(UroToday.com) The 2026 AUA annual meeting featured a non invasive bladder cancer session and a presentation by Dr. Angela Smith discussing patient preferences, treatment received, and quality of life in the CISTO Study comparing radical cystectomy or bladder sparing therapy for recurrent high grade non muscle invasive bladder cancer. The CISTO Study demonstrated that most outcomes, including physical functioning, depression, anxiety, and overall quality of life, were similar or better 12 months after radical cystectomy compared with bladder sparing therapy for recurrent high grade non muscle invasive bladder cancer.1 There is limited evidence available to support the management of recurrent high grade non muscle invasive bladder cancer, which leads to uncertainty for patients and clinicians. To support decision-making in this setting, Dr. Smith and colleagues sought to understand how patient preferences impact treatment selection and outcomes.
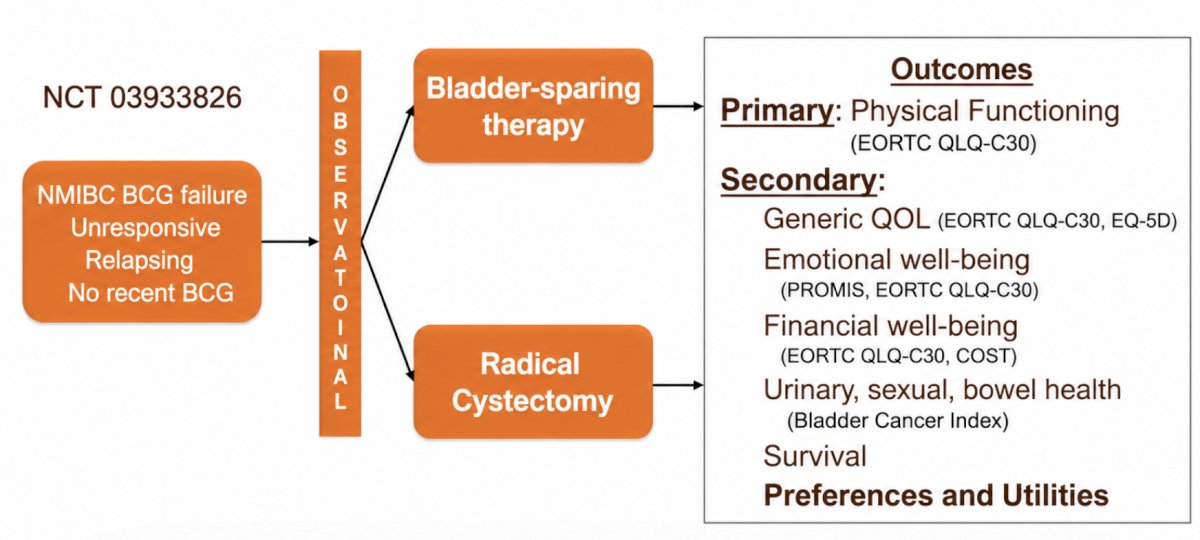
The CISTO Study is a pragmatic trial among patients with recurrent high grade non muscle invasive bladder cancer eligible for both radical cystectomy and bladder sparing therapy who selected their treatment. Baseline surveys assessed certainty of cure and willingness to accept treatment-related burdens in exchange for longevity. Health state utilities were calculated for three