(UroToday.com) At the 2026 American Urological Association (AUA) Annual Meeting in Washington, DC, a point-counterpoint session addressed one of the most important emerging questions in muscle-invasive bladder cancer (MIBC): what is the optimal local management strategy for patients who achieve a clinical complete response (cCR) following neoadjuvant enfortumab vedotin plus pembrolizumab (EV+pembro)?
With perioperative EV+pembro now demonstrating excellent pathologic complete response (pCR), event-free survival (EFS), and overall survival (OS) benefits in the phase III KEYNOTE-905/EV-303 and KEYNOTE-B15/EV-304 trials,1,2 the historical assumption that all patients require immediate radical cystectomy is increasingly being challenged. In this session, Dr. Leslie Ballas argued in favor of bladder-preserving radiation, Dr. Kelly Bree contended that radical cystectomy remains essential, and Dr. Kent Mouw proposed that active surveillance is the best option for most patients with cCR after EV+pembro.
Dr. Leslie Ballas began by making the case that radiation therapy is an underutilized but highly effective bladder-preserving strategy. She emphasized that if modern systemic therapy has already eradicated the majority of invasive disease, local therapy should focus on achieving durable bladder control while minimizing treatment-related morbidity and preserving quality of life. To illustrate the limitations of relying on clinical restaging alone, she revisited the SWOG 0219 trial, which enrolled patients with cT2–T4aN0M0 MIBC treated with neoadjuvant paclitaxel, carboplatin, and gemcitabine (PCG).3 Following repeat transurethral resection of bladder tumor (TURBT), 34 of 74 patients (46%) were classified as cT0. Ten of these patients subsequently underwent immediate radical cystectomy, and only 4 (40%) were found to have pT0 disease. The remaining 6 patients (60%) harbored persistent residual disease, including carcinoma in situ, lamina propria invasion, muscle-invasive disease, and one patient with lymph node metastasis. These findings underscore that even an apparently complete clinical response does not guarantee pathologic eradication of disease.

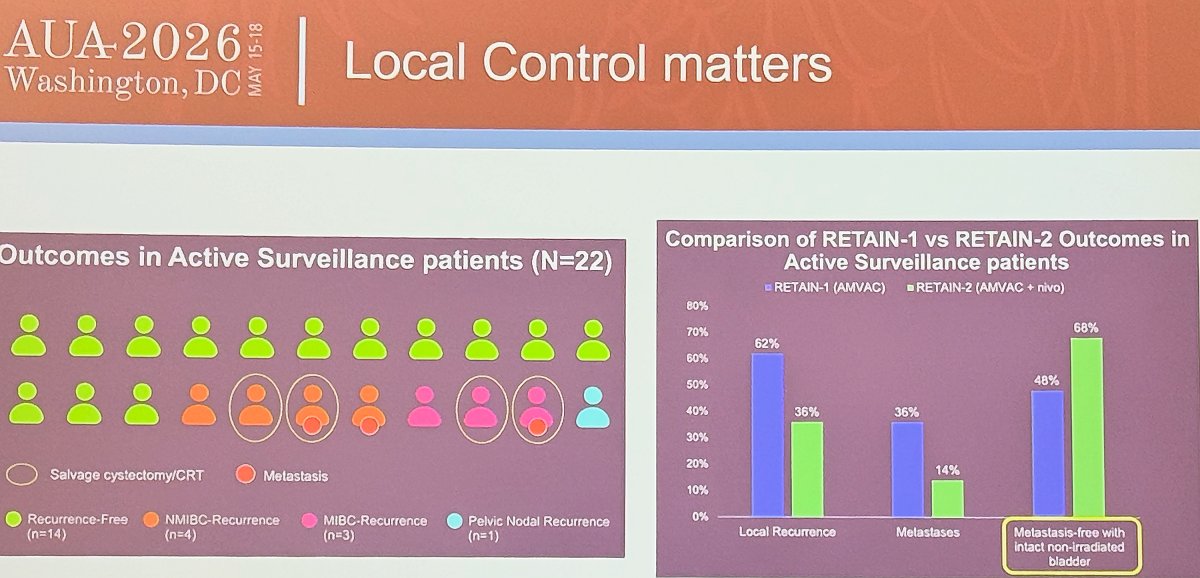
Dr. Ballas then highlighted more contemporary response-adapted surveillance studies. In RETAIN-2, patients with favorable biomarkers and cCR after neoadjuvant accelerated MVAC plus nivolumab were eligible for active surveillance. Among 22 surveillance patients, 14 (64%) remained recurrence-free, while 4 developed non-muscle-invasive recurrences, 3 developed muscle-invasive recurrences, and 1 experienced an isolated pelvic nodal recurrence. Compared with RETAIN-1, outcomes improved substantially with the addition of nivolumab: local recurrence decreased from 62% to 36%, metastatic recurrence decreased from 36% to 14%, and metastasis-free survival with an intact non-irradiated bladder improved from 48% to 68%. Dr. Ballas argued that these data suggest increasingly effective systemic therapy is expanding the feasibility of bladder preservation strategies.4,5
Quality of life was another central component of Dr. Ballas’ argument. She reviewed contemporary patient-reported outcomes comparing bladder preservation and radical cystectomy, noting similar bowel and urinary function scores but superior sexual function, body image, cognitive function, informed decision-making, and less interference with daily activities among patients managed without cystectomy. Although radical cystectomy was associated with less pain and better emotional functioning in some analyses, Dr. Ballas emphasized that for many patients, preserving the native bladder represents a meaningful quality-of-life advantage.

She concluded by highlighting two ongoing cooperative group studies that will further inform this question: ARCHER (Alliance A032103), which is evaluating neoadjuvant EV+pembro followed by response-adapted bladder preservation, and BRIGHT (SWOG/NRG S2406), which is investigating modern radiation-based bladder preservation approaches.

Dr. Kelly Bree then presented an opposing viewpoint, arguing that radical cystectomy remains the cornerstone of curative therapy after EV+pembro. She began by emphasizing that radical cystectomy forms the backbone of all current level 1 evidence supporting perioperative EV+pembro. In both KEYNOTE-905/EV-303 and KEYNOTE-B15/EV-304, all patients were intended to undergo radical cystectomy, and the demonstrated survival benefits therefore reflect the combination of highly active systemic therapy plus definitive surgical extirpation.

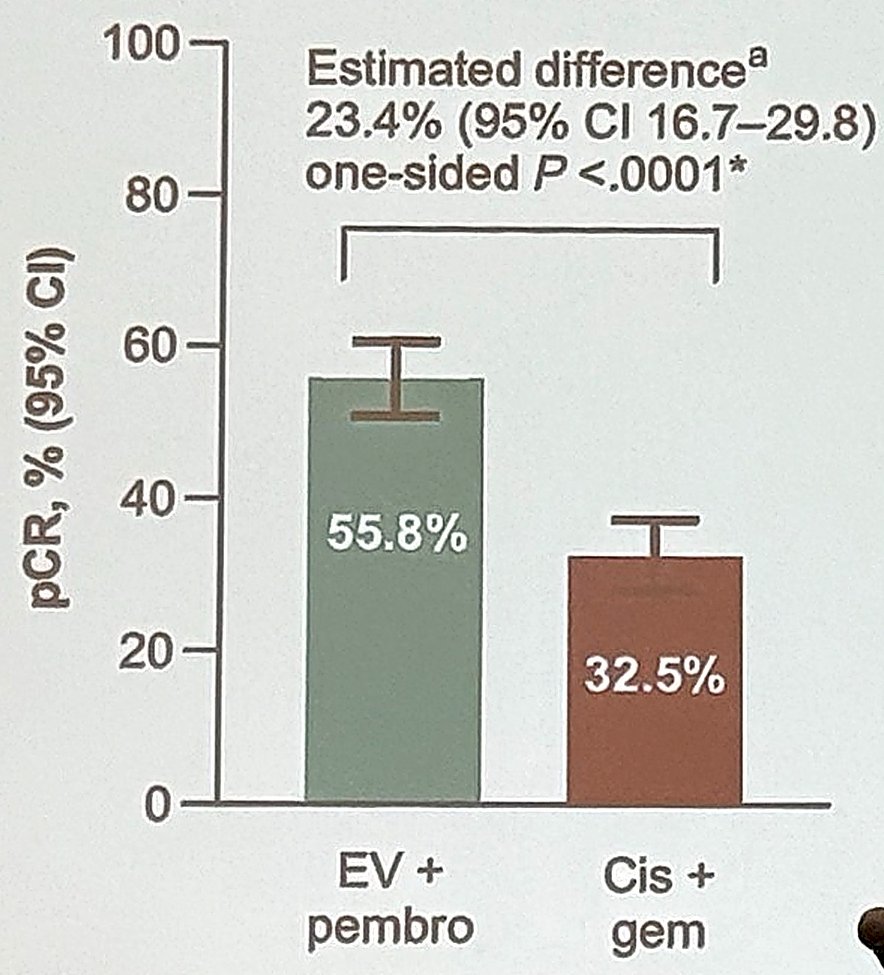
Dr. Bree reviewed the pivotal efficacy data from these studies. In KEYNOTE-905/EV-303, which enrolled cisplatin-ineligible or cisplatin-declining patients with cT2–T4aN0M0 or T1–T4aN1M0 urothelial carcinoma, perioperative EV+pembro reduced the risk of EFS events by 60% compared with surgery alone (HR 0.40, 95% CI 0.28–0.57; one-sided p<0.0001) and reduced the risk of death by 50% (HR 0.50, 95% CI 0.33–0.74; one-sided p=0.0002). The pathologic complete response rate was approximately 57%, with pathologic downstaging to <ypT2N0 achieved in nearly two-thirds of patients. In KEYNOTE-B15/EV-304, which compared perioperative EV+pembro with neoadjuvant gemcitabine/cisplatin in cisplatin-eligible patients, the pCR rate was 55.8% with EV+pembro versus 32.5% with gemcitabine/cisplatin, representing an absolute improvement of 23.4% (95% CI 16.7–29.8; one-sided p<0.0001). Pathologic downstaging rates were 63.7% versus 45.2%, respectively. Interim survival analyses also favored EV+pembro, with EFS HR 0.53 and OS HR 0.65.
Despite these remarkable results, Dr. Bree stressed that there are no randomized data demonstrating that EV+pembro alone produces outcomes equivalent to EV+pembro followed by radical cystectomy. She emphasized a critical concept: clinical complete response is not synonymous with pathologic complete response. Clinical staging remains notoriously inaccurate, and residual disease may persist despite apparently normal cystoscopy, cytology, and imaging findings. To support this point, she cited a 2026 systematic review and meta-analysis by Roessler and colleagues evaluating concordance between cCR and pCR.6 Across 10 studies and 419 patients, the pooled proportion of true pCR among patients categorized as having cCR was only 51% (95% CI 42–60), meaning that more than half of patients thought to have eradicated disease still harbored residual tumor at cystectomy.

