(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a poster presentation by Dr. Akihiro Kumono and colleagues from Tokyo Women’s Medical University evaluating the association between serum kidney injury molecule-1 (KIM-1) levels and treatment response and survival in patients with metastatic renal cell carcinoma (mRCC).
Immune checkpoint inhibitor-based combinations, including dual immune checkpoint blockade (IO–IO) and immune checkpoint inhibitor plus tyrosine kinase inhibitor (IO–TKI) regimens, have substantially improved outcomes in metastatic RCC. However, robust predictive biomarkers that can identify patients more likely to respond to therapy remain lacking. Kidney injury molecule-1 (KIM-1), a marker of proximal tubular injury that is detectable in peripheral blood and highly expressed in RCC tissue, has emerged as a promising biomarker associated with tumor aggressiveness and prognosis.
The investigators retrospectively analyzed 73 patients with mRCC treated with first-line IO-based combination therapy between 2018 and 2024. Thirty-six patients received IO–IO therapy, and 37 received IO–TKI therapy. Baseline serum KIM-1 levels were dichotomized into high versus low/intermediate groups, and associations with best overall response, progression-free survival (PFS), and overall survival (OS) were evaluated using Kaplan–Meier and Cox regression analyses. In a subset of 63 patients, early on-treatment KIM-1 changes from baseline to 3 weeks were also assessed.
The study cohort had a median age of 70 years (range 34–86), and 77% were male. IMDC risk classification was favorable in 4%, intermediate in 56%, and poor in 39%. Histologies were predominantly clear cell RCC (66%), with additional papillary, chromophobe, TFE3-rearranged, collecting duct, SDHB-deficient, and unclassified subtypes represented. Median serum KIM-1 was 134.3 pg/mL, and the median follow-up was 17 months.
