(UroToday.com) Friday’s afternoon plenary session featured Dr. Giovanni E. Cacciamani, who delivered a state-of-the-art lecture on advances in image-guided robotic surgery. Drawing on his group’s extensive portfolio of systematic reviews, meta-analyses, and clinical studies, Dr. Cacciamani traced the field’s transformation. From static preoperative image overlays to dynamic, real-time, AI-powered intraoperative guidance, Dr. Cacciamani laid out a compelling vision for where the technology of image-guided robotic surgery is headed next.
Fluorescence-Guided Surgery: Indocyanine Green (ICG)
Dr. Cacciamani opened the lecture with a discussion on near-infrared fluorescence (NIRF) imaging using indocyanine green (ICG) as a modality of intraoperative image-guided navigation. He explained that ICG is injected intravenously and binds to albumin in the bloodstream. An excitation laser causes the dye to fluoresce, and the signal is captured via a scope-mounted camera connected to a dedicated vision cart, providing real-time green fluorescent overlay on the surgical field.
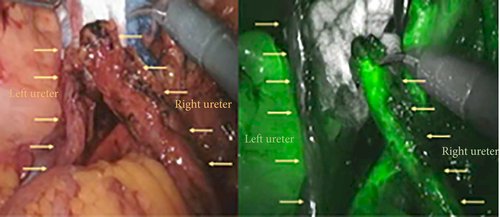
Figure 1: Distal ureters following radical cystectomy as seen under white light (left) and NIRF imaging (right) after i.v. ICG administration, from et al).
Dr. Cacciamani highlighted work from Ahmadi, Aron et al.1 (USC Institute of Urology) demonstrating the use of ICG to minimize uretero-enteric strictures following robotic radical cystectomy. Compared to non-ICG controls (n=132), ICG-guided cases (n=47) demonstrated lower per-patient uretero-enteric stricture rate 10.6% (non-ICG) vs. 0% (ICG), p = 0.020. The per-ureter stricture rate between the non-ICG vs ICG group was 6.6% vs. 0%, p = 0.013, the mean ureter length excised was 2.2 cm vs. 2.7 cm, p = 0.001, and there were no significant differences in operative time, estimated blood loss (EBL), or length of stay (LOS).
Dr. Cacciamani also referenced a phase II randomized comparison of intratumoral versus intraprostatic tracer injection for sentinel lymph node (SLN) detection in prostate cancer.2 Intratumoral injection (n=55) outperformed intraprostatic injection (n=58) on several key metrics: node-positive patients detected (42% vs. 24%, p=0.045), positive SLNs among all positive nodes (73.7% vs. 37.3%, p=0.015), and positive non-SLNs detected (10 vs. 37, p=0.001). Metastasis-free survival was similar between groups.
Augmented Reality in Urological Surgery
After discussing the use of ICG as a static method of image-guided surgery, Dr. Cacciamani then defined augmented reality (AR) as the overlay of computer-generated images onto a live surgical view, enabling real-time tuning of the visual field. He outlined AR’s broad surgical potential. For instance, projecting patient-specific anatomical data directly onto the operative field allows surgeons to better visualize anatomy. AR can also track surgical instruments and improve spatial orientation, which can prove especially useful in complex or high-risk cases.
Dr. Cacciamani credited the Department of Urology at the University of Turin3 as the pioneering group in this field, who began with preoperative 3D reconstructions superimposed onto the operative view. Dr. Cacciamani explained that early iterations relied on high-accuracy 3D models built before surgery. While clinically promising, these models required significant pre-surgical preparation. Image alignment was also manual and could not simulate tissue deformation during the operation, limiting their use to static phases of the procedure.
