(UroToday.com) During a plenary session at the American Urological Association Annual Meeting 2026, Dr. Sara M. Lenherr delivered a State-of-the-Art lecture highlighting multiple available catheter technologies and emerging innovations in urinary drainage.
BRIEF HISTORY OF URETHRAL CATHETERIZATIONShe began by framing the current landscape of urinary drainage technologies, emphasizing that despite a 3,000-year history dating back to ancient China and Pompeii, contemporary clinical practice remains heavily tethered to foundational designs developed nearly a century ago. While historical artifacts such as the silver “Franklin Catheter” (Figure 1) were engineered for episodic urinary retention, it was Dr. Frederick Foley’s 1935 introduction of the latex self-retaining balloon catheter that standardized continuous bladder drainage.

Figure 1. The Franklin Catheter.1
To further engage the audience, she cited Dr. Ralph R. Landes: “There is little doubt that the catheter is the most valuable single instrument in the urologist’s armamentarium”.
CURRENT PROBLEMS AND EMERGING SOLUTIONSShe emphasized that systematic data continue to underscore the significant clinical limitations of these traditional models, presenting a landmark meta-analysis in which Hollingsworth and Saint quantified the high prevalence of non-infectious complications associated with chronic indwelling catheter use, defined as catheter placement extending beyond three weeks (Figure 2).
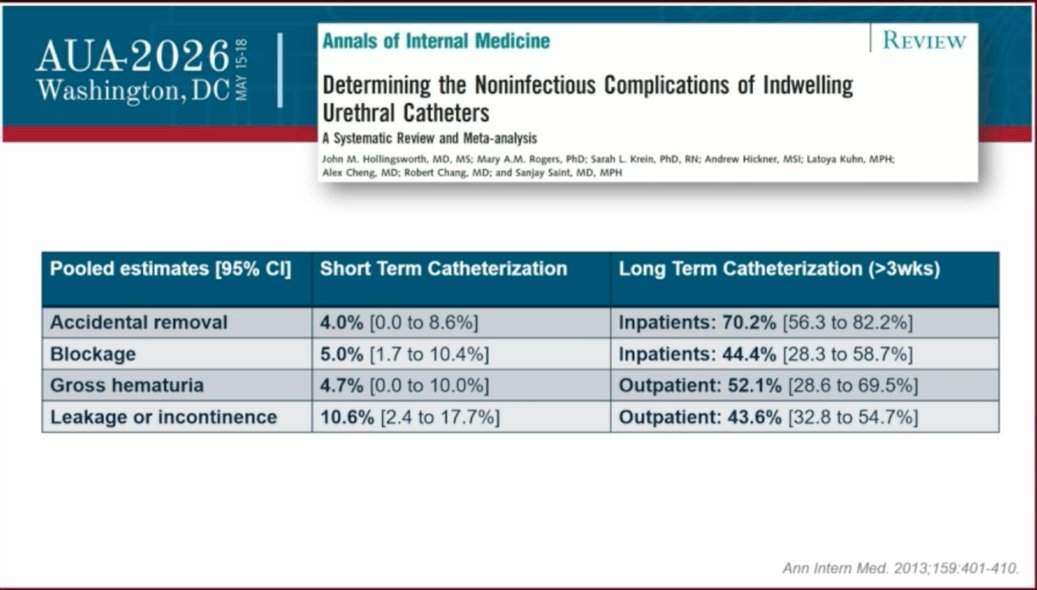
Figure 2. Determining the noninfectious complications of indwelling urethral catheters.2
These non-infectious complications generate substantial nursing burdens and patient dissatisfaction. Dr. Lenherr emphasized that the root cause of many mechanical failures is bladder mucosal suction, where suction forces cause the bladder wall to collapse directly into the drainage eyelets, leading to localized microtrauma, painful bladder spasms, and flow obstruction.
To overcome these structural design limitations, Dr. Lenherr highlighted four distinct FDA-approved technological innovations aimed at improving patient quality of life, material science, and procedural safety. She underscored that many additional innovations are attempting to reach physicians and patients, although adoption in routine clinical practice remains limited.
CATHETER INNOVATIONS1. Problem → Suction of the bladder wall // Solution → Duette/TruCath Duo (Figure 3)
- Category: Mechanical interface redesign.
- Mechanics: Engineered with a distinct dual-balloon architecture. A second, distal balloon is strategically positioned directly at the tip of the catheter, completely subsuming the tip profile.
- Key Characteristics: This dual-balloon setup places the raw drainage holes between the two cushioned balloons. This prevents the bladder wall mucosa from physically making contact with or aspirating into the drainage eyelets, significantly decreasing bladder spasms, bleeding, and intermittent flow disruptions.

