(UroToday.com) The 2026 American Urological Association annual meeting featured a non-invasive bladder cancer session and a presentation by Dr. Joshua Meeks discussing a real-world evidence study assessing the prevalence and prognostic value of FGFR alterations in patients with intermediate risk non-muscle invasive bladder cancer. Non-muscle invasive bladder cancer comprises 75% of new bladder cancer diagnoses.
Clinicopathologic features (tumor grade, stage, size, multiplicity, and frequency of/time to recurrence) can be used to stratify non-muscle invasive bladder cancer into low, intermediate, and high risk disease, corresponding to risk of recurrence and progression, and to guide clinical management. Intermediate risk non-muscle invasive bladder cancer is associated with substantial burden on patients and healthcare resource utilization due to frequent recurrences and need for close surveillance, underscoring a need for new treatment options in this population. Fibroblast growth factor receptor (FGFR) alterations may function as oncogenic drivers in non-muscle invasive bladder cancer, yet data on the prevalence and prognostic value of FGFR alterations in the intermediate risk non-muscle invasive bladder cancer population remain limited. The objective of this study, presented at AUA 2026, was to characterize the prevalence of FGFR alterations and their association with recurrence-free survival across EAU risk groups and tumor grades using a real-world clinical and multi-omics non-muscle invasive bladder cancer dataset.
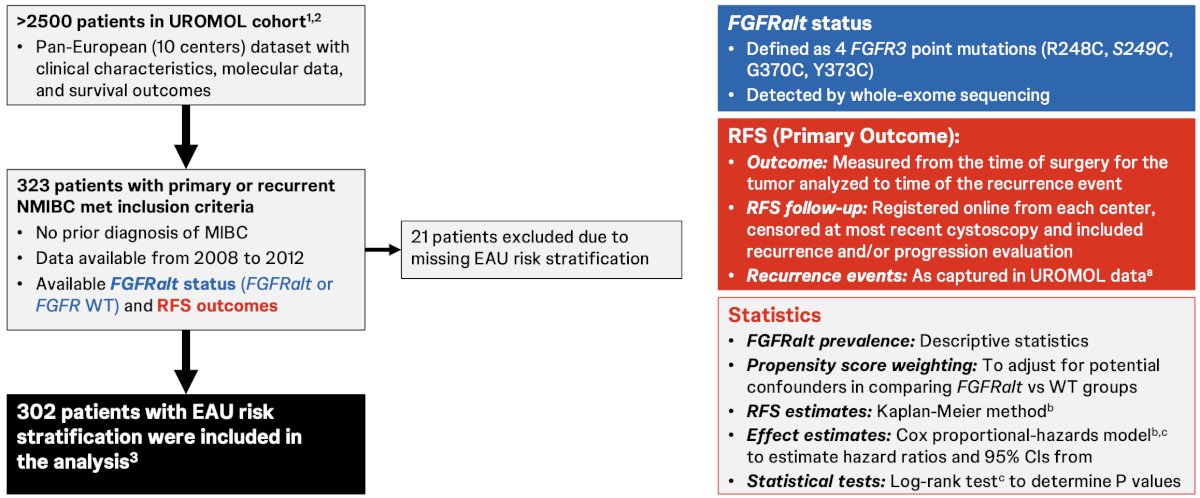
The UROMOL cohort is a pan-European dataset detailing clinical characteristics, molecular data, and survival outcomes from over 2,500 patients with bladder cancer. A curated set of 302 