(UroToday.com) The 2026 AUA annual meeting featured a non-invasive bladder cancer session and a presentation by Dr. Gal Wald discussing the final results of a phase II trial of BCG and intravesical gemcitabine for patients with BCG-exposed high-grade non-muscle invasive bladder cancer.
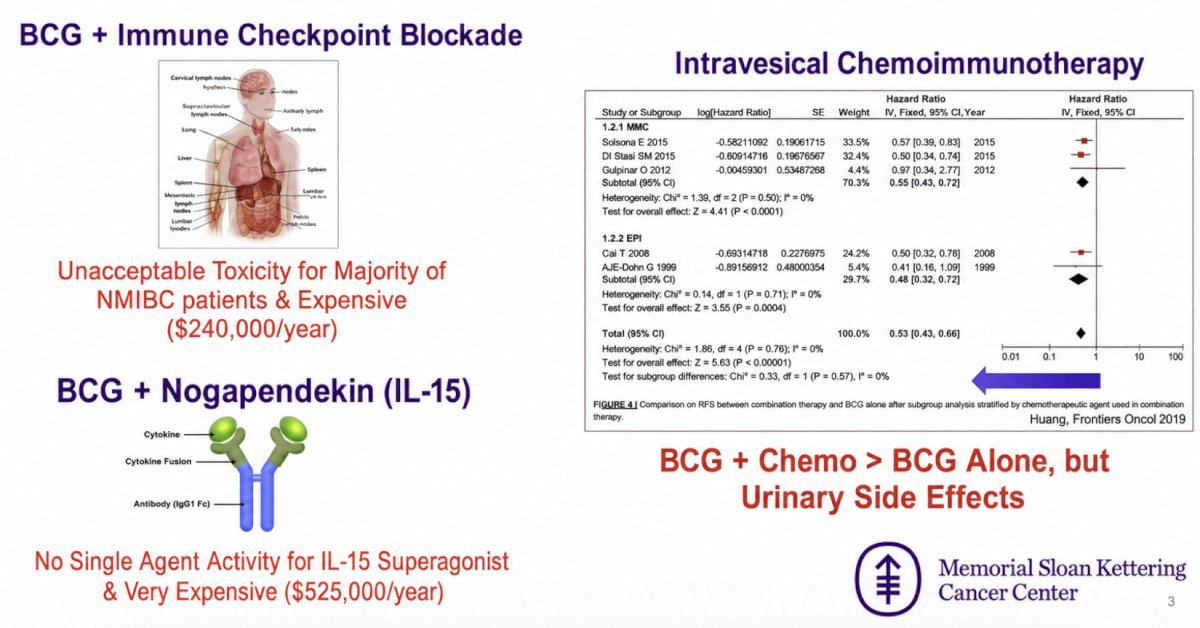
Retreatment with BCG remains the standard of care for BCG-exposed high-grade non-muscle invasive bladder cancer. However, response rates to BCG retreatment and with gemcitabine and docetaxel are only ~50%. Combination therapies are needed, with the current treatment landscape (and its limitations) highlighted in the following figure:
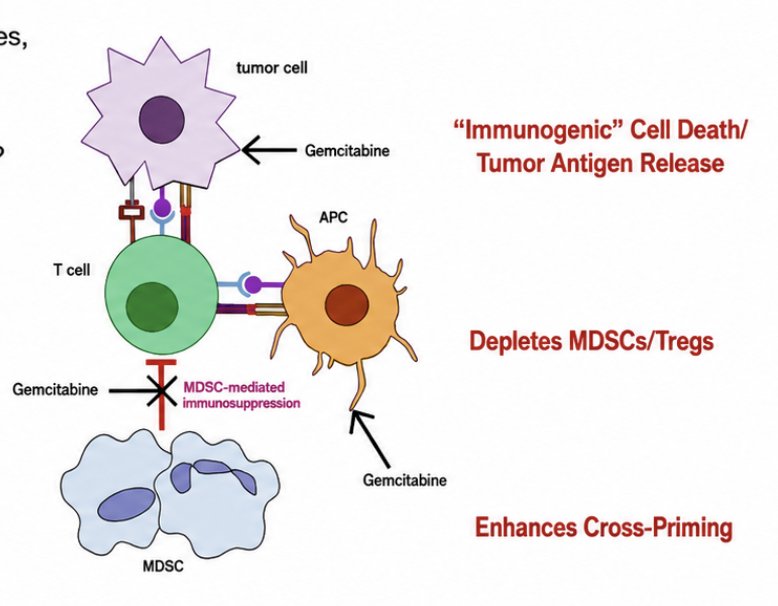
Intravesical gemcitabine, compared to mitomycin, is more effective and better tolerated. Gemcitabine has direct toxicity on the bladder by inhibiting (i) DNA replication, (ii) the formation of deoxyribonucleotides, and (iii) the nucleotide excision repair pathway. Additionally, gemcitabine has multiple immune-enhancing effects, including blocking the recruitment of MDSCs, enhancing the anti-tumor activity of CD8+ T cells and activated NK, it may enhance yoT cell (critical in the BCG response), and it increases the expression of HLA-I, Fas/FasL, and INF-gamma:
Combination intravesical gemcitabine + BCG is a novel chemoimmunotherapy regimen that may enhance immune activity and direct cytotoxicity. At AUA 2026, Dr. Wald and colleagues presented the final results from their phase II single-arm multi-institutional trial with gemcitabine + BCG in BCG-exposed high-grade non-muscle invasive bladder cancer.