health states (anticipated retained/removed bladder, current health) at baseline and 12 months via electronic time tradeoff instruments. Treatment preference was defined as the anticipated health state with higher baseline utility. Correlations with treatment selected and the association between preference-treatment discordance and 12-month outcomes were evaluated. Semi structured interviews with patients, selected via purposive sampling, were analyzed using deductive coding to capture factors influencing treatment decisions and perspectives on quality of life impacts. The study design is as follows:
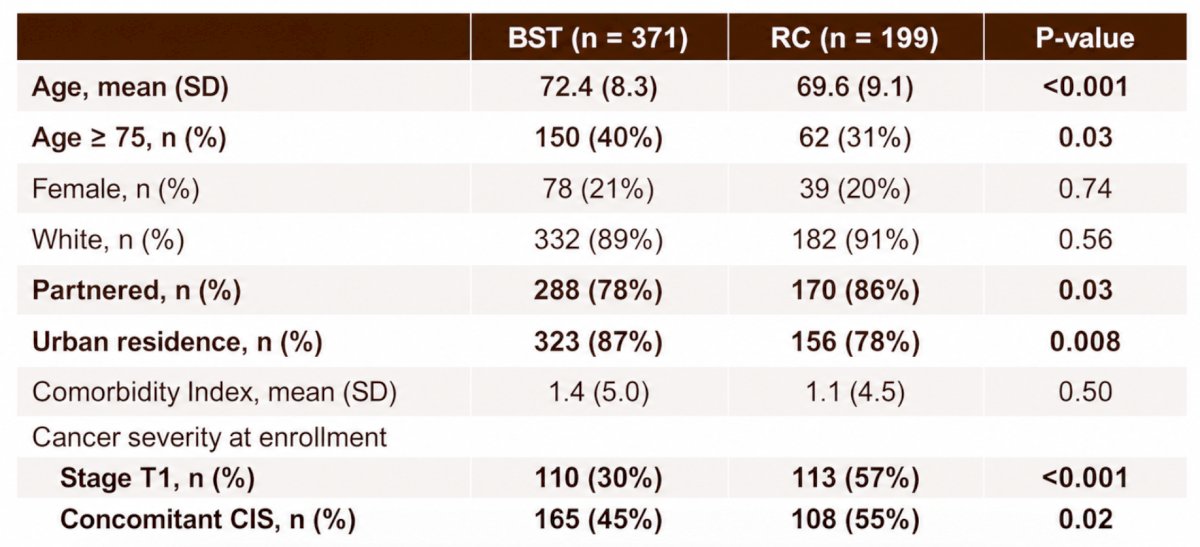
Among 570 participants, 371 selected bladder sparing therapy and 199 selected radical cystectomy. Patients undergoing radical cystectomy were significantly younger than those choosing bladder sparing therapy (mean 69.9 versus 72.4; p < 0.001):
Patients who selected radical cystectomy more often reported high certainty of cure (28% versus 14%) and willingness to undergo major surgery. Of 296 completing baseline time tradeoffs, 45% preferred a retained bladder, 18% preferred a removed bladder, and 37% had no preference. Treatment preferences strongly correlated with treatment chosen (radical cystectomy 68% who preferred removal, 48% with no preference, 15% who preferred retained):

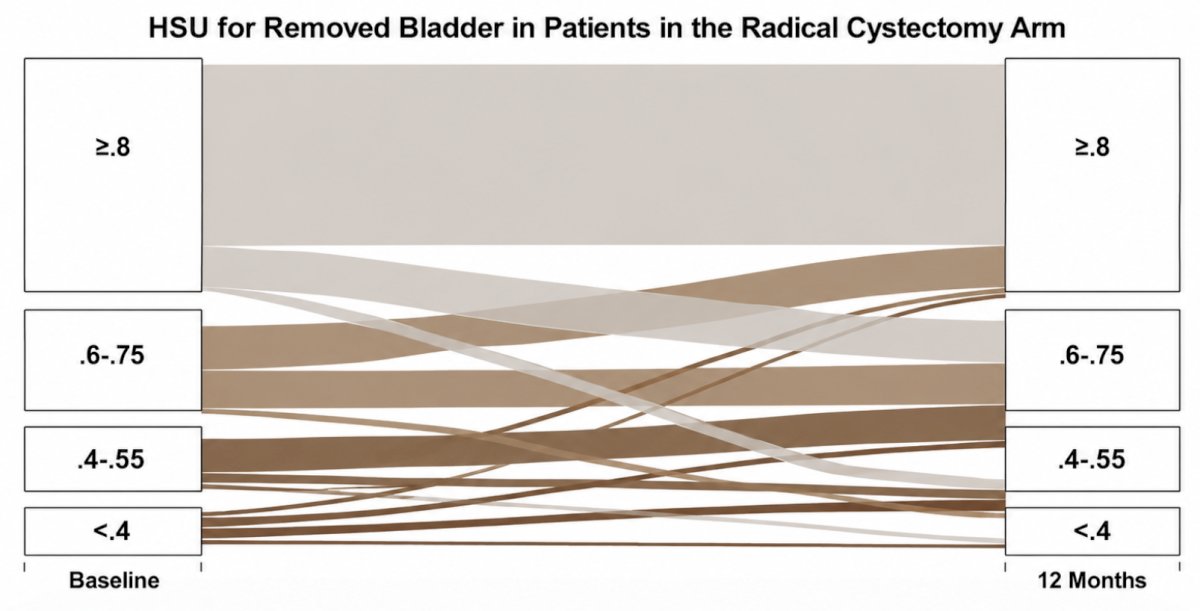
