(UroToday.com) The 2026 American Urological Association annual meeting featured a non-invasive bladder cancer session and a presentation by Dr. Andrew Zganjar discussing results from the INVITE study, a phase Ib/II, single-arm trial of delivering intravesical therapy for bladder cancer in patients’ homes. Intravesical therapy is the mainstay of treatment for non-muscle invasive bladder cancer.
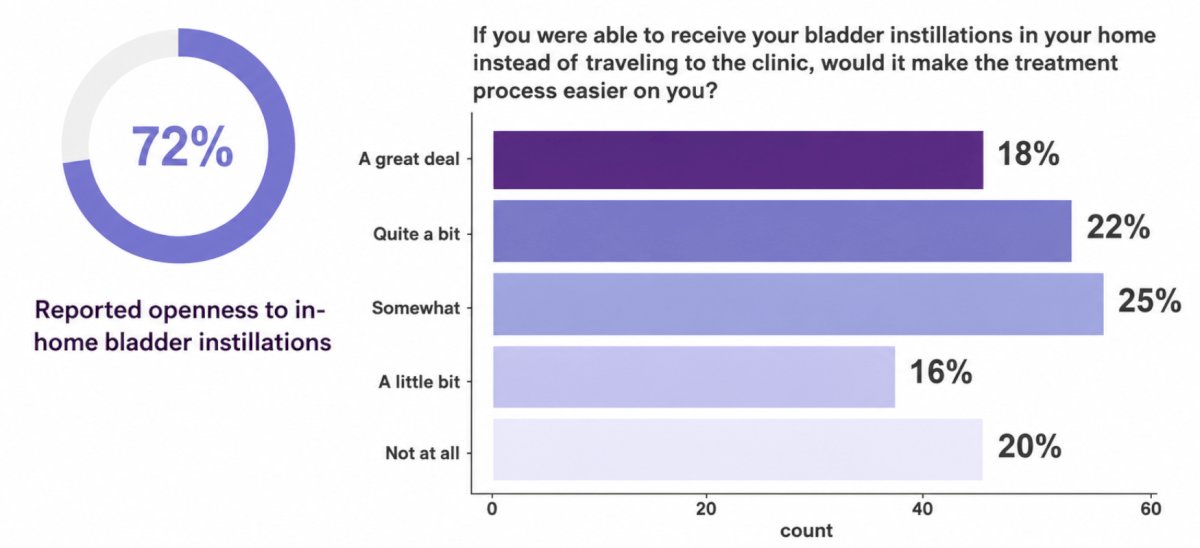
Regardless of agent used, this is a burdensome process requiring 6 weekly visits for induction therapy followed by 1-3 years of maintenance, annual upper tract imaging, and periodic cystoscopic surveillance. This treatment schedule is demanding and can be disruptive to the lives of patients and their caregivers due to the considerable time, travel, and financial toxicity associated with treatment. Indeed, the quality of life of non-muscle invasive bladder cancer patients declines over time, and maintenance intravesical therapy is discontinued at rates higher than expected from adverse events alone. One potential solution to decrease the treatment burden for our patients is in-home administration of intravesical therapy, meeting our patients where they are to deliver their cancer treatment in a location more convenient for them. Dr. Zganjar and colleagues recently conducted a survey of bladder cancer survivors across the US1 in which 55% traveled > 30 minutes one way for treatments, 33% paid >$25 out of pocket per treatment, 56% brought caregivers, 36% missed work, and 72% of respondents reported openness to receiving in-home intravesical therapy:
The objective of the INVITE trial, therefore, is to prospectively assess the safety and feasibility of delivering intravesical therapy in patients’ homes.
INVITE (NCT06704191) is a currently accruing single-arm, phase Ib/II study that aims to enroll 40 patients with cTa-T1N0M0 non-muscle invasive bladder cancer to receive induction intravesical therapy in their homes. Phase Ib has enrolled 10 patients beginning induction therapy with an eligible regimen (BCG, gemcitabine, mitomycin C, or sequential gemcitabine and docetaxel). Patients must live within 60 miles of the treatment center and be free of psychiatric illness or a social situation that precludes in-home treatment. Enrolled patients received the first dose of intravesical therapy in the brick and mortar clinic to ensure tolerability and then received doses 2-6 in their homes delivered by a network of contracted home care nurses.