Dr. Cacciamani highlighted that over recent years, the Turin group has developed elastic, deformable 3D models that move dynamically with the organ in real time during surgery, overcoming the static-model limitation. He presented their data in robot-assisted partial nephrectomy for complex renal tumors (PADUA score ≥ 10), where 3D AR guidance was compared head-to-head with conventional 2D ultrasound guidance. Results demonstrated that 3D AR offered more accurate identification of lesions and intraparenchymal structures, reduced global ischemia rate - 45.8% (3D AR) vs. 69.7% (2D US), increased enucleation rate - 62.5% (3D AR) vs. 37.5% (2D US), and reduced violation of the collecting system - 10.4% (3D AR) vs. 45.5% (2D US).
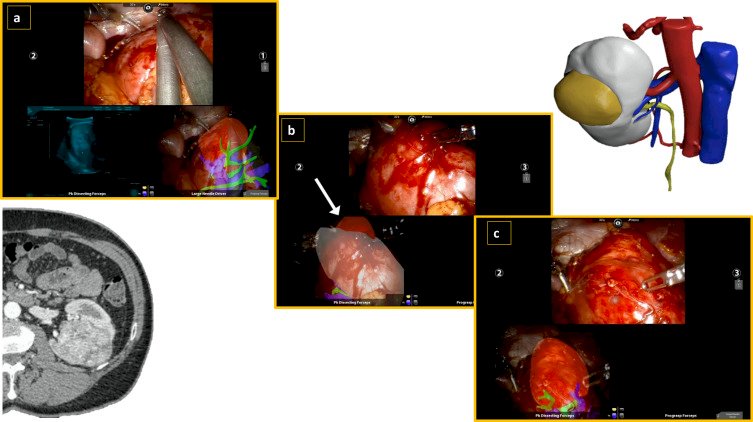
Figure 2: 3D Augmented Reality Robot-assisted Partial Nephrectomy for Complex Tumors.
Dr. Cacciamani then discussed how the same elastic AR framework was applied to robot-assisted radical prostatectomy in the setting of extracapsular extension. He referenced a study by Porpiglia et al.4 demonstrating superiority of the 3D AR group in capsular invasion detection during the nerve-sparing phase: 100% sensitivity vs. 47.0% (p < 0.05). Dr. Cacciamani noted that while the model is dynamic, a key limitation of the current implementation is that image segmentation and overlay are performed manually. Most recently, Dr. Cacciamani described data from his group suggesting AR guidance may improve oncological outcomes in radical prostatectomy, including improved detection of extracapsular extension (EPE) and a reduction in positive surgical margin (PSM) rate from 39% to 20%, with potential functional benefits as well.
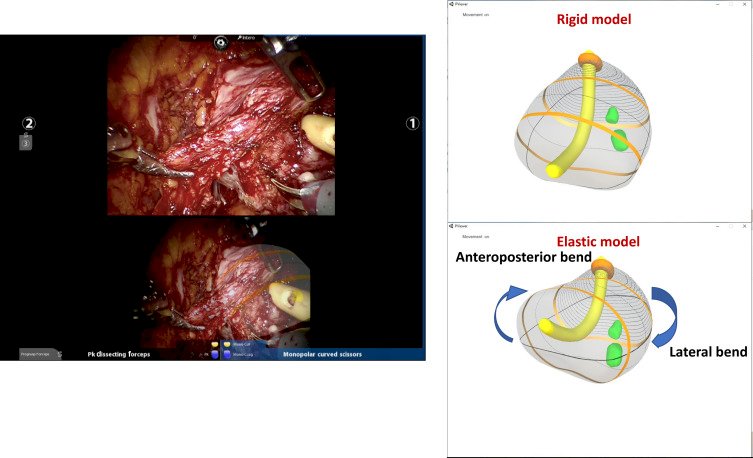
Figure 3: Three-dimensional Elastic AR Robot-assisted Radical Prostatectomy.
Dr. Cacciamani then presented one of the first meta-analyses combining prospective and retrospective data on AR-guided urological surgery conducted by his team. Despite the heterogeneity of included studies, pooled results indicated that AR guidance was associated with reduced global ischemia time, enhanced tumor enucleation, reduced violation of the collecting system, and no negative impact on oncological adequacy.