The following figure shows the health state uncertainty from baseline to 12 months for bladder removal in patients in the radical cystectomy arm:
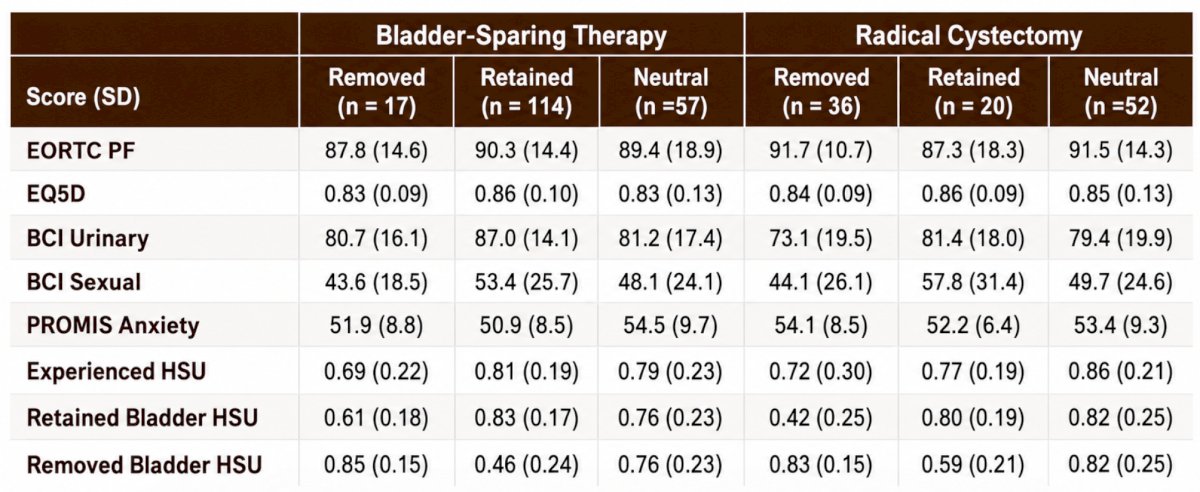
Preference-treatment discordance was not associated with 12-month outcomes:
Interviews revealed that participants who underwent radical cystectomy (n = 22) had unexpectedly strong physical recovery, improved emotional well-being, and relief from anxiety. Participants who chose bladder sparing therapy (n = 28) had a strong desire to avoid the quality of life impact of radical cystectomy, even if that meant burdensome surveillance or additional bladder treatments.
Dr. Smith concluded her presentation discussing patient preferences, treatment received, and quality of life in the CISTO Study with the following take home points:
- Patients made treatments choices largely aligned with their preferences for a retained or removed bladder
- Concordance of treatment with health state preferences was not associated with patient reported outcomes 12 months after CISTO enrollment
- Better delineation of expectations and outcomes with radical cystectomy using the CISTO study outcomes may help overcome biases against the removed bladder health state
Presented by: Angela Smith, MD, MS, University of North Carolina, Chapel Hill, NC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References: