(UroToday.com) Advances in imaging software have made three-dimensional (3D) volumetric analysis more common in the surgical planning of patients with urolithiasis. Even though stone size is usually described using traditional linear measurements like maximal stone diameter, these measurements do not always reflect the true overall stone burden, especially in patients with multiple stones or more complex stone shapes such as staghorn calculi. Since most clinicians are still more familiar with standard linear measurements, there is a growing need for a practical reference tool that connects commonly used stone size cutoffs with estimated 3D stone volumes.
In this study, researchers from the University of Rochester retrospectively reviewed preoperative CT scans from patients who underwent surgery for urolithiasis between June 2010 and December 2024. Using Spectra IDS7 software, they measured the maximal stone length in any imaging plane and calculated corresponding 3D stone volumes. These measurements were added together to determine each patient’s total cumulative stone length and volume. They also recorded the number of stones present and whether staghorn calculi were identified. To better understand how traditional stone measurements relate to overall stone burden, volume distributions were analyzed across clinically relevant stone length cutoffs of 5 mm, 10 mm, 15 mm, and 20 mm. Regression models were then used to determine how total stone length, stone number, and staghorn morphology affected overall stone volume.
A total of 653 stone procedures were included in the analysis. The results showed that stone volume increased in a nonlinear manner as cumulative stone length increased. Smaller stones tended to have a much narrower range of volumes, while larger stones showed significantly more variability. For example, stones in the 5 mm category had fairly consistent volumes, whereas stones in the 15 mm and 20 mm groups varied much more widely. This suggests that as stones become larger and more complex, linear measurements alone become less reliable in estimating the true stone burden.
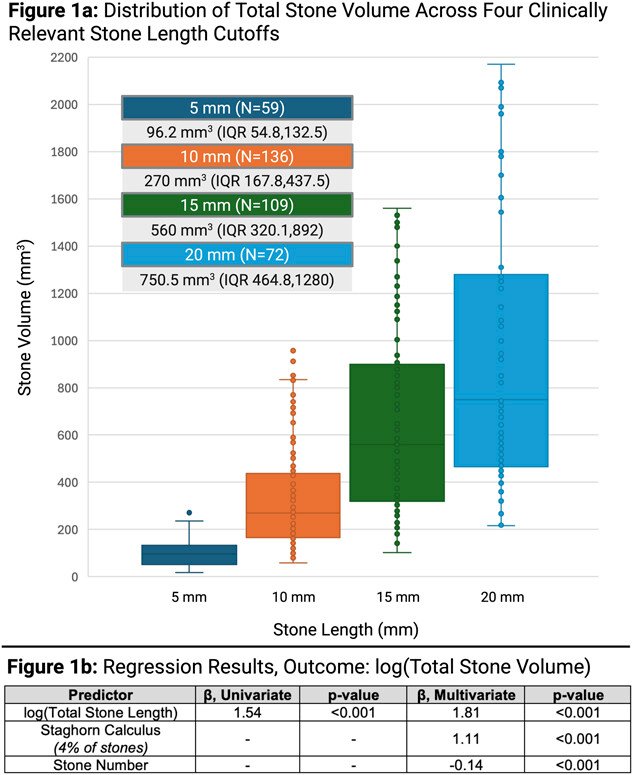
Figure 1a. Distribution of total stone volume across clinically relevant stone length cutoffs.
The regression analysis also found that total stone length was strongly associated with total stone volume, although the relationship was affected by both stone number and staghorn morphology. Patients with staghorn calculi generally had much larger stone volumes compared to patients with non-staghorn stones of similar cumulative length. On the other hand, patients with multiple smaller stones often had lower overall stone volumes despite having similar cumulative stone lengths. These findings show that two patients with the same linear stone measurements may still have very different overall stone burdens depending on the shape and distribution of the stones.
Figure 1b. Regression analysis predicting log(total stone volume) based on cumulative stone length, staghorn morphology, and stone number.
During the Q&A, an audience member asked how the linear stone measurements were determined and where the start and end points were chosen. Mr. Winzer clarified that the measurement was taken using the longest visible dimension of the stone across any of the three imaging planes. Dr. Jain, who also worked on this study, also noted that although prior studies have shown that clinical outcomes correlate more closely with stone volume than stone length, clinicians still commonly think in terms of “5 mm” or “10 mm” stones. Because of this, the study aimed to help contextualize what those familiar stone sizes actually look like in terms of total volume.
Overall, this study highlights some of the limitations of relying only on traditional linear stone measurements when estimating stone burden and planning surgical treatment. The authors suggest that incorporating volumetric reference tools into clinical practice could improve preoperative evaluation and provide a more accurate understanding of stone complexity. By better understanding how cumulative stone length relates to actual 3D stone volume, clinicians may be able to make more informed decisions and improve surgical planning for patients with urolithiasis.
Presented by: Benedikt Winzer, Medical Student, University of Rochester School of Medicine and Dentistry, NY, USA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between May 15 – May 18, 2026, in Washington, D.C
Reference:
- Benedikt M. Winzer, Carl Ceraolo, Jason Fairbourn, Ashley Li, Yadong Lu, Scott Quarrier, Rajat K. Jain. From Length to True Burden: Making Sense of Linear Stone Measurements [abstract]. In: American Urological Association Annual Meeting, May 15-18, 2026, Washington, DC.