The futility rate of the phase Ib portion was defined as 30%, which was met, allowing the investigators to proceed to a phase II expansion cohort that aims to accrue 30 additional patients beginning induction or maintenance intravesical therapy. The co-primary endpoints are safety, defined as the incidence, nature, and severity of adverse events, and feasibility, defined as the proportion of patients who receive at least 5 of 6 induction doses or 2 of 3 maintenance doses within 12 weeks of initiating intravesical therapy, with all prescribed in-home doses delivered in the home. The key secondary endpoint is patient satisfaction and willingness to recommend in-home intravesical therapy as assessed by a post-treatment questionnaire. Other secondary endpoints include global health-related quality of life, home days free of physical health care system contact, unplanned interactions with the urological care team, and 3- and 12-month disease-free survival rates. Accrual of 40 patients will provide 82% power to reject the null hypothesis that the proportion of patients who can successfully complete intravesical therapy in the home is 50% based on a two-sided Fisher’s exact test with α=0.05, assuming 72% of patients can successfully complete in-home therapy. The phase 2 trial design is as follows: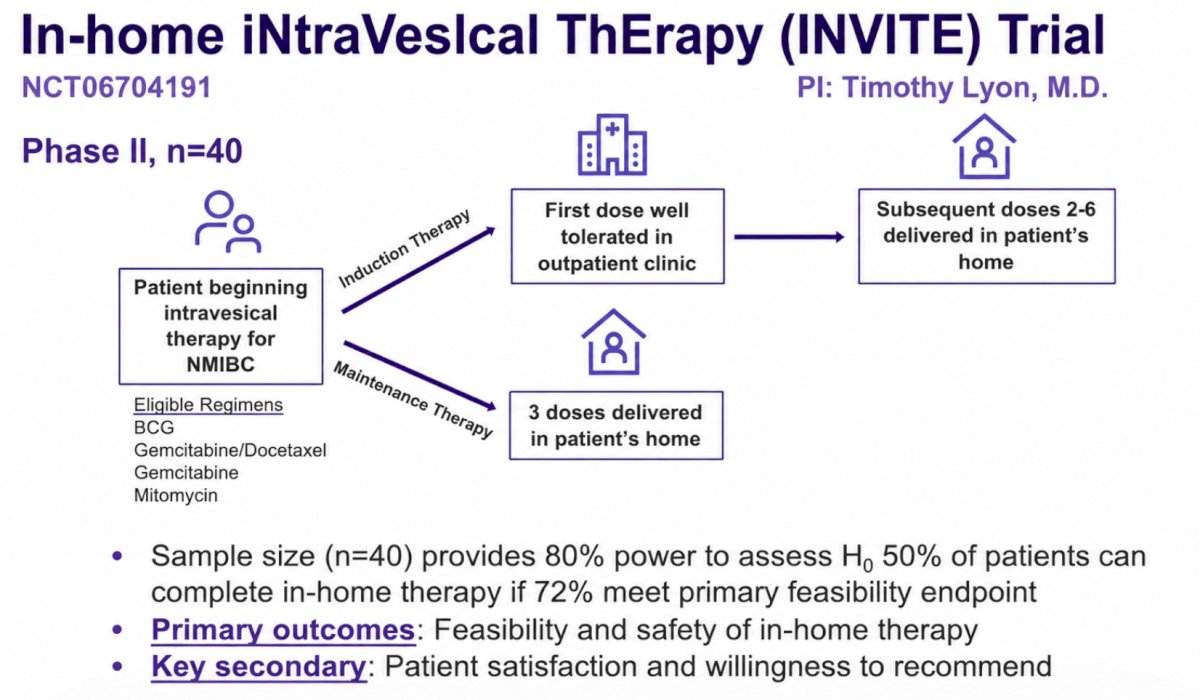