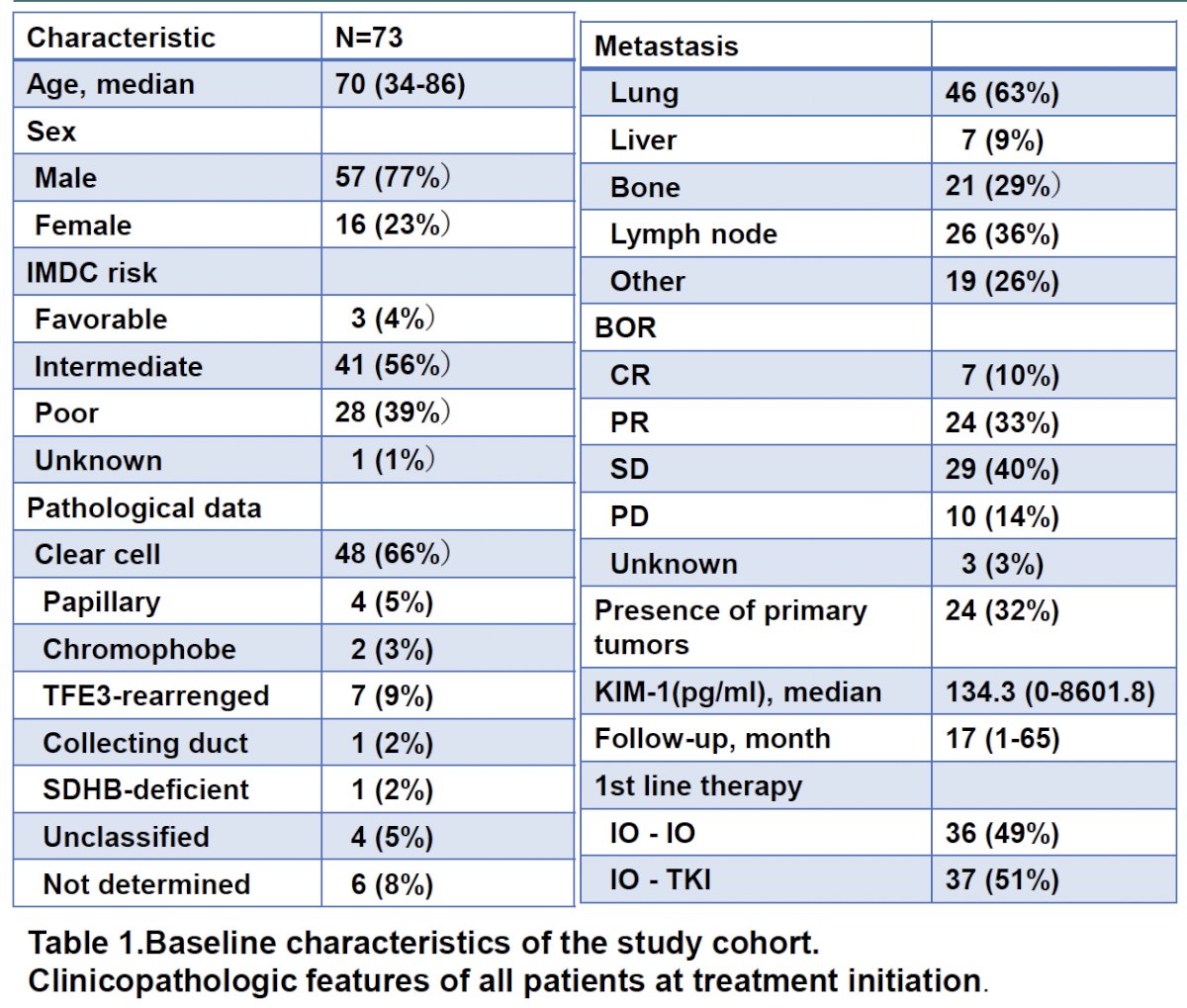
Overall best responses included complete response in 7 patients (10%), partial response in 24 (33%), stable disease in 29 (40%), and progressive disease in 10 (14%), corresponding to an objective response rate of 43% and a disease control rate of 83%.
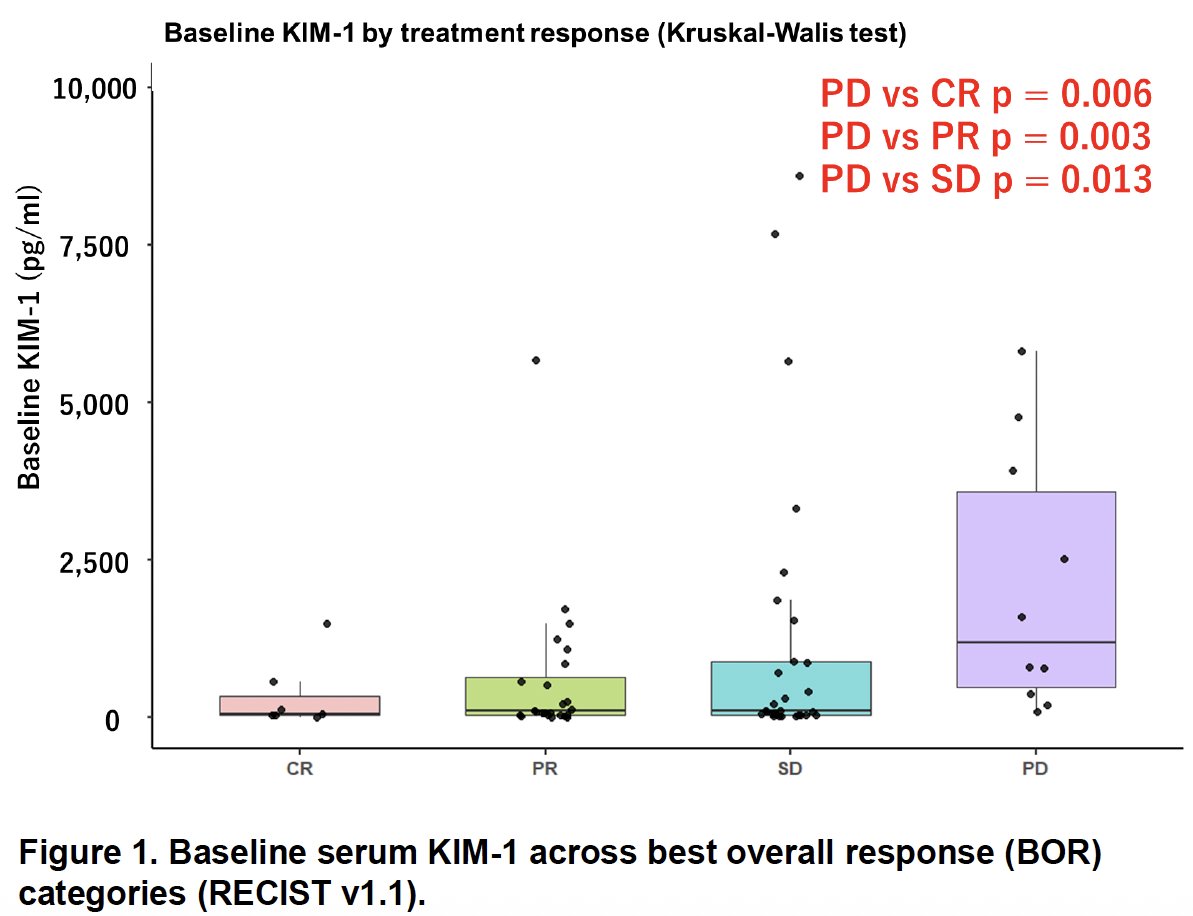
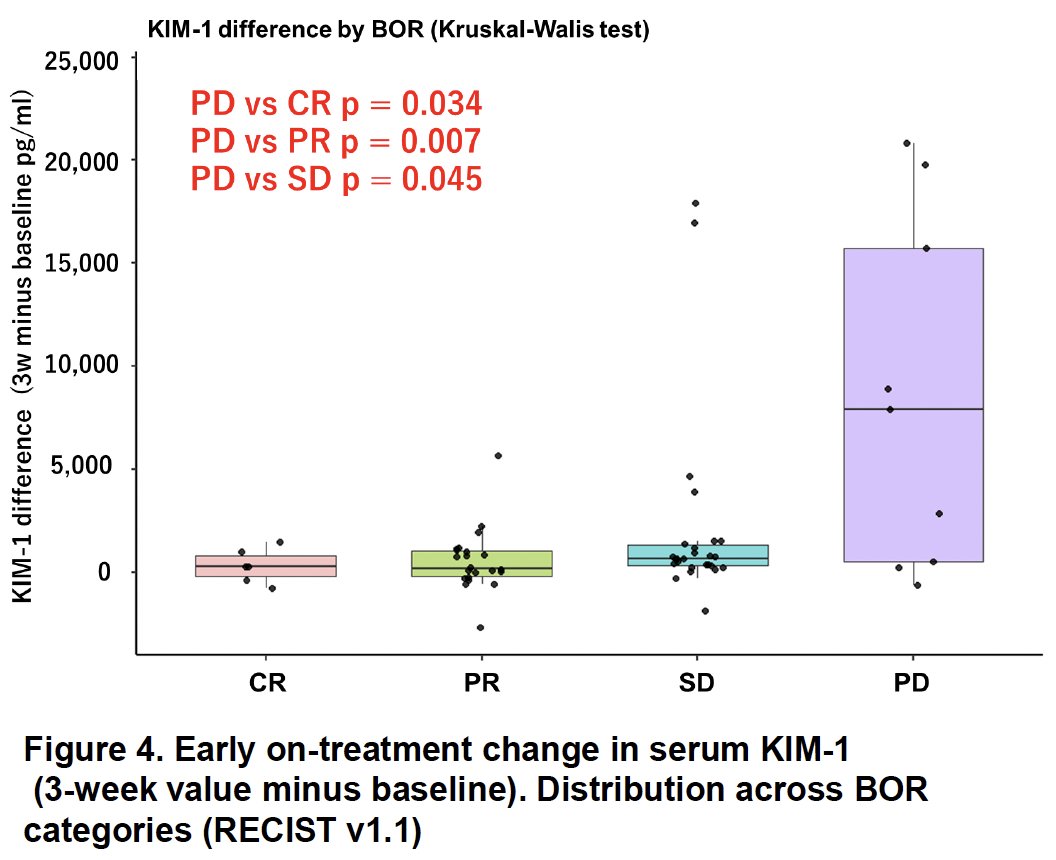
The figure above demonstrates a clear association between higher baseline serum KIM-1 levels and poorer treatment response. Median KIM-1 values were significantly higher among patients with progressive disease compared with complete response (p=0.006), partial response (p=0.003), and stable disease (p=0.013). These findings suggest that elevated baseline KIM-1 identifies patients with biologically more aggressive tumors and a lower likelihood of response to first-line IO-based therapy.