patients stratified by EAU risk groups with matched FGFR alterations positive status or FGFR wild type was analyzed. FGFR alteration positive status was defined as 4 susceptible FGFR3 point mutations detected by whole-exome sequencing. FGFR alterations prevalence was summarized using descriptive statistics. Recurrence-free survival in FGFR alterations versus FGFR wild-type subgroups in all patients and in patients with intermediate non-muscle invasive bladder cancer was estimated using the Kaplan-Meier method. The estimated hazard ratio and 95% CI were derived using the Cox proportional-hazards model, with FGFR alterations status as the sole independent variable. The p-value was obtained using the log-rank test. Ten patients with missing recurrence-free survival data (low risk, 1; intermediate risk, 3; high risk, 6) were excluded from the outcome analysis:
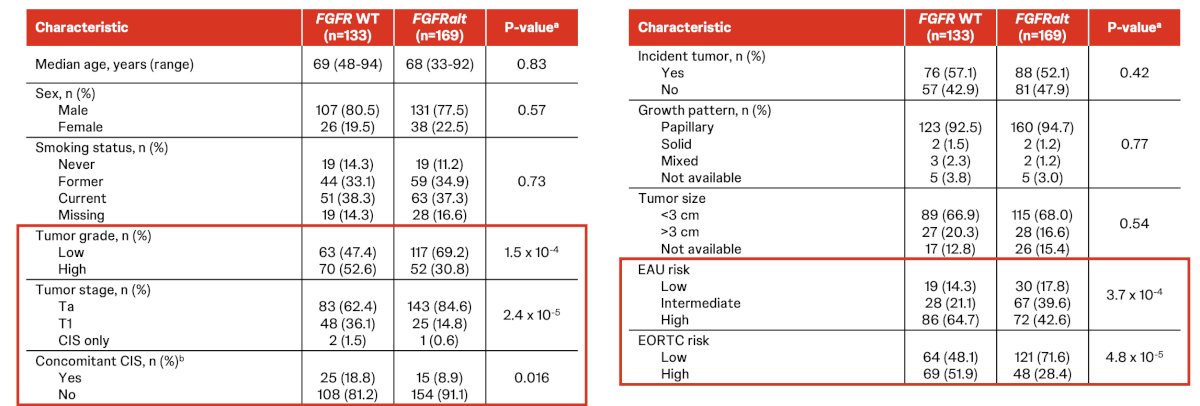