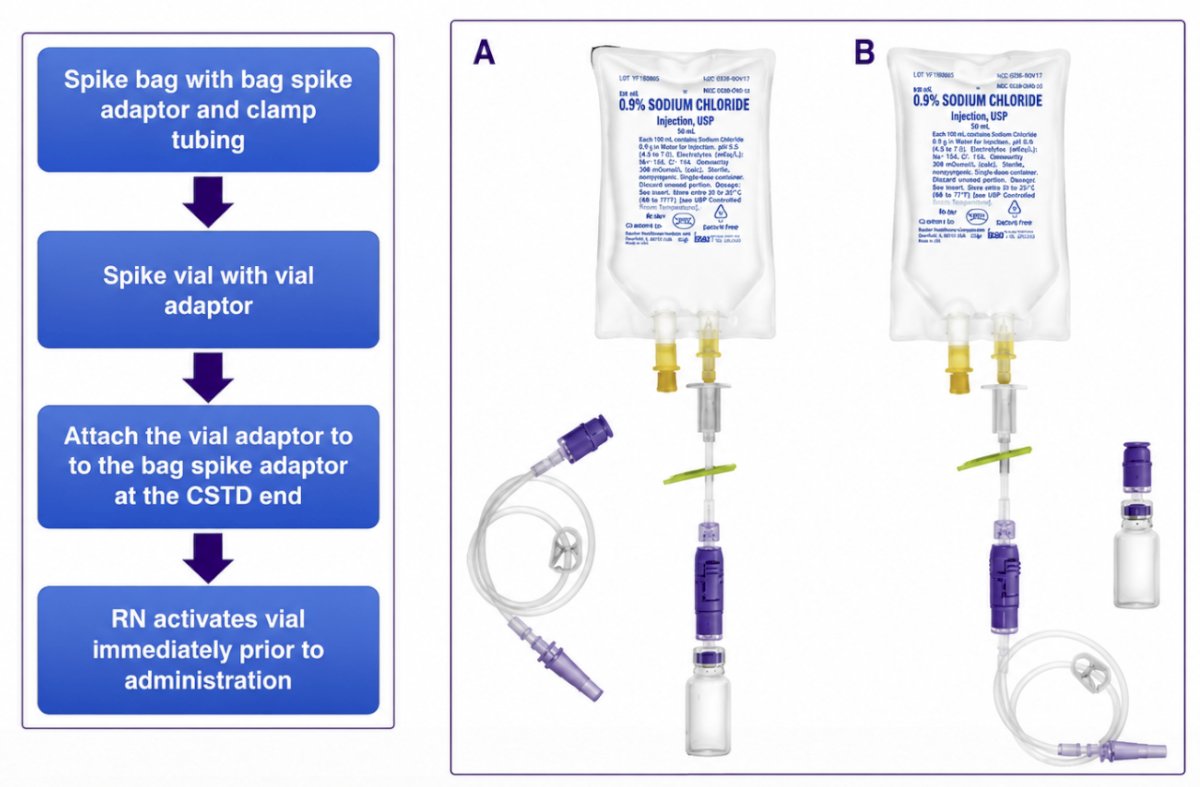
Dr. Zganjar also noted that they have developed an innovative delivery system for BCG bladder administration:
Dr. Zganjar concluded his presentation discussing results from the INVITE study with the following take-home points:
- Intravesical therapy is burdensome
- The INVITE trial is assessing the safety and efficacy of in-home intravesical therapy as a potential patient-centered solution
- As urologists, we owe it to our patients to develop innovative methods of care delivery to decrease time toxicity and improve the patient experience of bladder cancer treatment
- Data from INVITE are expected in Q4 2026.
Clinical Trials Registry Number: NCT06704191
Presented by: Andrew Zganjar, MD, Mayo Clinic, Jacksonville, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference:
- Myers A, Ristau B, Mossanen M, et al. Patient-reported treatment burden and attitudes towards in-home intravesical therapy among patients with bladder cancer. Urol Oncol. 2024 Feb;42(2):29.e17-29.