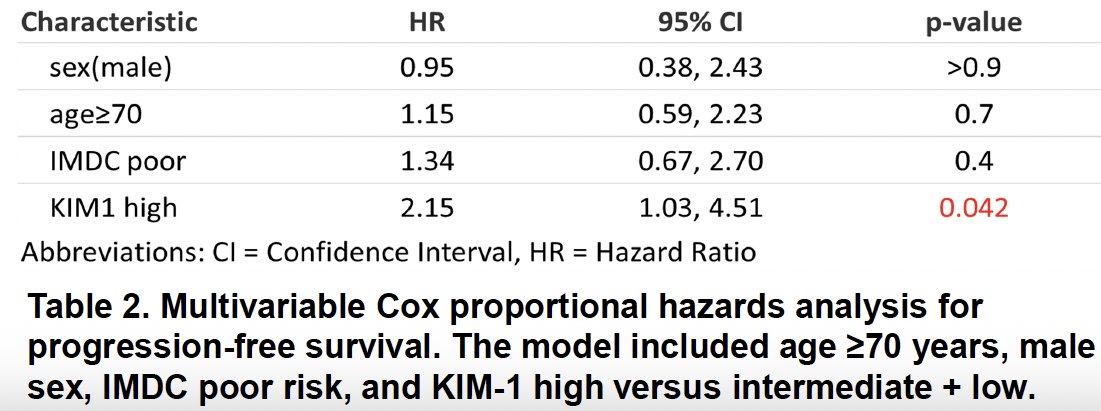
The progression-free survival analysis further supported the prognostic value of KIM-1. In the Kaplan–Meier curves, patients with high baseline KIM-1 had significantly shorter PFS compared with those in the low/intermediate group (log-rank p=0.009). In multivariable Cox regression adjusting for age ≥70 years, sex, IMDC poor risk, and treatment type (IO–IO versus IO–TKI), high KIM-1 remained an