(UroToday.com) At the AUA 2026 meeting during a session on stone disease, David S. Goldfarb, MD, delivered a State-of-the-Art lecture which provided a comprehensive overview of the escalating intersection between climate change and renal disease, focusing specifically on how global warming and urban microclimates drive upward trends in nephrolithiasis and acute kidney injury (AKI).
THE IMPACT OF GLOBAL WARMING ON STONE PREVALENCEDr. Goldfarb opened his lecture with historical NHANES data tracking the US population prevalence of nephrolithiasis from 1976 to 2010. The numbers reveal a stark, continuous rise in adult stone prevalence, jumping from 3.2% to 8.8%, which translates to roughly 19.2 million affected US adults. This expanding clinical challenge is mirrored across global datasets from Japan, Germany, and Brazil.
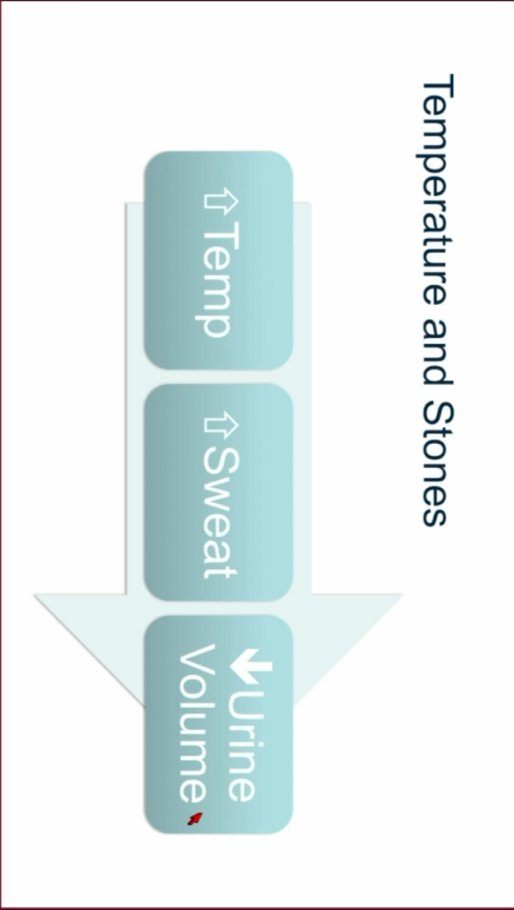
Figure 1. Relationship between temperature and stones.1
While stone disease is increasingly recognized as a chronic metabolic entity, with common contributors including rising rates of obesity, metabolic syndrome, and diabetes, Dr. Goldfarb introduced a core pathophysiological framework directly connecting rising ambient temperatures to accelerated stone formation based on urine volume reduction (Figure 1).
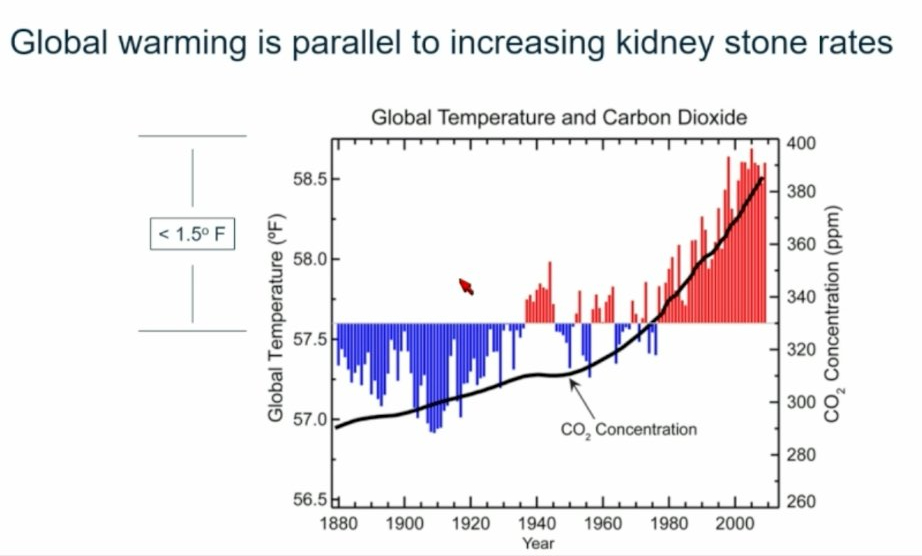
Figure 2. Atmospheric CO2 and temperature rise.1
Reviewing a 120-year climate timeline, he noted that post-World War II climbs in atmospheric carbon dioxide run entirely parallel to a shifting global temperature baseline, showing a graph where the blue bars represent below-average yearly temperatures, while the red bars represent above-average (Figure 2).