Dr. Bree also discussed circulating tumor DNA (ctDNA) as a potential biomarker for response assessment. Data from the RETAIN studies demonstrated that post-neoadjuvant ctDNA positivity strongly predicted residual disease; however, ctDNA negativity did not reliably identify patients with ypT0. In one analysis, 67% of ctDNA-negative patients still had ≥pT2 disease at radical cystectomy, underscoring that currently available biomarkers remain inadequate for confidently selecting patients who can safely forgo surgery.

Finally, Dr. Bree argued that delaying or omitting radical cystectomy risks missing a critical opportunity for cure. She highlighted outcomes from RETAIN-1 and RETAIN-2 showing local recurrence rates of 62% and 36%, respectively, and metastatic recurrence rates of 36% and 14%. Even with improved systemic therapy, approximately three in five surveillance patients experienced local recurrence and roughly one in three developed metastases in earlier cohorts. Her conclusion was straightforward: until more accurate tools are available to distinguish true complete responders from patients with occult residual disease, radical cystectomy should remain the standard consolidative treatment following EV+pembro.

Dr. Kent Mouw concluded the session by arguing that surveillance is the most appropriate option for most patients with cCR after EV+pembro. He began by reframing the implications of the KEYNOTE-905/EV-303 and KEYNOTE-B15/EV-304 results. Since the majority of patients in both trials achieved pCR at radical cystectomy—57% in EV-303 and 56% in EV-304—he argued that most patients may not have required radical cystectomy in the first place. Consequently, a large proportion may have been unnecessarily exposed to the morbidity, quality-of-life consequences, and long-term functional impairments associated with local therapy.
Dr. Mouw emphasized that the central question is not whether cCR predicts pCR, but whether cCR predicts metastasis-free survival (MFS). If patients can be monitored closely and local recurrences detected before systemic dissemination occurs, salvage local therapy may be administered without compromising cure. He cited the prospective, phase II HCRN GU16-257 trial, in which patients with MIBC received gemcitabine/cisplatin plus nivolumab followed by response-adapted management. Among patients achieving cCR and managed with surveillance plus maintenance nivolumab, the positive predictive value of cCR for 2-year MFS was 97%. Test characteristics were highly favorable, with sensitivity 0.89, specificity 0.97, positive predictive value 0.97, and negative predictive value 0.89.7
A critical observation supporting surveillance was that local recurrences consistently preceded metastatic recurrences. In RETAIN-2, no patient developed metastatic disease in the absence of a prior local recurrence. Similarly, in RETAIN-1, local recurrence preceded metastatic progression in 8 of 9 patients. These findings suggest that structured surveillance can identify failures early enough to permit effective salvage radical cystectomy or radiation therapy without jeopardizing metastasis-free outcomes.

