(UroToday.com) Following an insightful “kick-off” morning at AUA 2026 in beautiful Washington, D.C., attendees were treated to a truly "State-of-the-Art Lecture" by Alexander Kutikov, MD, FACS, Chair of the Department of Urology at Fox Chase Cancer Center. Dr. Kutikov, provided a comprehensive overview of the evolving landscape of renal mass management, focusing specifically on the strategic role of ablation in renal cell carcinoma (RCC).
A FRAMEWORK FOR DECISION-MAKING
Dr. Kutikov began by emphasizing that the management of a newly diagnosed, localized renal mass in an algorithmic process, rather than a binary one (Figure 1), where the treatment selection needs to be tailor-made for each specific patient, rather than just the tumor. He presented a tripartite framework for decision-making:
- Patient Risk: Factors such as age, frailty, surgical history, comorbidities, and baseline renal function.
- Tumor Risk: Size, growth kinetics, focality, and anatomical complexity.
- System Risk: Surgeon expertise and the center’s ability to manage potential complications.
These decisions should consider the balance of three treatment goals:
- Oncologic control – the topmost goal.
- Nephron preservation – when it is reasonable and justified.
- Minimize morbidity.
He underscored that there are two key treatment decisions: first, whether to observe the mass vs. treating it (Decision Point 1), and second, if treating, what is the treatment intensity (Decision Point 2)? When a treatment decision is made, it should be calibrated to each unique patient and tumor. Another incredibly accurate phrase was “tumor complexity drives destiny” for treatment selection.
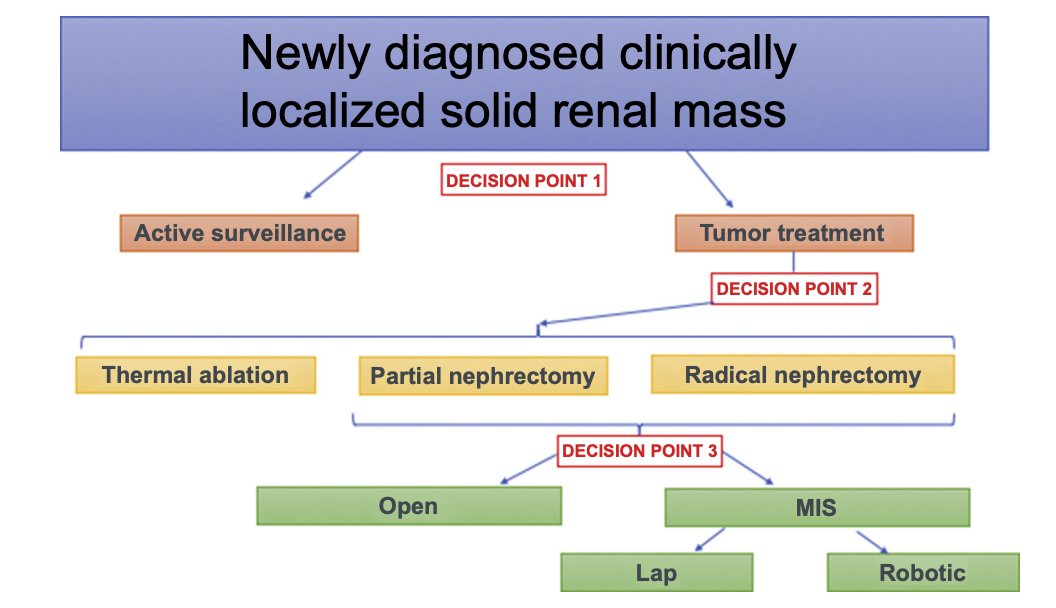
Figure 1. Key decision points in the management of newly diagnosed localized solid renal mass.1
Dr. Kutikov mentioned that ablation occupies a "middle ground" because it is “more active than surveillance but less invasive than surgery”. He also clarified that ablation is most appropriate when the clinical goal shifts from maximal control to minimal harm, particularly for elderly or comorbid patients.
However, he issued a stern warning: “Ablation is not surveillance with a billing code”. It carries real risks, including significant blood loss and "burning bridges" for future surgical interventions. He argued that complex anatomy should trigger surgical expertise (referral for a complex partial nephrectomy) rather than a default to ablation – “Ablation is not the answer for anatomically complex and larger tumors”. To illustrate this, he presented an index case referred to him where ablation was chosen due to complex anatomy; the patient subsequently presented with a locally invasive persistence of the disease requiring a radical nephrectomy.
ABLATION MODALITIESRegarding technology, Dr. Kutikov addressed the cryoablation vs. thermal ablation debate. For tumors < 3 cm, the modality is often chosen based on anatomy and expertise. However, for tumors > 3 cm or central masses, he argued that cryoablation offers superior control, visibility, and safety due to real-time ice ball visualization. He also highlighted Histotripsy as an exciting non-thermal frontier, noting the completion of the HOPE4KIDNEY trial and recent FDA submission for renal tumor indications.