Overall, 56.0% of patients with non-muscle invasive bladder cancer had FGFR alterations, with the following baseline characteristics:
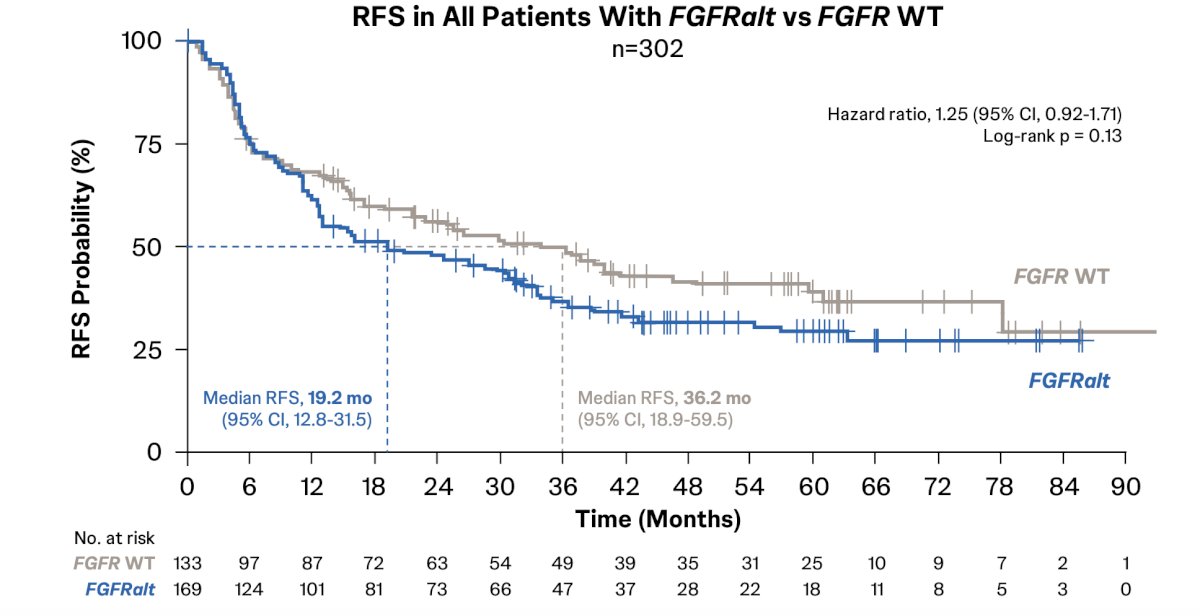
There was no significant difference in recurrence-free survival noted between patients with non-muscle invasive bladder cancer with FGFR alterations versus FGFR wild type (HR 1.25, 95% CI 0.92-1.71):
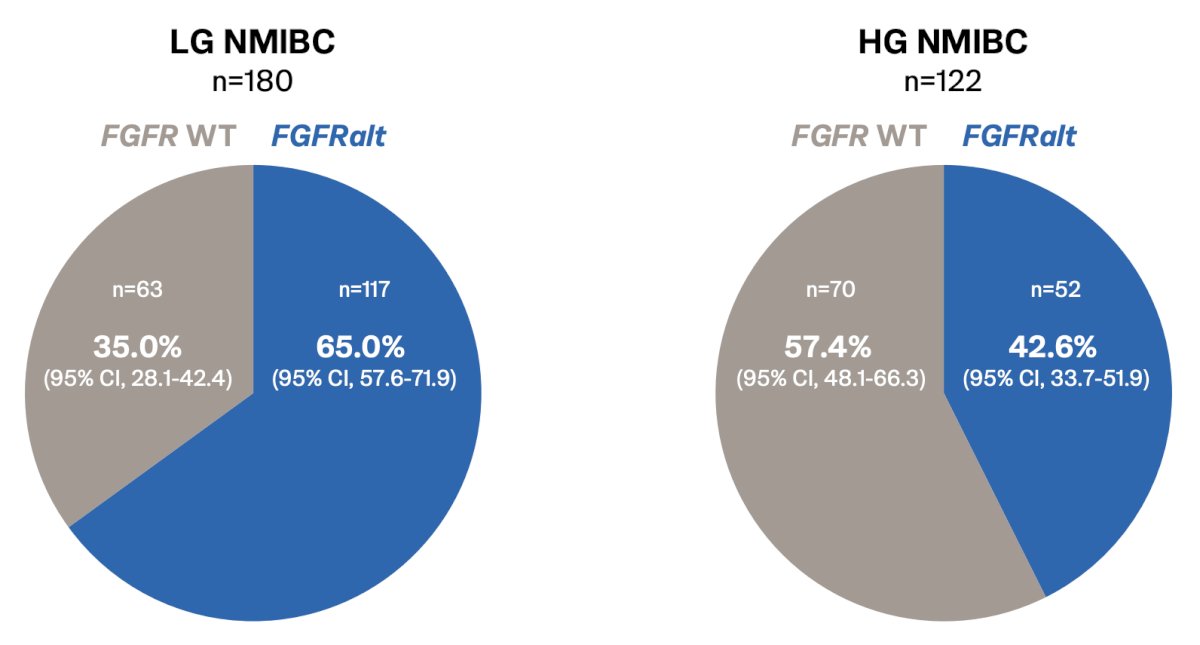
The prevalence of FGFR alterations by tumor grade included 65.0% in low-grade and 42.6% for high grade non-muscle invasive bladder cancer:
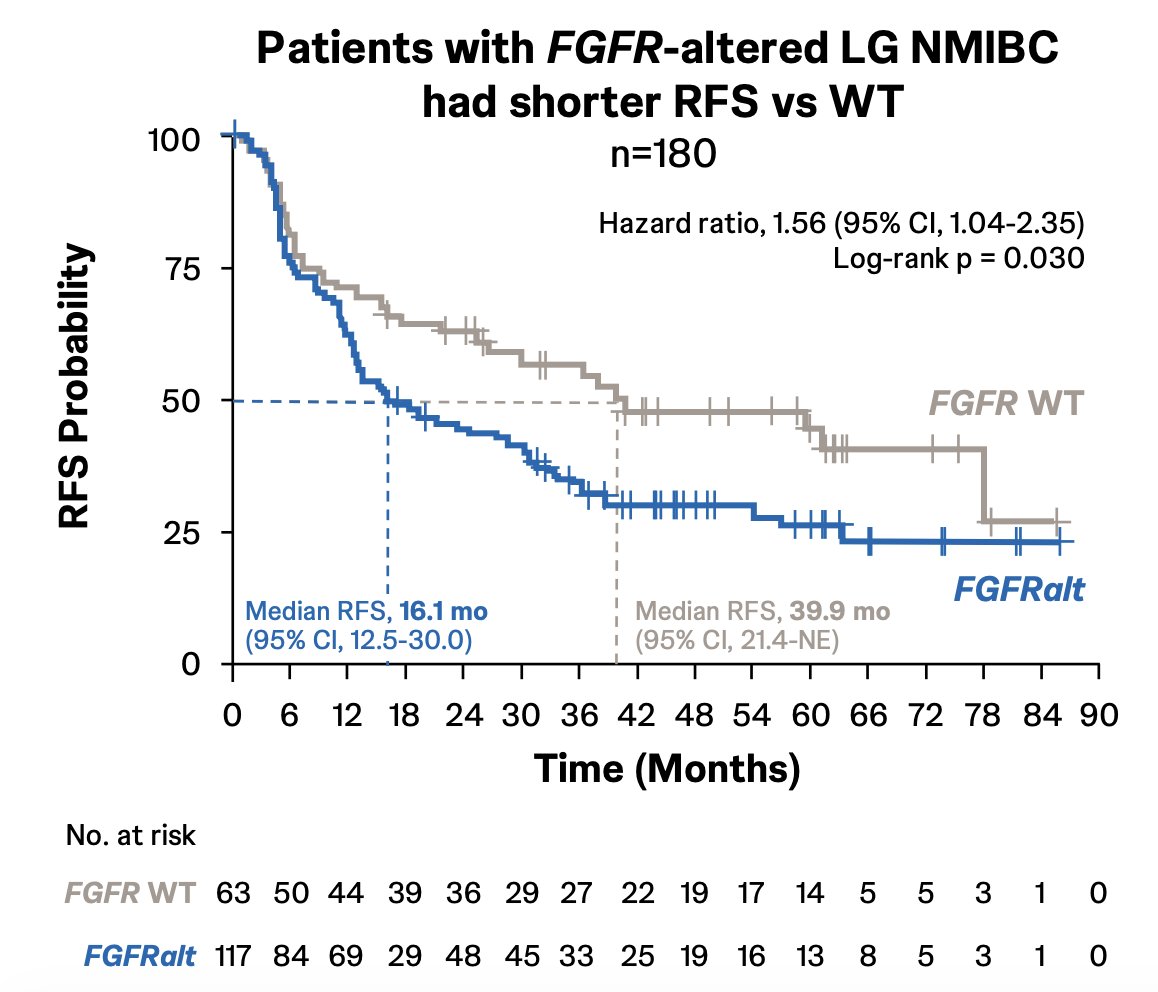
Dr. Meeks noted that patients with FGFR-altered low-grade non-muscle invasive bladder cancer had shorter recurrence-free survival versus wild-type patients (HR 1.56, 95% CI 1.04-2.35):
However, FGFR alterations were not associated with recurrence-free survival in high-grade non-muscle invasive bladder cancer (HR 0.88, 95% CI 0.54-1.43):

