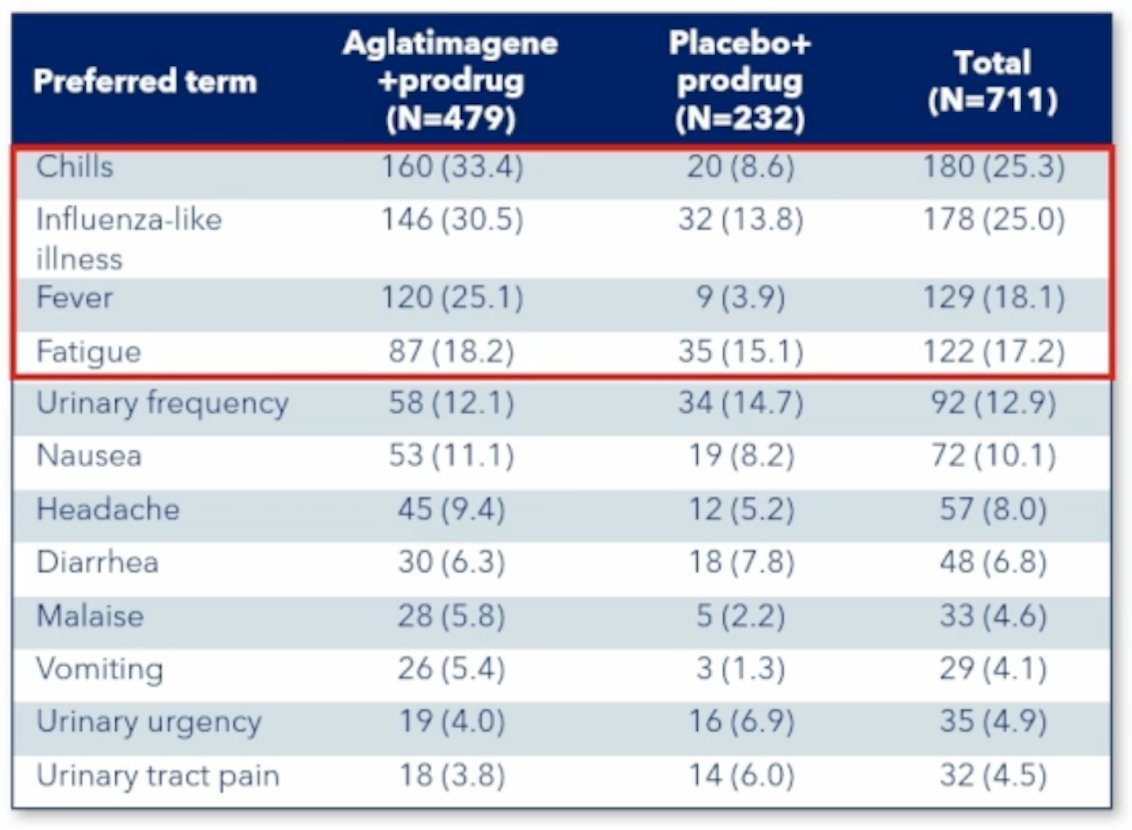
Aglatimagene in combination with standard of care radiation +/- ADT was generally well tolerated – there were no grade 4+ treatment related adverse events, lower serious adverse events in the aglatimagene arm (5.8% versus 7.3%), and comparable rates of discontinuation secondary to adverse events (5.4% versus 6.0%). Chills, fever, and flu-like symptoms were commonly mild to moderate, and self limited: > 90% of fever, flu-like symptoms, chills, and fatigue resolved within 24-72 hours. Most treatment related adverse events were grade 1-2, and grade 3 treatment related adverse events occurred in <5% of patients:
Dr. Garzotto concluded his presentation discussing extended follow-up of patients treated with aglatimagene + prodrug in combination with standard of care external beam radiotherapy in men with localized prostate cancer with the following take home points:
- The previously presented primary endpoint demonstrated statistically significant improvement in disease free survival, as well as increased pathological complete response in 2-year biopsies, known to be predictive of subsequent biochemical failure and metastasis after 10+ years of follow-up
- Consistent with these earlier findings, extended follow-up demonstrated delayed biochemical failure, metastatic disease, and salvage anticancer therapy in the aglatimagene arm versus placebo
- Clinical outcomes were associated with an acceptable tolerability profile to date
- If approved, aglatimagene could offer a new treatment option that may extend the time men live free from prostate cancer recurrence
Presented by: Mark Garzotto, MD, Oregon Health Sciences University, Portland, OR
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.