(UroToday.com) At the 2026 American Urological Association (AUA) Annual Meeting, Dr. Kendrick Yim from the Moffitt Cancer Center presented results from a randomized, double-blind, placebo-controlled trial evaluating the role of alvimopan, a peripheral μ-opioid receptor antagonist, in patients undergoing radical cystectomy with urinary diversion within a standardized Enhanced Recovery After Surgery (ERAS) protocol.
Alvimopan has previously shown efficacy in reducing postoperative ileus and accelerating bowel recovery after major abdominal surgery; however, much of the initial work surrounding its benefit was prior to the widespread implementation of comprehensive ERAS pathways, begging the question as to whether the drug still offers postoperative benefit in light of modern recovery protocols where many perioperative measures have already been implemented to improve gastrointestinal recovery.
Between October 2018 and December 2024, 132 patients between 18 and 85 years of age undergoing radical cystectomy with urinary diversion within a standardized ERAS protocol were randomized to receive either 12 mg alvimopan (n=67) or placebo (n=65) preoperatively, followed by twice-daily dosing for up to seven days postoperatively. The study’s primary endpoint was the time to recovery of combined upper and lower GI function, defined by tolerance of diet (G1) and bowel movement (G2). Secondary endpoints were hospital length of stay, nasogastric tube insertion, prolonged hospitalization, and 30-day postoperative readmission rates.
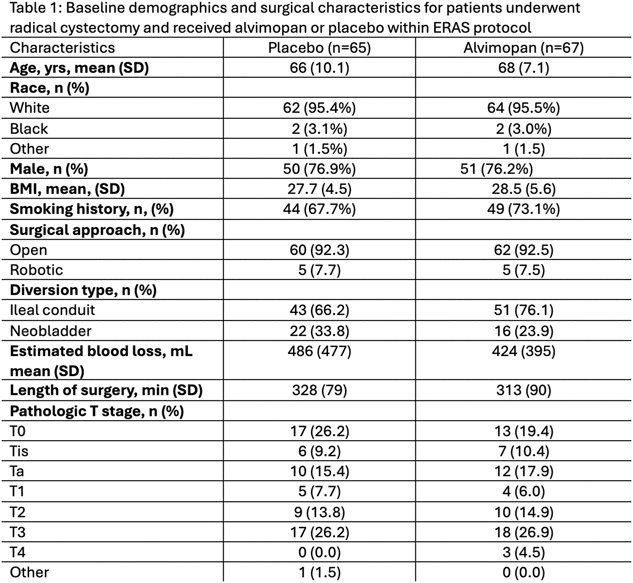
Table 1: Baseline characteristics and demographics
Overall, there were no meaningful differences observed in GI recovery between the two groups: the mean time to recovery of bowel function was 4.2 days in the alvimopan cohort compared to 4.1 days in the placebo cohort. Neither were there any significant differences in secondary outcomes between the groups: the rate of nasogastric tube insertion was 13.8% vs. 11.9% between the alvimopan cohort and placebo cohorts, respectively. Similarly, median hospital length of stay, incidence of prolonged hospitalization, and 30-day readmission rates were identical between groups.
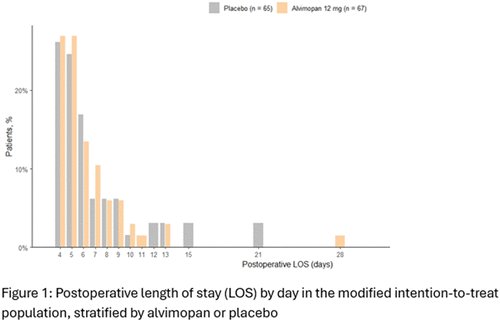
Figure 1: Postoperative length of stay for control and treatment groups
Dr. Yim concluded that within the context of a standardized ERAS pathway, alvimopan did not confer any GI benefits following radical cystectomy and urinary diversion, indicating that many of the previously identified benefits of alvimopan may already be being captured by modern ERAS protocols that have incorporated multimodal perioperative recovery strategies.
The study highlighted the broader trend toward reassessing legacy perioperative interventions as ERAS protocols continue to become increasingly optimized, specifically generating discussion and calling into question whether the routine use of alvimopan remains cost-effective in systems with such protocols.
Presented by: Kendrick Yim, MD, Moffitt Cancer Center, Tampa, FLWritten by: Tom No, Junior Specialist, Department of Urology, University of California Irvine, during the 2026 American Urological Association (AUA) Annual Meeting, May 15– 18, 2026, Washington, D.C.