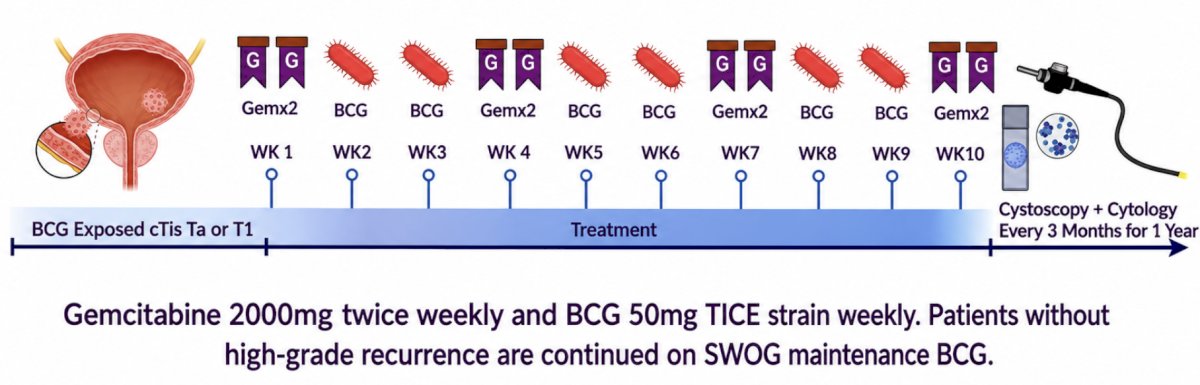
Patients with BCG-exposed non-muscle invasive bladder cancer (HG Ta/HG T1/Tis) within 24 months of the last treatment with BCG were eligible. Exclusion criteria included contraindication to BCG, BCG-unresponsive non-muscle invasive bladder cancer, and concurrent prostatic urethral or upper tract urothelial cancer. Patients underwent TURBT followed by intravesical instillation of 2,000 mg gemcitabine twice weekly (weeks 1, 4, 7, 10), and once weekly 50 mg TICE BCG (weeks 2, 3, 5, 6, 8, 9) followed by 1-year of maintenance BCG in responders:
Centralized pathologic review was performed. The primary endpoint was complete response at 6 months, defined as the proportion of patients who are free of high-grade disease within the bladder. The trial followed an optimal Simon two-stage design (complete response 55% versus 75%, 5% type 1 error, and 80% power), requiring at least 29 responses out of a total 43 patients.