Figure 3. Duette/TruCath Duo. From: https://www.poiesismedical.com/medical-device-company-duette.
2. Problem → Bladder cycling and catheter design // Solution → MiniSPC® Button by Advanced Medical Technology (Figure 4)
- Category: Catheter alternative, low-profile suprapubic catheter.
- Mechanics: Modeled directly after the low-profile “Mickey buttons” utilized by pediatric gastroenterologists for gastric feeding, this device sits flush against the skin of the suprapubic tract. It incorporates a subsumed drainage eyelet to prevent mucosal suction.
- Key Characteristics: The device utilizes a completely detachable drainage set to enable episodic bladder draining and natural bladder cycling. This design removes the need for long external tubing or cumbersome catheter plugs that are notoriously difficult to manipulate. It is exchanged monthly by a provider.

Figure 4. MiniSPC® Button by Advanced Medical Technology From: https://www.appliedmedical.net/enteral/minispc-button.
3. Problem → Eyelet obstruction // Solution → Luja by Coloplast (Figure 5)
- Category: Flow-dynamics redesign (Intermittent Catheter).
- Mechanics: Replaces the standard two-eyelet design with advanced Micro-hole Zone Technology, which incorporates over 80 individual drainage holes distributed across the body of the catheter tip.
- Key Characteristics: The highly distributed drainage field ensures continuous drainage. This dynamic eliminates the need for patients to rotate, twist, or prematurely pull back the catheter mid-void to re-establish flow, resulting in more complete bladder emptying, lower post-void residual volume, and minimized friction-induced microtrauma.

Figure 5. Luja catheter by Coloplast. From https://products.coloplast.us/global/luja/?srsltid=AfmBOoplDPa7UkXGotPrI8Cre3DPElzmVMTu38akg3YreBbgT_AQGg-N.
4. Problem → Encrustation // Solution → SILQ/ClearTract (Figure 6)
- Category: Surface science/antifouling Foley.
- Mechanics: The silicone surface of the catheter is molecularly engineered with a highly advanced, non-leaching zwitterionic-coated surface. This creates a permanent, dense hydration layer of water molecules tightly bound to the device material.
- Key Characteristics: Instead of relying on traditional silver coatings that chemically leach to kill bacteria, this material uses a passive anti-fouling strategy. The hydration layer makes the surface too slick for proteins, bacteria, or crystalline matrices to adhere to, directly interrupting the initial step of biofilm formation, chronic bacterial colonization, and subsequent catheter encrustation.