independent predictor of progression, with a hazard ratio of 2.15 (95% CI 1.03–4.51; p=0.042). Thus, patients with elevated baseline KIM-1 had more than twice the risk of disease progression.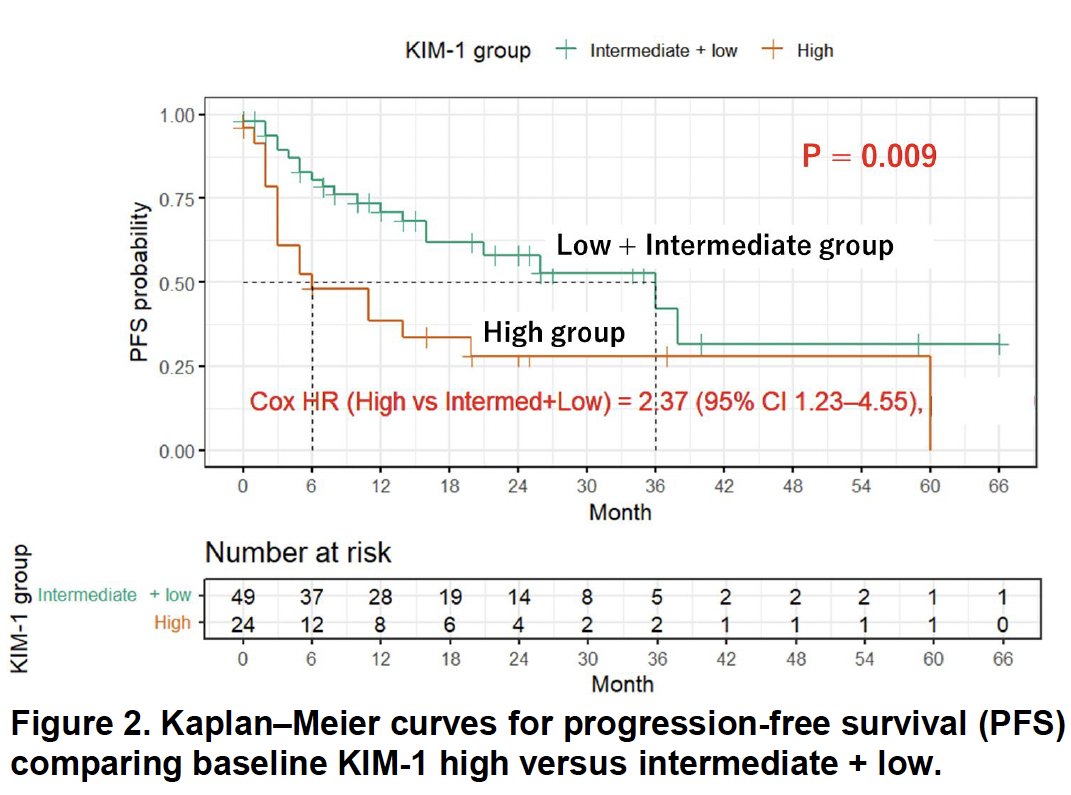
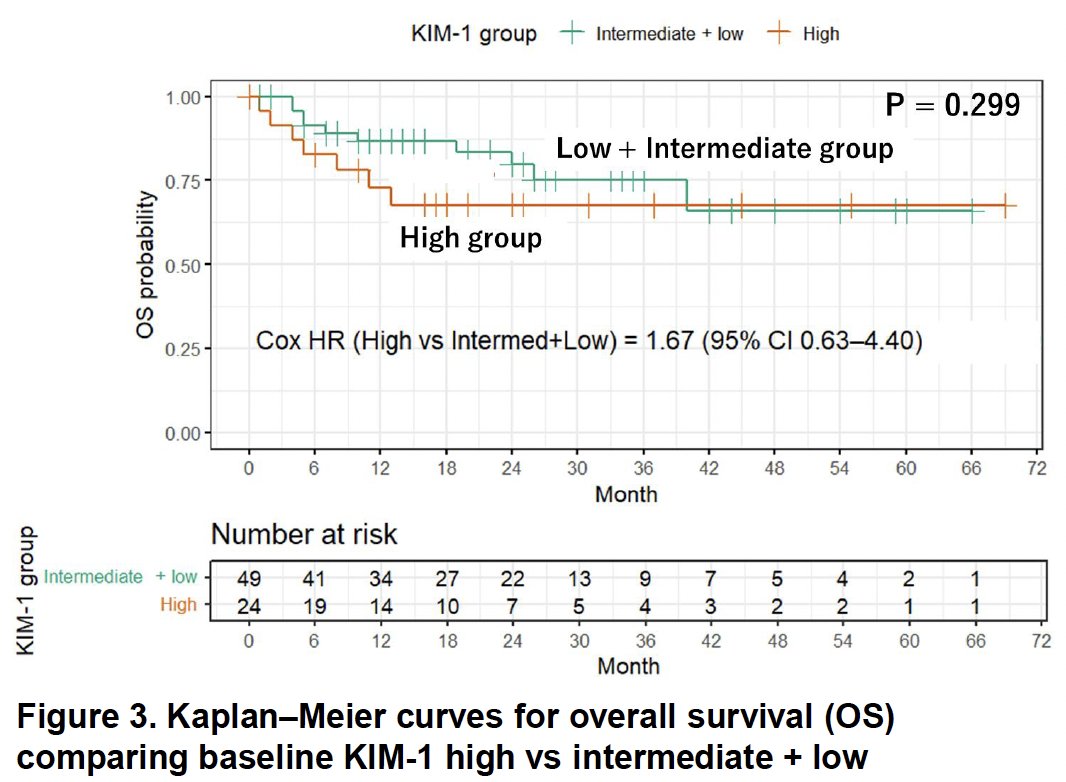
In contrast, baseline KIM-1 was not significantly associated with overall survival. The Kaplan–Meier curves for OS were largely overlapping, with a log-rank p value of 0.299.