Furthermore, he emphasized that between 1963 and 2023, heat waves in the United States altered dramatically, becoming extended in duration (averaging 4 days), more frequent (averaging 6 times per year), and lengthening the overall heat wave season by 46 days, and more intense (1.5°C above the local threshold).
Dr. Goldfarb showcased extensive data from South Carolina tracking stone cases between 1997 and 2015. The findings reveal a tight, undeniable correlation where emergency room visits for kidney stones peak perfectly alongside seasonal shifts in mean monthly ambient temperature. Crucially, the data demonstrated an incredibly tight clinical timeline: stone events manifest approximately 3 days following a severe heat spike, proving that “kidney stones occur concurrent with increases in ambient temperature.”
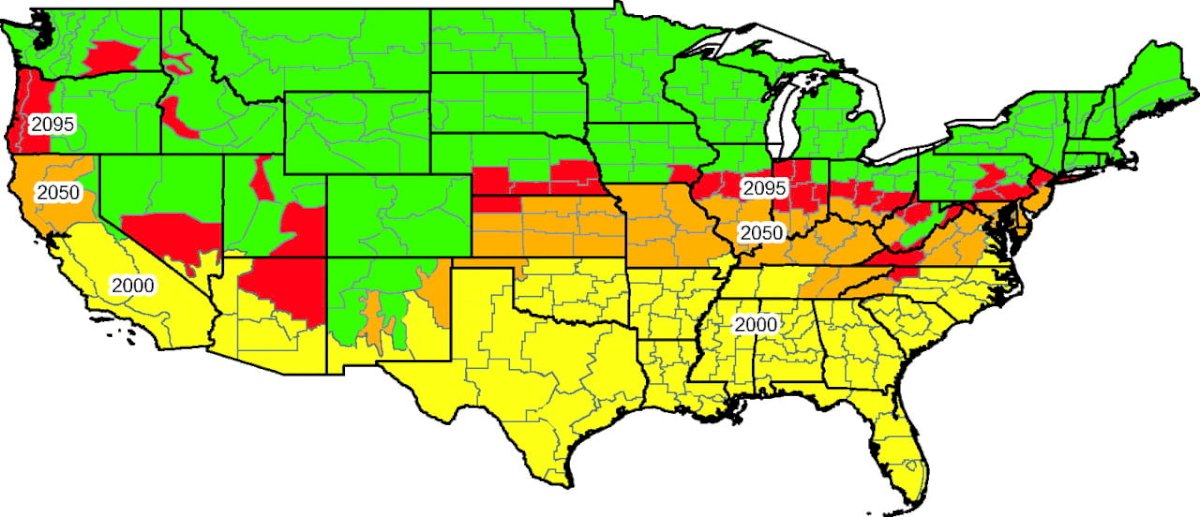
Turning to geographic predictive models, he highlighted the landmark 2008 PNAS study that assessed the expansion of climate-driven urolithiasis. In this study, they demonstrated that each 1°C increase in mean global temperature is associated with an estimated 4.2% increase in individual stone risk, and predicted a geographical northward expansion of the “stone belt” by 2095 (Figure 3).
URBAN HEAT ISLANDS AND THE DISPROPORTIONATE BURDEN OF REDLINING
A major focal point of the lecture was the phenomenon of Urban Heat Islands, where structural city profiles create severe, hyper-local thermal gradients. Due to dense concrete and asphalt absorbing heat radiation, a lack of vegetative shade, and minimal rainwater ground storage, urban centers stay up to 9-12°F hotter than adjacent rural zones (Figure 4). Furthermore, cities act as chronic "non-dippers" at night; unlike rural areas, where temperatures drop safely after sunset, metropolitan areas maintain dangerously high ambient heat around the clock. In places like Phoenix, 49% of summer nights are now categorized as abnormally hot, with average low temperatures jumping nearly 10°F since the 1960s.
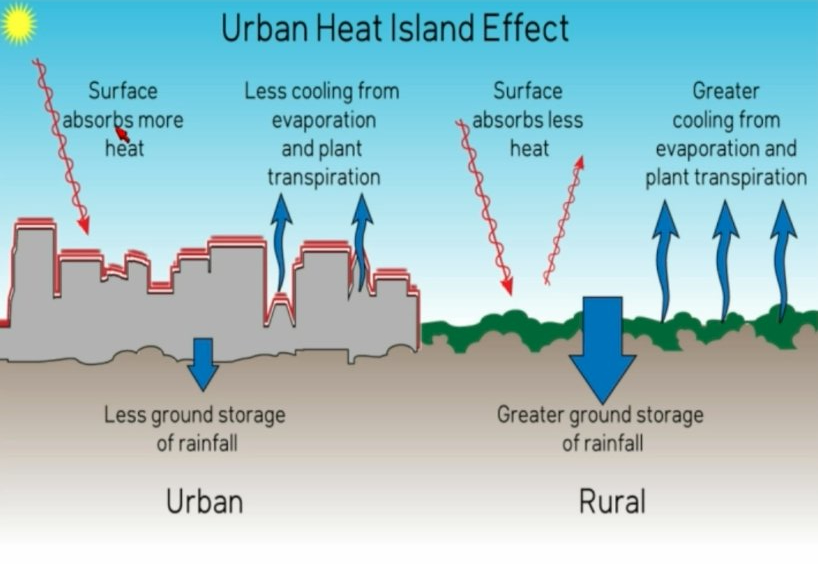
Figure 4. Urban heat island effect.1
Dr. Goldfarb seamlessly bridged this environmental hazard with health equity, presenting NHANES data demonstrating that minoritized populations face a significantly higher rate of increase in stone disease. This disparity is directly tied to the lasting legacy of 1930s "redlining" maps generated by the Home Owners' Loan Corporation (HOLC). Modern climate analyses show that historically redlined, "D-graded" neighborhoods are structurally dense, lack green canopies, and measure 3 to 13°F hotter today than "A-graded" neighborhoods in the exact same city.
BEYOND STONES: ACUTE KIDNEY INJURYThe danger of rising global temperatures extends far beyond lithiasis into parenchymal damage. Dr. Goldfarb highlighted a large-scale case-crossover analysis of extreme heat and AKI. The data indicate a massive risk escalation: on days when ambient temperatures reach 32°C (89.6°F) compared to a baseline of 17°C (62.6°F), the Odds Ratio for developing an AKI episode climbs to 1.6. Additionally, he mapped out the severe cellular strain placed on the kidney in a thermally stressed environment, where dehydration and heat force a cascading pathway of tissue ischemia, localized hypoxemia, ATP depletion, and subsequent accelerated chronic kidney disease progression or mortality.
While there have been strategies to implement preventive programs to improve outcomes during heatwaves, Dr. Goldfarb simply recommends that his patients increase water intake and remain aware of changes in temperature
He concluded this magnificent talk, encouraging the healthcare providers to talk to their patients about global warming and its direct relationship to kidney stones, AKI, and CKD.
Presented by: David S. Goldfarb, MD. Professor of Medicine and Physiology, NYU School of Medicine; Clinical Chief of Nephrology at NYU Langone Medical Center. New York, NY.
Written by: Jonathan Badin-Castro, MD. Endourology and Minimally Invasive Surgery Fellow, Department of Urology, University of California, Irvine. @JonBadin on Twitter during the 2026 American Urological Association (AUA) Annual Meeting, May 15– 18, 2026, Washington D.C. the 2026 American Urological Association (AUA) Annual Meeting, May 15– 18, 2026, Washington D.C.
References:- Goldfarb DS. Climate Change and Kidney Health. State-of-the-Art Lecture presented at: American Urological Association (AUA) Annual Meeting; May 16, 2026; Washington, DC.
- Brikowski TH, Lotan Y, Pearle MS. Climate-related increase in the prevalence of urolithiasis in the United States. Proc Natl Acad Sci U S A. 2008 Jul 15;105(28):9841-6. doi: 10.1073/pnas.0709652105. Epub 2008 Jul 14. PMID: 18626008; PMCID: PMC2474527.