DATA LIMITATIONS AND THE GOLD STANDARDDr. Kutikov emphasized that there is no meaningful prospective randomized data supporting ablation rather than only real-world outcomes. Thus, Partial Nephrectomy (PN) remains the gold standard for fit patients with cT1a masses, as it offers the most reliable oncological control and durable cancer-specific survival.
He also exemplified predictive models for treatment selection (Figure 2), underscoring that, unfortunately, these still fall short due to selection bias – “risk calculators can provide context and a jumping-off point, but not an ultimate clinical decision”.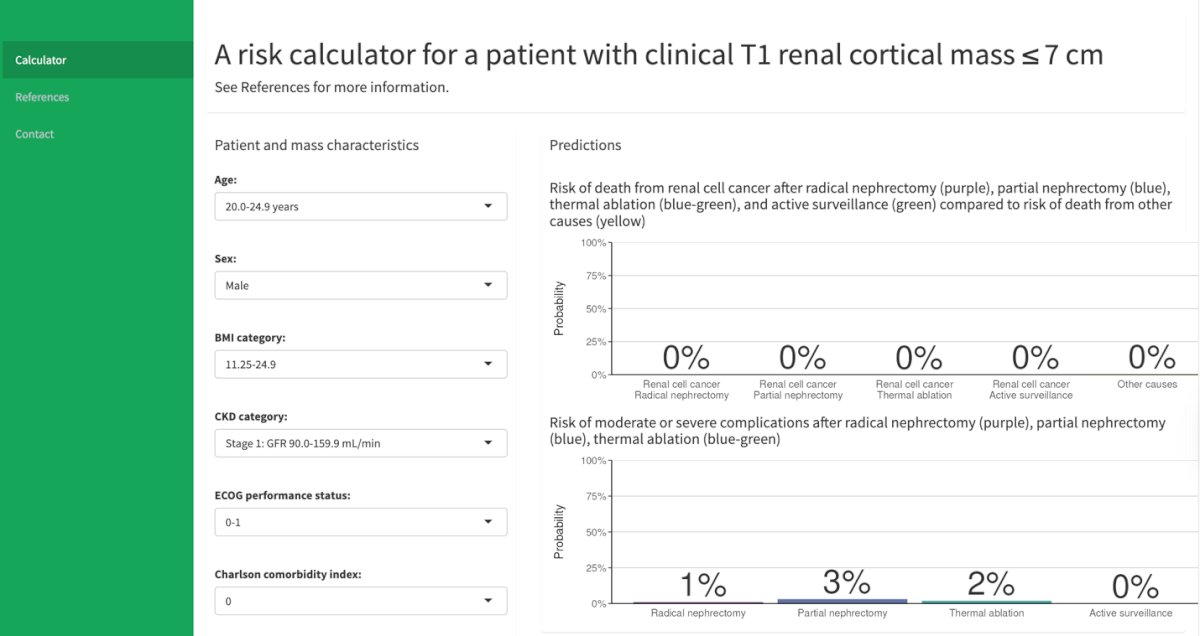
Figure 2. Small renal mass risk calculator.2, 3 https://small-renal-mass-risk-calculator.fredhutch.org/
In his concluding summary, Dr. Kutikov offered several key principles for renal mass ablation in context:
- Ablation has a clear role but is not oncologically equivalent to surgery in fit patients.
- Selection and execution drive outcomes.
- Evidence and predictive tools remain limited.
- New technologies, including histotripsy, are investigational.
- In renal mass, judgment matters – "Decisions always override incisions."
Presented by: Alexander Kutikov, MD, FACS. Chair, Department of Urology, Fox Chase Cancer Center. Philadelphia, PA.
Written by: Jonathan Badin-Castro, MD. Endourology and Minimally Invasive Surgery Fellow, Department of Urology, University of California, Irvine. @JonBadin on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:- Chandrasekar T, Boorjian SA, Capitanio U, Gershman B, Mir MC, Kutikov A. Collaborative Review: Factors Influencing Treatment Decisions for Patients with a Localized Solid Renal Mass. Eur Urol. 2021 Nov;80(5):575-588. doi: 10.1016/j.eururo.2021.01.021. Epub 2021 Feb 6. PMID: 33558091.
- Psutka SP et al., A novel clinical decision aid to support personalized treatment selection for patients with CT1 renal cortical masses: Results from a multi-institutional competing risks analysis including performance status and comorbidity. Journal of Clinical Oncology 2020;38(6_suppl):610-610. DOI: 10.1200/JCO.2020.38.6_suppl.610
- Psutka SP et al., A Clinical Decision Aid to Support Personalized Treatment Selection for Patients with Clinical T1 Renal Masses: Results from a Multi-institutional Competing-risks Analysis. European Urology. DOI: https://doi.org/10.1016/j.eururo.2021.11.002.