(UroToday.com) The 2026 American Urological Association annual meeting featured a non-invasive bladder cancer session and a presentation by Dr. Yijun Shen discussing results from a randomized parallel cohort phase I/II study assessing intravesical versus intravenous therapy of camrelizumab in BCG-unresponsive high-risk non-muscle invasive bladder cancer. High-risk non-muscle invasive bladder cancer unresponsive to BCG remains difficult to manage.
Radical cystectomy offers the best chance of cure, but is associated with high perioperative morbidity and often refused by many patients. Immune checkpoint inhibitors have shown promise, but systemic administration is associated with substantial toxicity. This study, presented at AUA 2026, aimed to assess the efficacy and safety of intravesical therapy compared to intravenous therapy using camrelizumab, a PD-1 inhibitor, for BCG-unresponsive high-risk non-muscle invasive bladder cancer patients.
Phase I for this trial was a safety run-in to determine the maximum tolerated dose and recommended phase II dose of intravesical therapy with camrelizumab given weekly for 6 weeks at 100, 150, and 200 mg. In the phase II study, patients were randomized 1:1 to receive either intravenous camrelizumab (200 mg every 3 weeks) or intravesical camrelizumab therapy (200 mg weekly for 6 weeks, then every 3 weeks) for 2 years:
The primary endpoint was 3-month event-free survival. Secondary endpoints included 6- and 12-month high-grade recurrence-free survival, recurrence-free survival, progression-free survival, cystectomy-free survival, and safety. Exploratory immune analyses were performed using proteomic sequencing and multiplex immunofluorescence staining. Kaplan-Meier estimates were used for time to event outcomes, and differences were assessed by the log-rank test.
From June 2021 to March 2023, 24 patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer were enrolled. In the phase I study, no dose-limiting toxicities occurred at 200 mg, which was set as both the maximum tolerated dose and recommended phase II dose. With a median follow-up of 35.0 months (95% CI 31.97-41.69), the median event-free survival was 12.68 months (95% CI 6.31-not estimable) for the intravesical group and 3.09 months (95% CI 2.53-not estimable) for the intravenous group (log-rank p = 0.026):

The 3-, 6-, and 12-month event-free survival rates were 100.0%, 87.5%, and 57.1% in the intravesical group versus 58.3%, 29.2%, and 14.6% in the intravenous group, respectively. In a descriptive analysis of CIS patients, there were 3 patients in the intravesical group: 1 patient with T1 + CIS who had a positive 3 month urine cytology, and at 9 months had CIS recurrence; 1 patient with T1 + CIS who at 9 months had a CIS recurrence; 1 patient with CIS, who at 3 months had a positive urine cytology, and at 6 months had a CIS recurrence. There was 1 patient in the intravenous group with T1 + CIS who had a 3-month CIS recurrence.
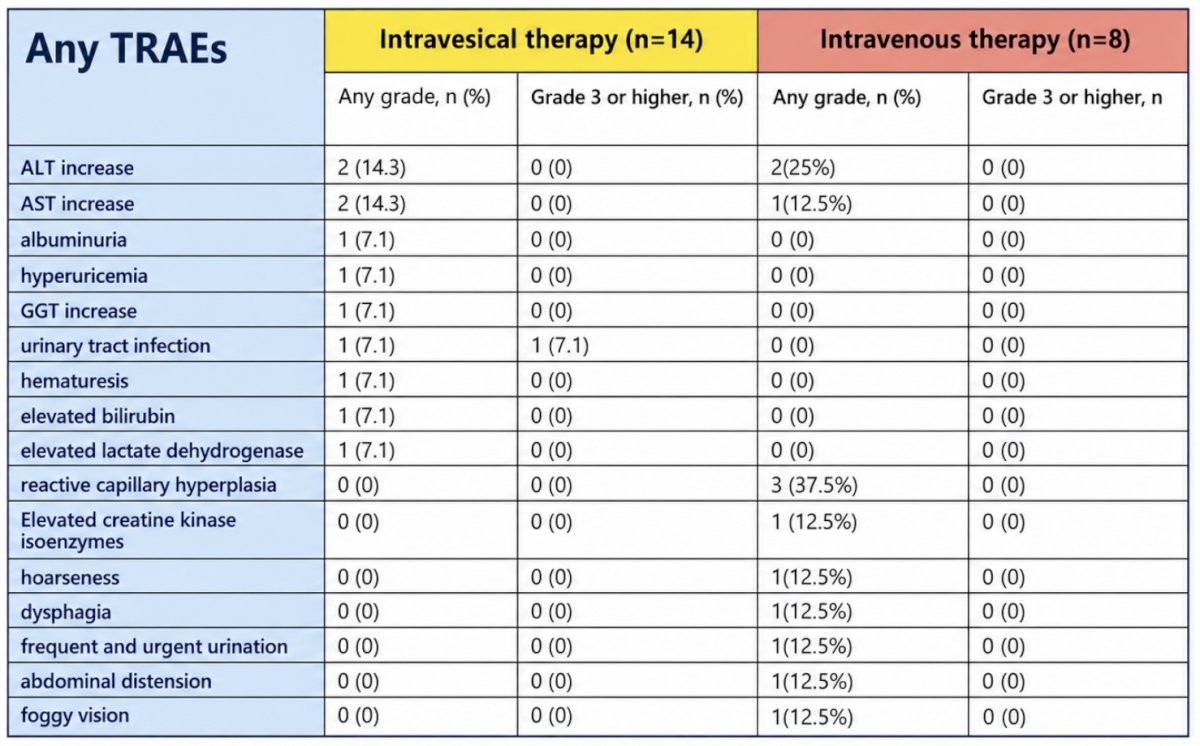
Treatment-related adverse events occurred in 21.4% of patients in the intravesical group, mostly grade 1 transaminase elevations, and one grade 3 urinary tract infection was observed. In the intravenous group, no grade 3 or higher treatment-related adverse events were reported, although three patients experienced reactive capillary hyperplasia, and several discontinued due to mild adverse events:
Exploratory immune analyses suggested that the superior efficacy of intravesical camrelizumab might be associated with localized immune activation and enhanced tumor-infiltrating lymphocyte responses. The following table provides a summary of available studies and treatments:

Dr. Shen concluded this presentation discussing results from a randomized parallel cohort phase I/II study assessing intravesical versus intravenous therapy of camrelizumab in BCG-unresponsive high-risk non-muscle invasive bladder cancer with the following take-home points:
- Intravesical administration of camrelizumab demonstrated longer event-free survival and a comparable safety profile compared with intravenous infusion in patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer
- These findings support further evaluation of intravesical PD-1 blockade as a bladder-preserving and potentially practice-changing immuno-therapeutic strategy
Presented by: Yijun Shen, Fudan University Shanghai Cancer Center, Shanghai, China
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.