The investigators also examined whether early changes in serum KIM-1 after treatment initiation could serve as a dynamic biomarker. Figure 4 demonstrated that increases in KIM-1 over the first three weeks were more pronounced among patients with progressive disease compared with complete response (p=0.034), partial response (p=0.007), and stable disease (p=0.045).
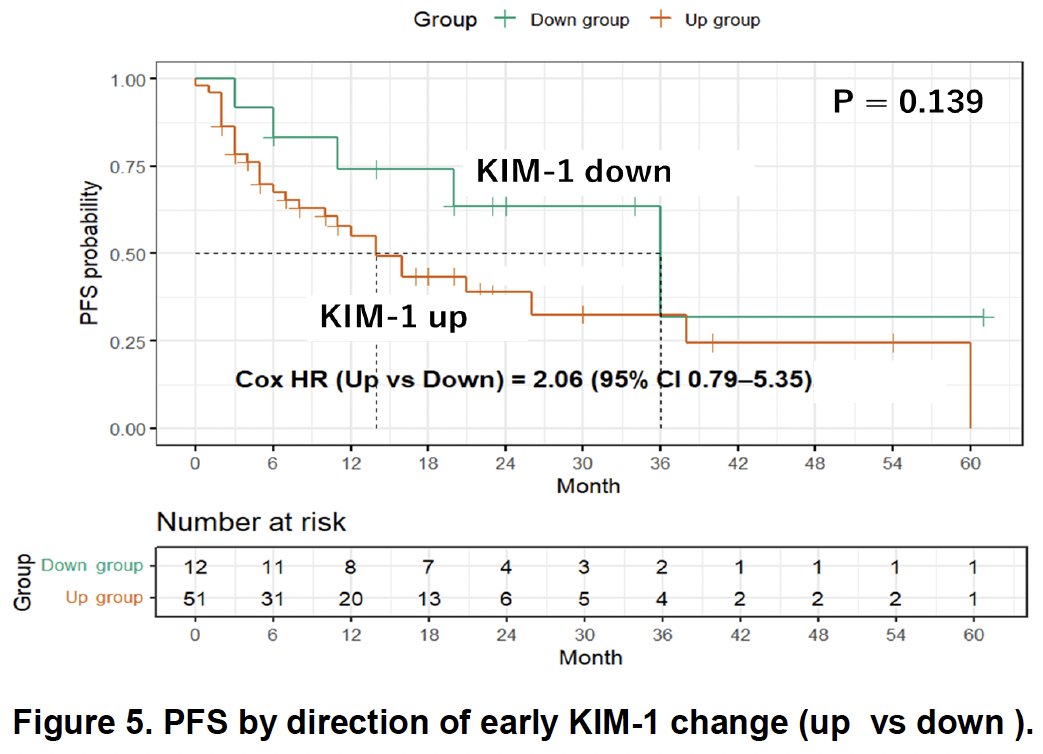
However, when patients were dichotomized according to whether KIM-1 increased or decreased, no significant difference in PFS was observed (HR 2.06, 95% CI 0.79–5.35; p=0.139).
The investigators concluded that serum KIM-1 may serve as a predictive biomarker for treatment response and prognosis in metastatic RCC. Elevated baseline KIM-1 was associated with lower response rates and significantly shorter progression-free survival, whereas early on-treatment changes did not independently predict clinical outcomes.
These findings add to the growing literature supporting circulating KIM-1 as a promising blood-based biomarker in RCC. If validated in larger prospective cohorts and correlated with tumor tissue expression, serum KIM-1 could help refine risk stratification and guide therapeutic decision-making for patients with metastatic RCC.
Presented by: Akihiro Kumono, MD, Department of Urology, Tokyo Women’s Medical University, Tokyo, Japan
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.