Surgical Artificial Intelligence
Dr. Cacciamani dedicated the final section of his lecture to the emerging role of surgical AI. He described a comprehensive framework in which pre-operative imaging modalities, including X-ray, ultrasound, CT/PET, nuclear medicine, MRI, etc, and intraoperative inputs, including NIRF, fluoroscopy, optical coherence tomography, optical, etc. feed into AI algorithms. These supervised and unsupervised algorithms enable capabilities such as 3D shape reconstruction, depth estimation, structural mapping, soft tissue feature tracking, and AR-based image registration in real-time.
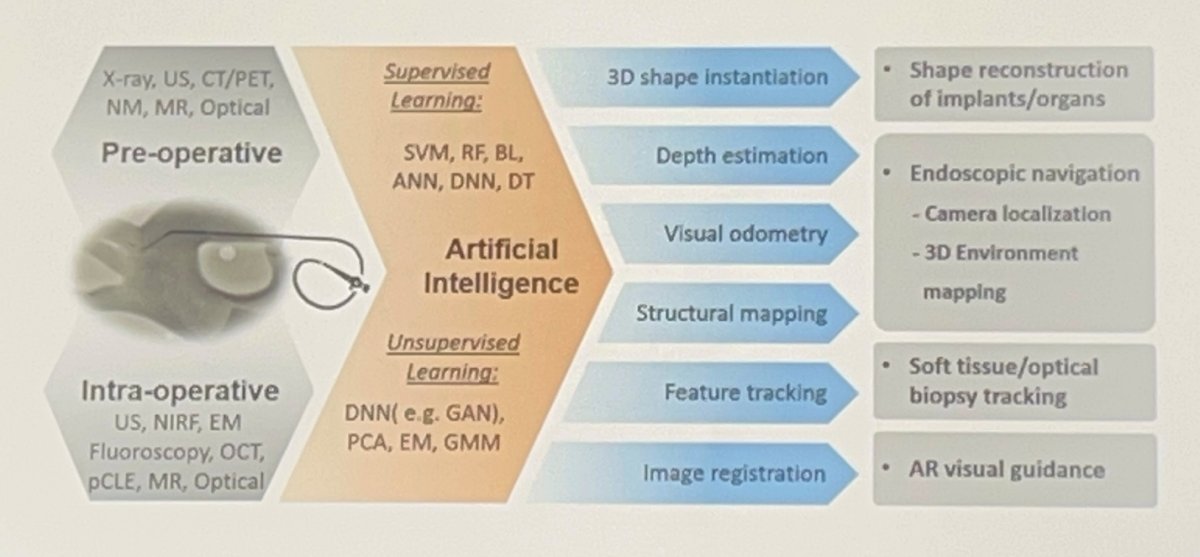
Figure 7: Workflow of Applications of Artificial Intelligence in Surgery.
Dr. Cacciamani explained that training pipelines involve expert surgeons annotating surgical video to define safe and unsafe operative zones, providing the foundational data that drives algorithmic learning.
Dr. Cacciamani showcased a practical demonstration from Endolux, which has developed an AI-trained system capable of automated, real-time identification of the bladder and bladder neck during endoscopic procedures. This is a key advantage over prior AR frameworks that depended on pre-operative segmentation and registration.
Figure 8: AI-Trained Automated Bladder and Bladder Neck Detection.
Dr. Cacciamani described another key of applying AI - automated surgical instrument detection and motion analysis. By tracking instruments in real time, AI systems can quantify instrument motion, predict potential surgical errors before they occur, and prompt movement adjustments. As Dr. Cacciamani emphasized, “We have to start thinking about AI as something implemented in real time in our surgical performance,” he stressed, “not something we do later on for analyzing the data.”