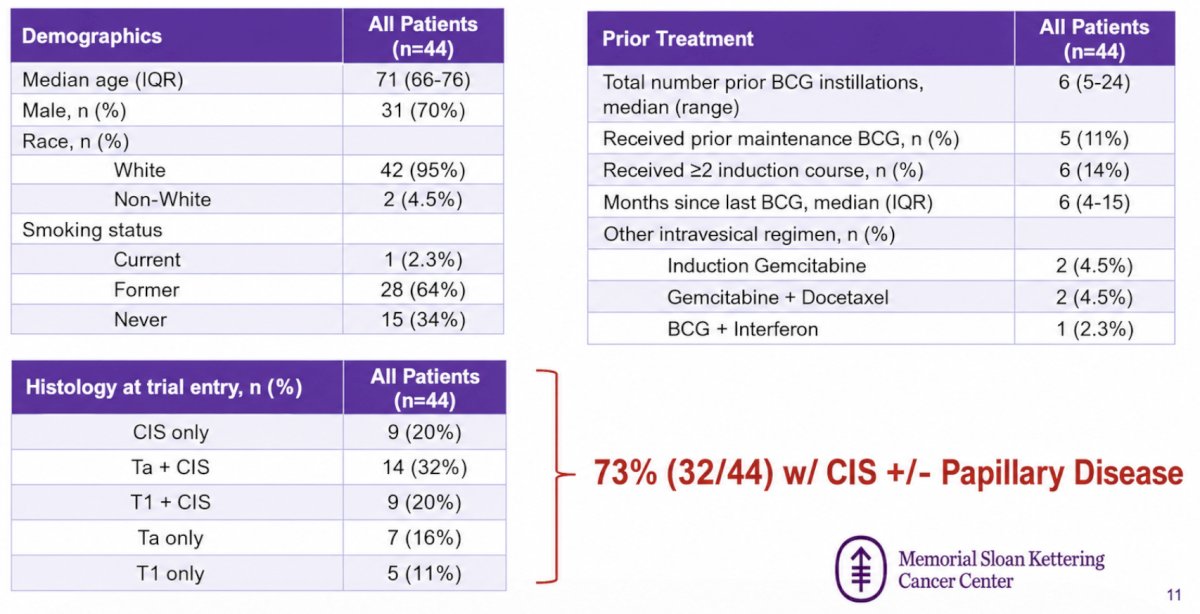
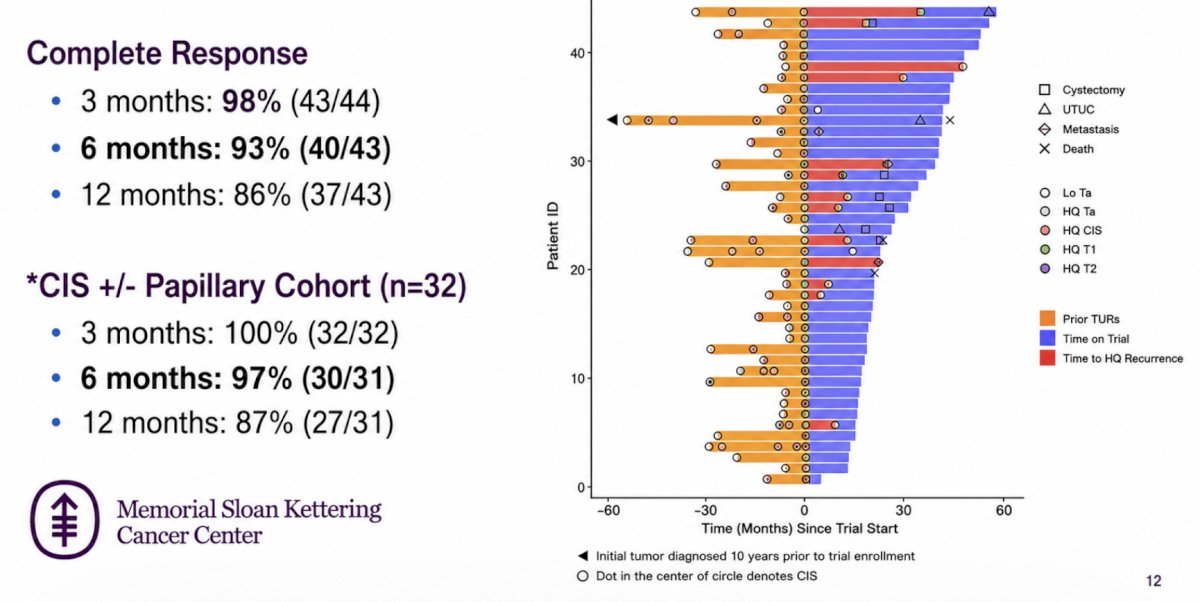
A total of 44 patients were enrolled in the phase II trial. Most patients received one prior BCG induction course, but 14% (6/44) of patients received ≥2 prior courses, and 11% (5/44) had prior maintenance. Four (9%) had prior induction gemcitabine (± docetaxel). Upon trial entry, 73% (32/44) had CIS ± Ta/T1 while 27% (12/44) had papillary-only disease:
The 6-month complete response was 93% (40/43) for the overall cohort and 97% (30/31) in those with CIS:
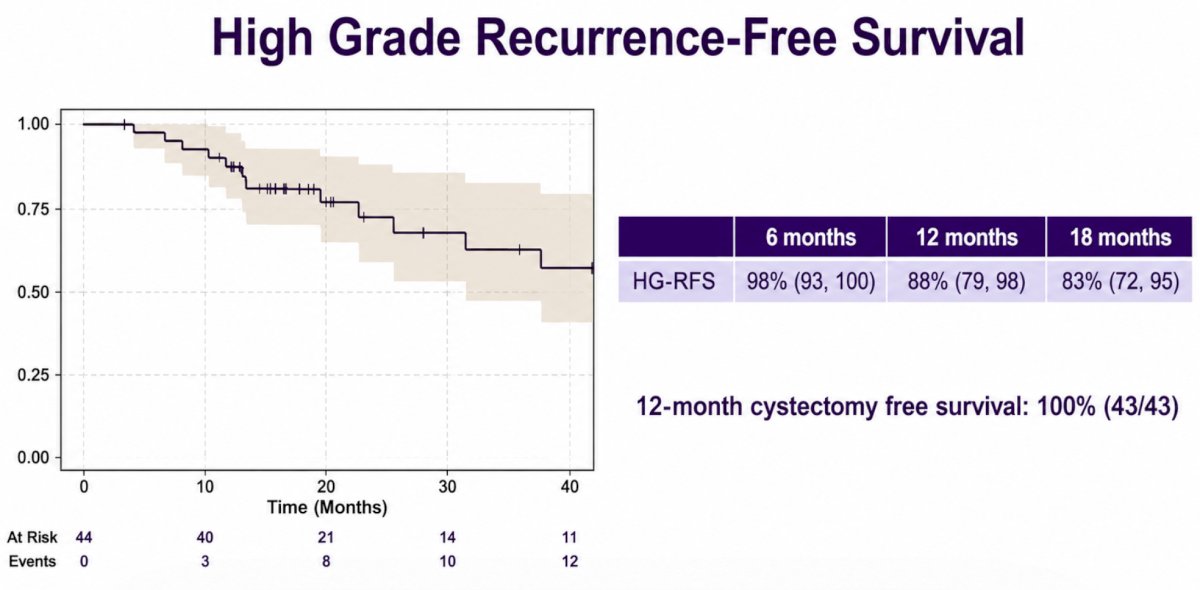
The 18-month high-grade recurrence-free survival was 83% (95% CI 72-95), and the 18-month cystectomy-free survival was 100% (95% CI 100-100):
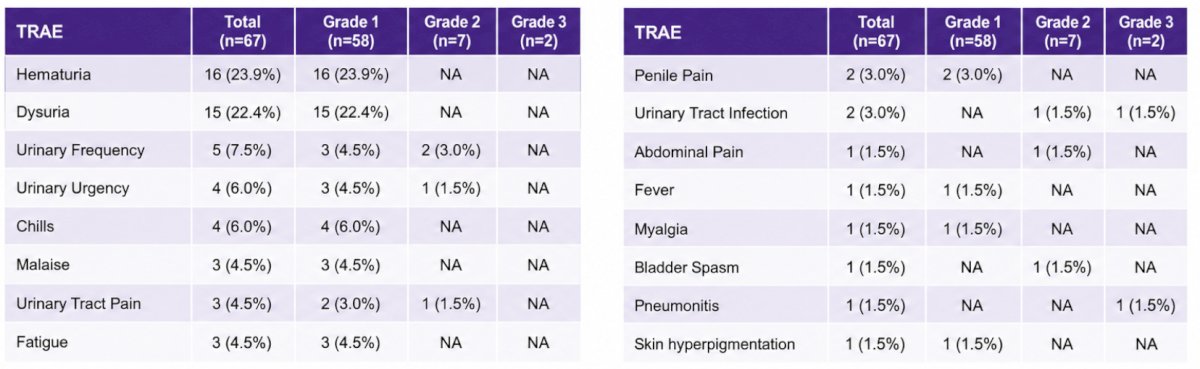
Grade 1-2 treatment-related adverse events were common and similar to what is expected with monotherapy. Two (5%) grade 3 treatment-related adverse events occurred (pneumonitis, which resolved, and a urinary tract infection requiring 1 dose of IV antibiotics). No patient experienced grade 4-5 toxicity:
Dr. Wald concluded his presentation discussing the final results of a phase II trial of BCG and intravesical gemcitabine for patients with BCG-exposed high-grade non-muscle invasive bladder cancer with the following take-home points:
- Gemcitabine + BCG in BCG-exposed high-grade non-muscle invasive bladder cancer demonstrates excellent oncological efficacy with minimal treatment-related adverse events
- Correlative studies are ongoing
- Based on these results, the randomized phase III GAIN trial (ALLIANCE A032303/NCT07000084) is comparing gemcitabine + BCG versus BCG for patients with BCG-exposed high-grade non-muscle invasive bladder cancer and is open for enrollment
Presented by: Gal Wald, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.