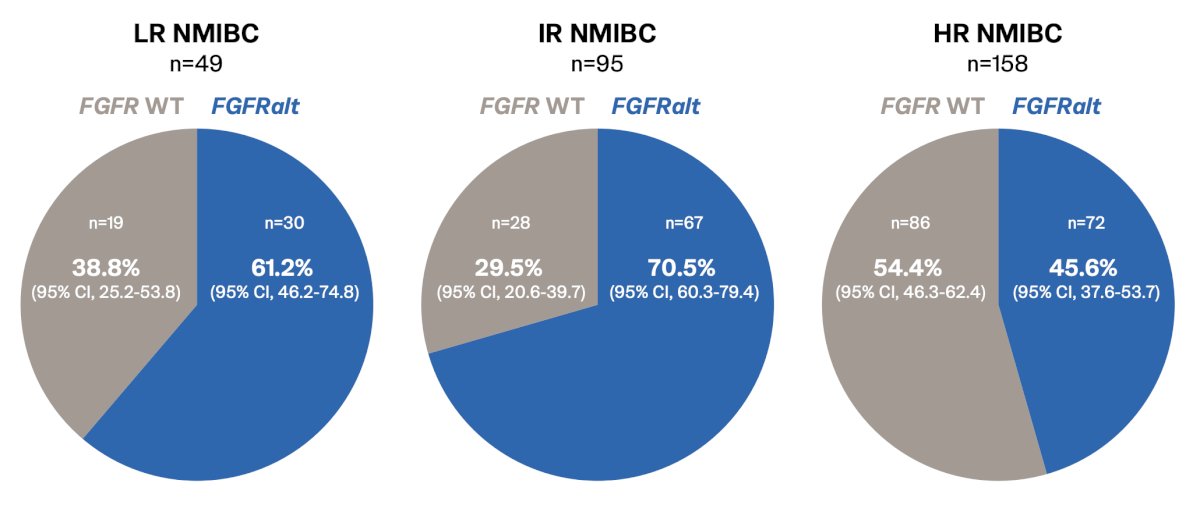
Regarding the prevalence of FGFR alterations by EAU risk category, low-risk non-muscle invasive bladder cancer had 61.2% alterations, intermediate risk 70.5%, and high risk 45.6%:
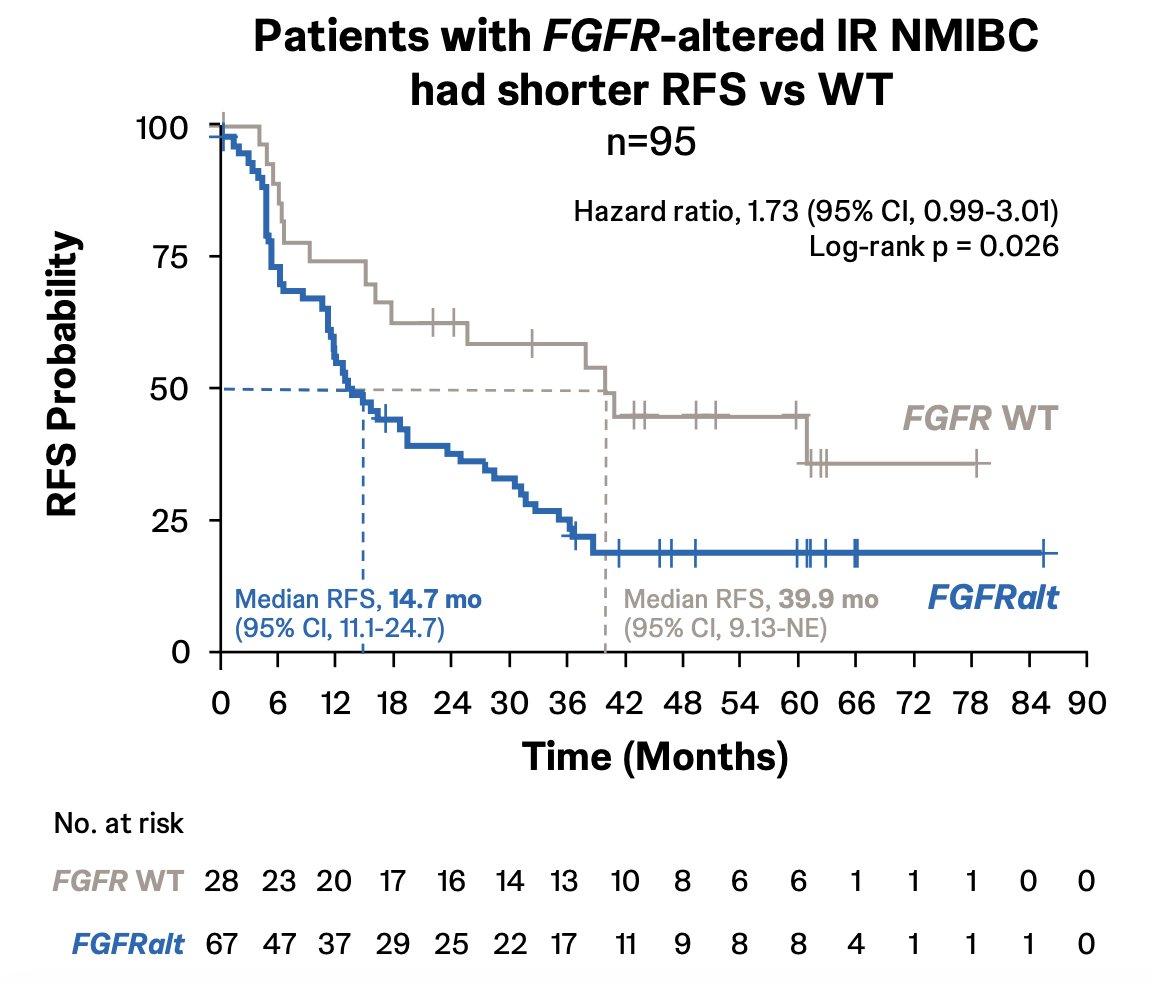
Patients with FGFR-altered intermediate-risk non-muscle invasive bladder cancer had shorter recurrence-free survival versus wild-type patients (HR 1.73, 95% CI 0.99-3.01):
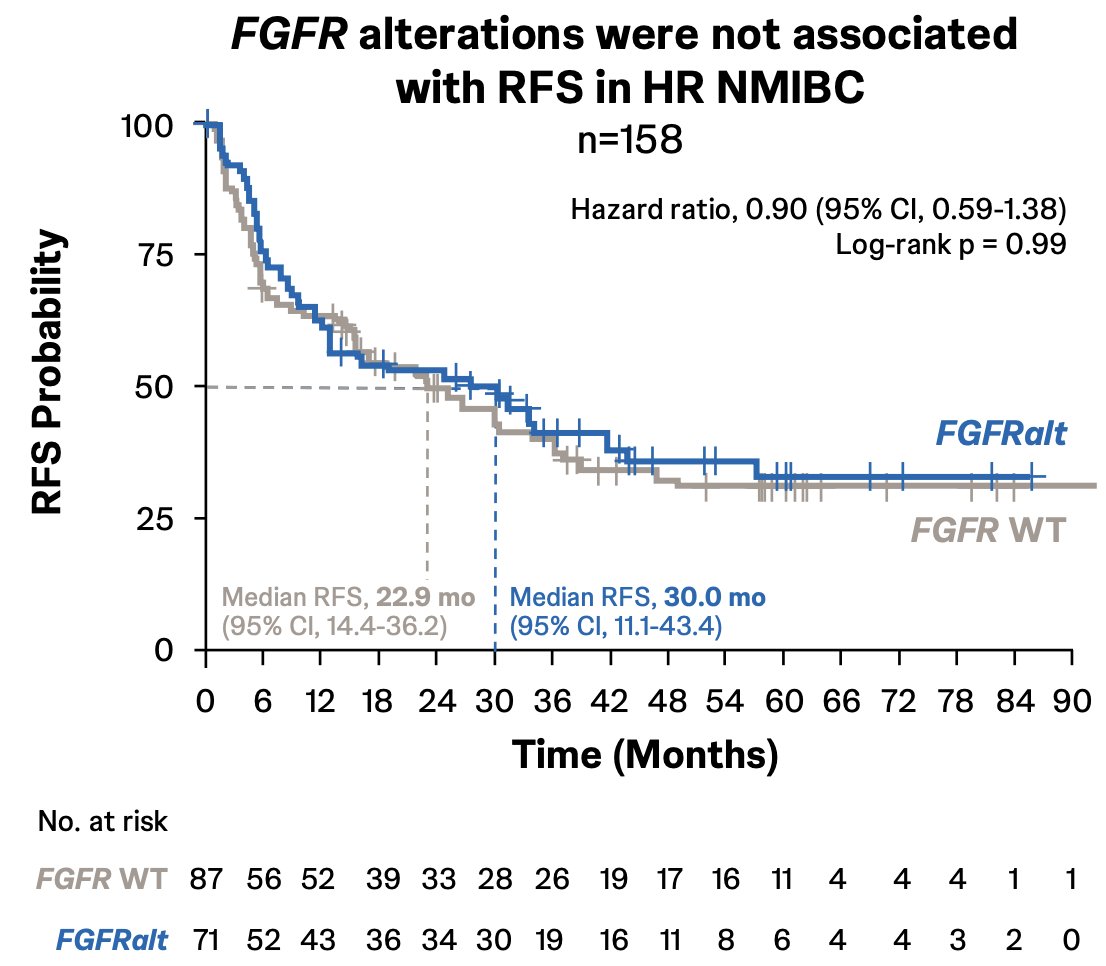
However, FGFR alterations were not associated with recurrence-free survival in high-risk non-muscle invasive bladder cancer (HR 0.90, 95% CI 0.59-1.38):
Dr. Meeks noted several limitations of this study, including (i) this being a retrospective analysis, (ii) FGFR fusions were not included in the FGFR status definition, (iii) treatment effects, including