Dr. Cacciamani also presented a systematic review and meta-analysis from his group on automated AI-based detection of intraoperative adverse events.5 The pooled analysis demonstrated that machine learning, specifically deep learning architectures, outperformed expert human reviewers in detecting intraoperative complications from surgical video, with an odds ratio of 14.74 (95% CI: 4.70–46.18). Dr. Cacciamani added that his team is currently developing texture-based AI tools for real-time bleeding source detection in laparoscopic surgery.
Intraoperative Navigation: From Static to Dynamic
Referencing foundational work by Rassweiler et al.,6 Dr. Cacciamani noted that intraoperative navigation has proven useful in percutaneous renal access, renal tumor biopsy, radical prostatectomy, and partial nephrectomy using various tracking techniques. He highlighted that early studies validated marker-based navigation laparoscopy, and that investigators were able to demonstrate the differential impact of real-time versus quasi-real-time rigid navigation systems. Dr. Cacciamani proposed that combining multiple tracking modalities offers a clear pathway to further improvements in minimally invasive surgery.
Dr. Cacciamani revisited a conceptual benchmark from his opening: in 2016, image-guided surgery was essentially static. The superimposition of preoperative landmarks was done manually and suffered from temporal lag. Today, he emphasized, guidance systems are digital, dynamic, and increasingly AI-augmented. The field has moved firmly toward the digitalization of the operative environment through integrated image-guided navigation.
Take-Home Messages
Concluding his talk, Dr. Cacciamani left the audience with the following key messages. First, image-guided surgical navigation technology is here to stay. The field has evolved and continues to evolve rapidly. Secondly, intraoperative navigation has transitioned from static to dynamic. Third, image-guided and radio-guided navigation are advancing in parallel. AI changes the entire landscape of camera-based surgery through real-time automation. Lastly, new trials are needed to evaluate these technologies on intraoperative performance, safety, and long-term oncological adequacy.
Presented by: Giovanni E. Cacciamani, MD, MSc, FEBU, Associate Professor of Research Urology and Radiology, University of Southern California, Los Angeles, CA, USA
Written by: Helen Gao, Medical Student at Robert Wood Johnson Medical School, Leadership and Innovation Fellowship Training (LIFT) Scholar at Department of Urology, University of California, Irvine. @helengao295 on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
- Ahmadi N, Ashrafi AN, Hartman N, et al. Use of indocyanine green to minimise uretero-enteric strictures after robotic radical cystectomy. BJU Int. 2019;124(2):302-307. doi:10.1111/bju.14733
- Wit EMK, van Beurden F, Kleinjan GH, et al. The impact of drainage pathways on the detection of nodal metastases in prostate cancer: a phase II randomized comparison of intratumoral vs intraprostatic tracer injection for sentinel node detection. Eur J Nucl Med Mol Imaging. 2022;49(5):1743-1753. doi:10.1007/s00259-021-05580-0
- Porpiglia F, Checcucci E, Amparore D, et al. Three-dimensional Elastic Augmented-reality Robot-assisted Radical Prostatectomy Using Hyperaccuracy Three-dimensional Reconstruction Technology: A Step Further in the Identification of Capsular Involvement. Eur Urol. 2019;76(4):505-514. doi:10.1016/j.eururo.2019.03.037
- Porpiglia F, Checcucci E, Amparore D, et al. Three-dimensional Augmented Reality Robot-assisted Partial Nephrectomy in Case of Complex Tumours (PADUA ≥10): A New Intraoperative Tool Overcoming the Ultrasound Guidance. Eur Urol. 2020;78(2):229-238. doi:10.1016/j.eururo.2019.11.024
- Eppler MB, Sayegh AS, Maas M, et al. Automated Capture of Intraoperative Adverse Events Using Artificial Intelligence: A Systematic Review and Meta-Analysis. J Clin Med. 2023;12(4):1687. Published 2023 Feb 20. doi:10.3390/jcm12041687
- Rassweiler J, Rassweiler MC, Müller M, et al. Surgical navigation in urology: European perspective. Curr Opin Urol. 2014;24(1):81-97. doi:10.1097/MOU.0000000000000014