(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a poster presentation by Dr. Kazuhiko Yoshida and colleagues from Tokyo Women’s Medical University comparing immune checkpoint inhibitor plus immune checkpoint inhibitor (IO–IO) and immune checkpoint inhibitor plus tyrosine kinase inhibitor (IO–TKI) combination therapies in patients with advanced renal cell carcinoma (RCC) and inferior vena cava (IVC) tumor thrombus.
RCC with extension into the IVC represents one of the most technically and biologically challenging presentations of advanced kidney cancer. While immune checkpoint inhibitor–based combinations have become standard first-line therapy for advanced RCC, data regarding their activity against both the primary renal mass and associated vena caval tumor thrombus remain limited. The investigators therefore sought to compare the efficacy, safety, surgical outcomes, and survival associated with IO–IO and IO–TKI strategies in this unique clinical setting.
This retrospective, two-center study included 46 patients with advanced RCC and IVC tumor thrombi treated with IO-based combination therapy. Fifteen patients received IO–IO therapy, consisting exclusively of nivolumab plus ipilimumab, while 31 received IO–TKI therapy, including pembrolizumab plus axitinib (13%), avelumab plus axitinib (3%), nivolumab plus cabozantinib (29%), and pembrolizumab plus lenvatinib (55%).
Baseline characteristics were generally similar, although patients receiving IO–TKI were older (median age 72 versus 62 years, p=0.035) and more likely to have right-sided tumors (87% versus 60%, p=0.037). Most patients had poor-risk disease by IMDC criteria (58–67%), and nearly all had advanced thrombus extension, with level III–IV IVC tumor thrombi in 60% of the IO–IO group and 48% of the IO–TKI group.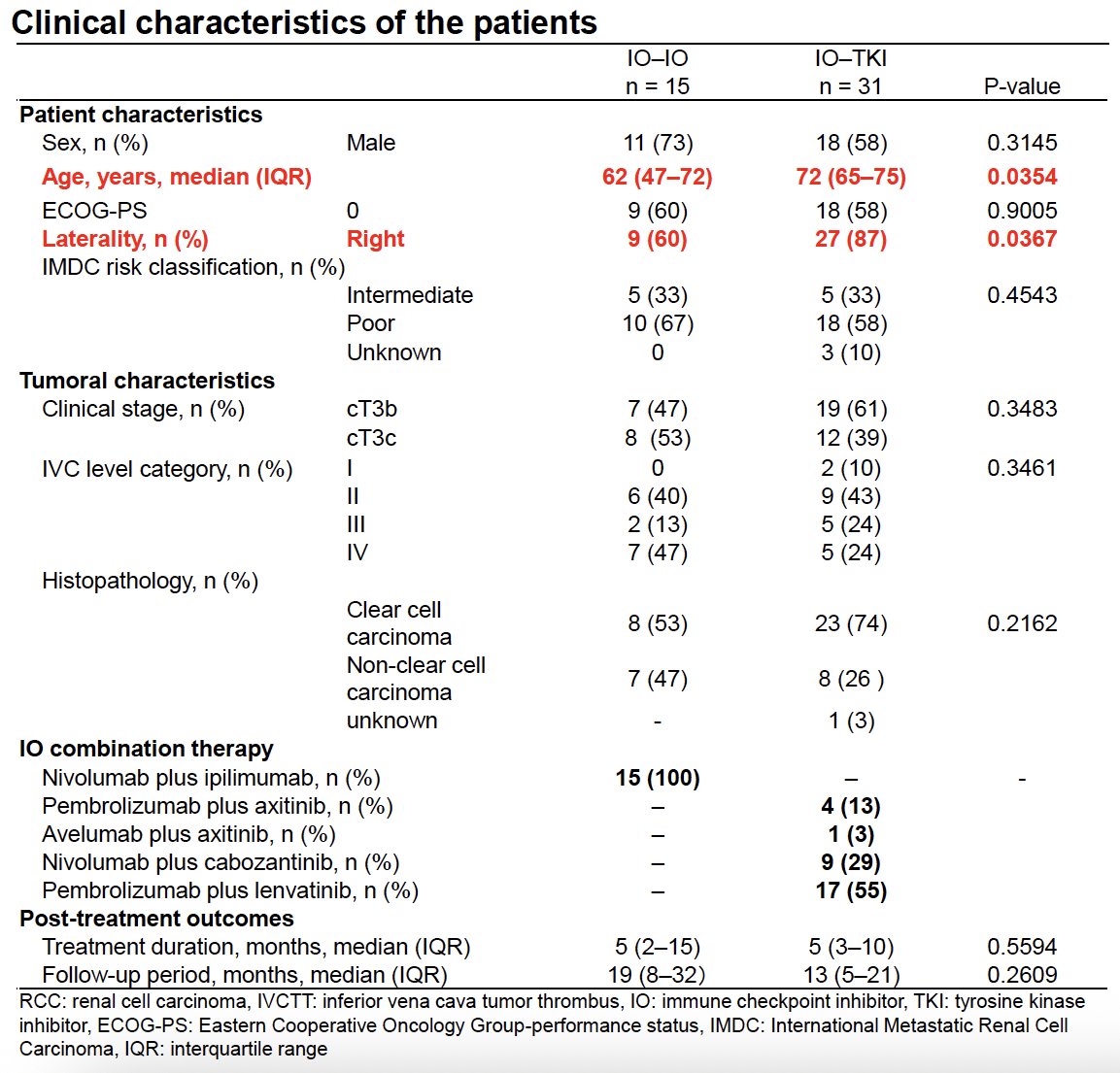
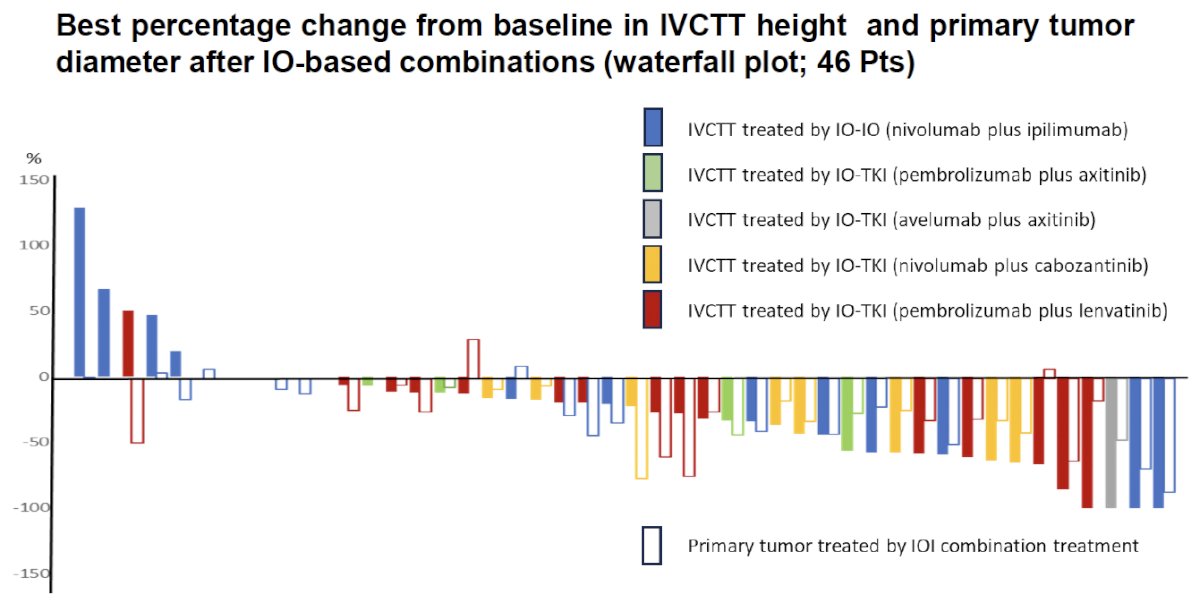
The waterfall plot demonstrated clinically meaningful shrinkage of both the primary tumor and the vena cava thrombus across treatment groups. The majority of bars fell below zero, indicating a reduction in tumor burden, with more pronounced and more frequent decreases observed among patients treated with IO–TKI regimens.
For the primary renal tumor, any tumor shrinkage was observed in 87% of patients treated with IO–TKI compared with 53% receiving IO–IO (p=0.0118). Median reduction in primary tumor diameter was numerically greater with IO–TKI (26% versus 16%), although this difference was not statistically significant (p=0.43). Time to best primary tumor response was shorter with IO–TKI (3 versus 6 months).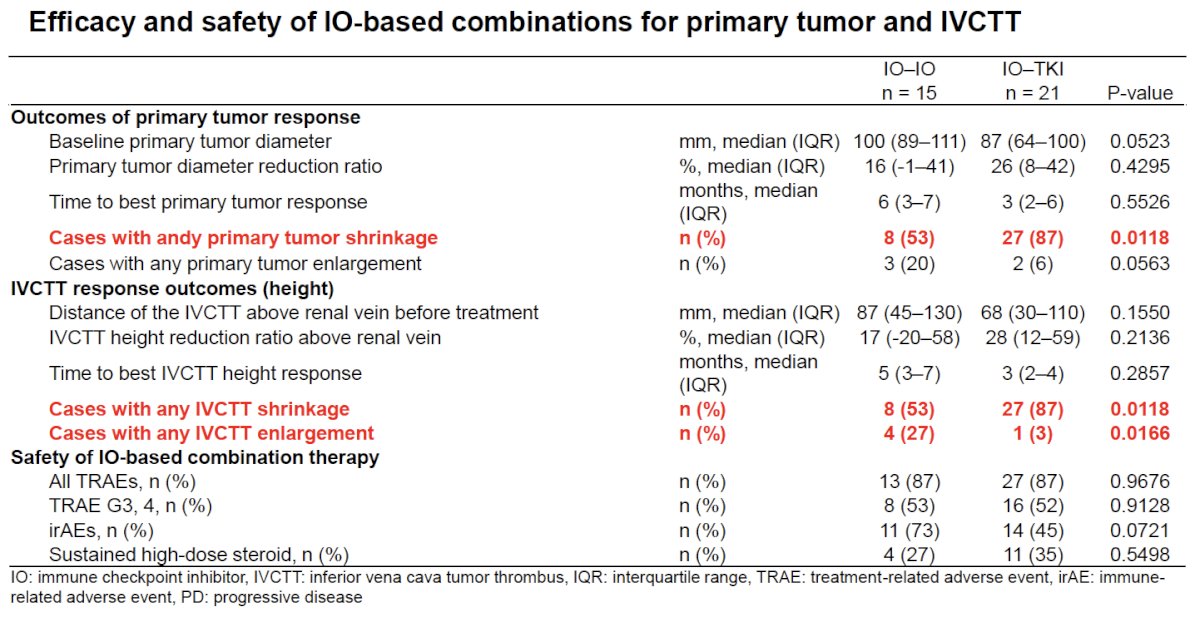
A similar pattern was observed for thrombus response. Any reduction in IVCTT height occurred in 87% of patients treated with IO–TKI compared with 53% receiving IO–IO (p=0.0118). Conversely, thrombus enlargement was significantly less common with IO–TKI (3% versus 27%, p=0.0166). Median reduction in thrombus height was 28% versus 17%, respectively, with median time to best response of 3 versus 5 months.