BCG, cannot be assessed, as the timing of treatments was not captured, and (iv) progression free survival data were insufficient in the database to be included in this analysis.
Dr. Meeks concluded his presentation discussing a real-world evidence study assessing the prevalence and prognostic value of FGFR alterations in patients with intermediate risk non-muscle invasive bladder cancer with the following take-home points:
- The analyzed FGFR alterations in this study were prevalent in patients with non-muscle invasive bladder cancer
- FGFR alterations were associated with shorter median recurrence-free survival compared with FGFR wild type in patients with intermediate risk non-muscle invasive bladder cancer (EAU definition) and in patients with low-grade disease, suggesting a negative prognostic value for recurrence
- In patients with high-risk or high-grade non-muscle invasive bladder cancer, FGFR alterations were associated with similar recurrence-free survival compared with FGFR wild type
- In the first in-human study (NCT05316155), erda-iDRS showed preliminary efficacy in patients with recurrent intermediate risk non-muscle invasive bladder cancer (complete response rate, 89%) or with BCG-treated high-risk non-muscle invasive bladder cancer (12-month recurrence-free survival rate, 83%) with select FGFR alterations
- Erda-iDRS is under investigation in the ongoing MoonRISe-1 (NCT06319820)
- MoonRISe-2 (NCT05316155, Part 4)
- MoonRISe-3 studies (NCT06919965)
Presented by: Joshua J. Meeks, MD, PhD, Oncologist, Associate Professor of Urology, Biochemistry and Molecular Genetics, Northwestern University Feinberg School of Medicine, Jesse Brown VA Medical Center in Chicago, Chicago, IL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.