Figure 6. SILQ/ClearTract catheter.
Dr. Lenherr highlighted three additional categories that represent a major departure from traditional urological management models:
1. Injury Prevention: Egress by InnoCare (Figure 7)
- Category: Mechanical safety Foley.
- Mechanics: This represents the first device approved under the FDA’s new expedited classification for “urinary catheters with additional safety features.” It features an internal pressure-relief mechanism built into the inflation line.
- Key Characteristics: In the event of sudden traumatic pulling or accidental extraction, the internal valve detects the rapid spike in pressure and automatically deflates the retention balloon before it can be forcibly dragged through the bladder neck or urethra, mitigating severe lower urinary tract tearing and hemorrhage.
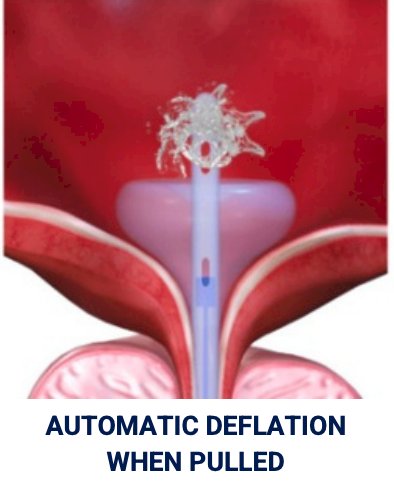
Figure 7. Automatic deflation of the Egress catheter. From: https://innocareurologics.com/resources.
2. The Paradigm Shift: InFlow by Vesiflo (Figure 8)
- Category: Catheter alternative, active bladder drainage prosthesis.
- Mechanics: Classified as a Class II urethral insert, this female-only device places a miniature, non-thermal internal valve-pump completely inside the urethra.
- Key Characteristics: It bypasses the need for an external collection bag entirely, serving as a mechanical alternative to intermittent or indwelling catheterization. To void, the patient sits on the toilet and holds a handheld magnetic remote control over the lower abdomen, which remotely activates the miniature internal pump to actively evacuate the bladder and mimic physiologic voiding. It needs to be exchanged monthly by a provider.
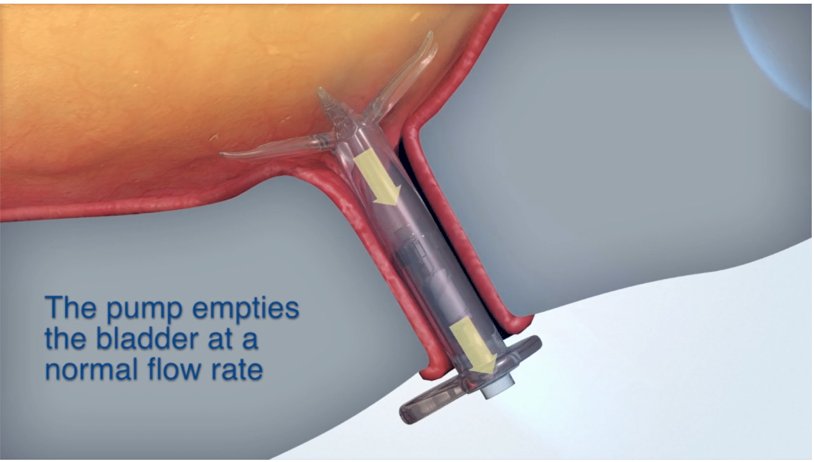
Figure 8. InFlow catheter. From: https://vesiflo.com/how-is-the-inflow-used/.
3. Environmental Sustainability: Aurie System (Figure 9)
- Category: FDA-approved, reusable intermittent catheter system.
- Mechanics: Developed to directly combat the massive volume of non-recyclable medical plastic waste generated by clean intermittent catheterization (CIC), this system consists of an FDA-approved, resilient, 100-times reusable no-touch intermittent catheter and a specialized portable docking case.
- Key Characteristics: After a voiding session, the patient inserts the reusable catheter into the compact storage container. The case automatically initiates a 36-minute high-level chemical disinfection cycle that leaves the catheter sterile and ready for subsequent use, mirroring the automated standards utilized to sanitize reusable surgical cystoscopes.
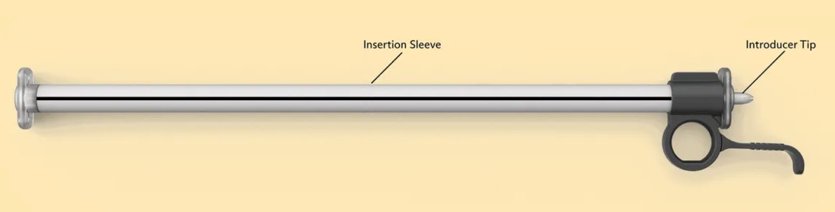

Figure 9. Aurie system. From: https://www.livewithaurie.com/.
Dr. Lenherr closed her presentation by calling on urologists and industrial engineers to actively look beyond basic Foley catheter options. As the clinical need for long-term urinary management in aging, neurogenic, and frail populations continues to rise, she emphasized that targeted advancements in catheter design represent a fundamental medical necessity to optimize patient quality of life while limiting healthcare expenditures.
She finalized saying: “What is your wishlist, and what are the problems that you identify in your patients with chronic catheter use?”
Presented by: Sarah M. Lenherr, MD, MS, URPS. Associate Professor and Urology Program Director, Department of Urology, University of Utah Health. Salt Lake City, UT.
Written by: Jonathan Badin-Castro, MD. Endourology and Minimally Invasive Surgery Fellow, Department of Urology, University of California, Irvine. @JonBadin on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:- Huth EJ. Benjamin Franklin’s place in the history of medicine. J R Soc Med. 2007;100(11):534-538. doi:10.1177/014107680710001116
- Lenherr SM. State-of-the-Art Lecture: New Developments in Urinary Catheters. Presented at: 2026 American Urological Association (AUA) Annual Meeting; May 17, 2026; Washington, DC.