Safety profiles were remarkably similar between treatment strategies. Any treatment-related adverse event (TRAE) occurred in 87% of patients in both groups, and grade 3–4 TRAEs were reported in 52–53%. Immune-related adverse events were numerically more common with IO–IO (73% versus 45%, p=0.072), while sustained high-dose steroid use occurred in 27% and 35%, respectively.
Deferred cytoreductive nephrectomy was performed in nearly half of patients in both groups: 47% after IO–IO and 45% after IO–TKI. Surgical outcomes were broadly comparable. Median operative time was 271 versus 259 minutes, estimated blood loss was 1,280 versus 545 mL, and hospital stay was 9 versus 8 days for IO–IO and IO–TKI, respectively. Perioperative complications of Clavien-Dindo grade ≥2 occurred in 17% of both groups. Pathologic complete response was observed in one patient in each cohort.

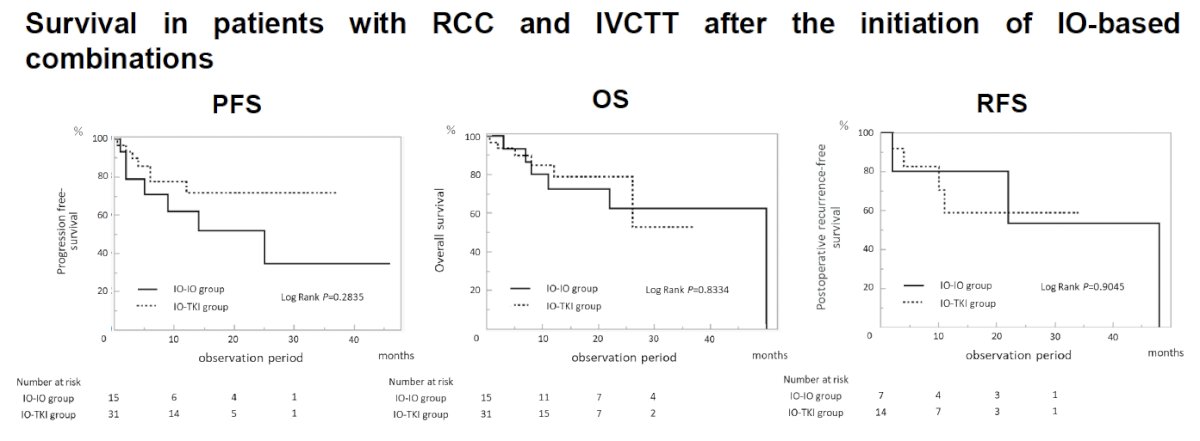
The Kaplan–Meier curves for progression-free survival (PFS), overall survival (OS), and recurrence-free survival (RFS) after surgery demonstrated overlapping trajectories, indicating no meaningful differences in long-term outcomes between IO–IO and IO–TKI approaches.
The investigators concluded that IO-based combination therapy provides clinically meaningful activity against both the primary renal tumor and IVC tumor thrombus in advanced RCC. Although IO–TKI therapy was associated with more frequent and more rapid tumor and thrombus shrinkage, overall safety, surgical outcomes, and survival were similar between IO–IO and IO–TKI regimens.
These findings suggest that both IO–IO and IO–TKI combinations are viable treatment options for selected patients with RCC and IVCTT, and treatment selection can be individualized based on patient characteristics, urgency for tumor shrinkage, and physician preference.
Presented by: Kazuhiko Yoshida, MD, PhD, Department of Urology, Tokyo Women's Medical University Hospital, Tokyo, Japan
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.