Dr. Mouw also discussed emerging biomarkers that may further improve patient selection. In the RETAIN analyses, ctDNA positivity after neoadjuvant therapy identified patients at very high risk of residual disease and recurrence, while data presented by Epstein and colleagues at ASCO GU 2026 demonstrated striking separation in post-trimodality therapy MFS according to ctDNA status (p<0.0001). Together, these studies suggest that integrating ctDNA with conventional clinical restaging may substantially refine risk stratification.

Dr. Mouw concluded that omission of immediate local therapy represents a safe and attractive strategy for carefully selected patients with MIBC who achieve cCR following systemic therapy. While a subset will ultimately require salvage radical cystectomy or radiation therapy, this approach may allow many patients to preserve their native bladder and avoid the toxicity and quality-of-life implications of definitive local treatment without compromising metastasis-free survival.
Taken together, this session underscored a rapidly evolving paradigm in MIBC management. Radical cystectomy remains the established standard and the foundation upon which the phase III EV+pembro data were generated. However, emerging prospective studies suggest that carefully selected patients achieving robust responses may be candidates for bladder preservation or even surveillance, with salvage therapy reserved for those who recur. As ongoing trials such as ARCHER and BRIGHT mature and biomarkers such as ctDNA become better validated, clinicians may soon be able to individualize local therapy after EV+pembro, balancing oncologic efficacy with organ preservation and quality of life.
Presented by:
- Leslie Ballas, MD, Professor, Department of Radiology, Director, Hematologic/Bone Marrow Transplant/Cellular Therapies Disease Research Group, Cedars-Sinai Medical Center, Los Angeles, CA
- Kelly Bree, MD, Assistant Professor, Department of Urology, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX
- Kent Mouw, MD, PhD, Assistant Professor of Radiation Oncology, Harvard Medical School, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:- Vulsteke C, Adra N, Danchaivijitr P, et al. Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer. N Engl J Med. 206;394:1257-1269.
- Galsky MD, Pérez-Valderrama B, Maruzzo M, et al. Neoadjuvant and Adjuvant Enfortumab Vedotin Plus Pembrolizumab for Participants With Muscle-Invasive Bladder Cancer Who Are Eligible for Cisplatin: Randomized, Open-Label, Phase 3 KEYNOTE-B15 Study. J Clin Oncol. 2026;44(7 Suppl):LBA630.
- deVere White RW, Lara Jr PN, Goldman B, et al. A Sequential Treatment Approach to Myoinvasive Urothelial Cancer: A Phase II Southwest Oncology Group Trial (S0219). J Urol. 2009; 181(6):2476-2481.
- Geynisman DM, Anderson CB, Wong YN, et al. Phase II Trial of Risk-Enabled Therapy After Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer (RETAIN 1). J Clin Oncol. 2025;43(2):180-189.
- Geynisman DM, Wong YN, Anderson CB, et al. A Phase 2 Trial of Risk Enabled Therapy After Neoadjuvant Chemo-Immunotherapy for Muscle-Invasive Bladder Cancer (RETAIN-2). J Clin Oncol. 2025;43(5 Suppl):815.
- Roessler N, Miszczyk M, Gontero P, et al. Clinical Complete Response as a Surrogate for Pathological Response in Bladder Cancer: A Systematic Review and Meta-Analysis. BJU Int. 2026.
- Galsky MD, Daneshmand S, Izadmehr S, et al. Gemcitabine and Cisplatin Plus Nivolumab as Organ-Sparing Treatment for Muscle-Invasive Bladder Cancer: A Phase 2 Trial. Nat Med. 2023;29:2825-2834.