(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to the annual AUA-International Bladder Cancer Group (IBCG) bladder cancer forum. Following a case presentation by Dr. Stephen Boorjian, Drs. Janet Kukreja and Leslie Ballas debated the timely topic of managing toxicities following radiation therapy within the context of trimodality therapy (TMT) for muscle-invasive bladder cancer (MIBC) – who and how?
The session began with Dr. Boorjian presenting a representative clinical case of a 71-year-old man with gross hematuria and mild-to-moderate irritative lower urinary tract symptoms. Imaging demonstrated normal upper urinary tracts without lymphadenopathy, and transurethral resection revealed a 3 cm sessile lesion on the right bladder wall with pathology confirming muscle-invasive urothelial carcinoma. Chest imaging was negative. Although the patient expressed strong interest in bladder preservation with TMT, he raised several practical questions regarding the potential “fallout” of treatment, including the likelihood of long-term urinary dysfunction, the risk of ultimately requiring cystectomy because the bladder “doesn’t work,” non-urinary quality-of-life consequences, management of intravesical recurrence, and, most importantly, who would serve as the “quarterback” coordinating management of treatment-related toxicities.
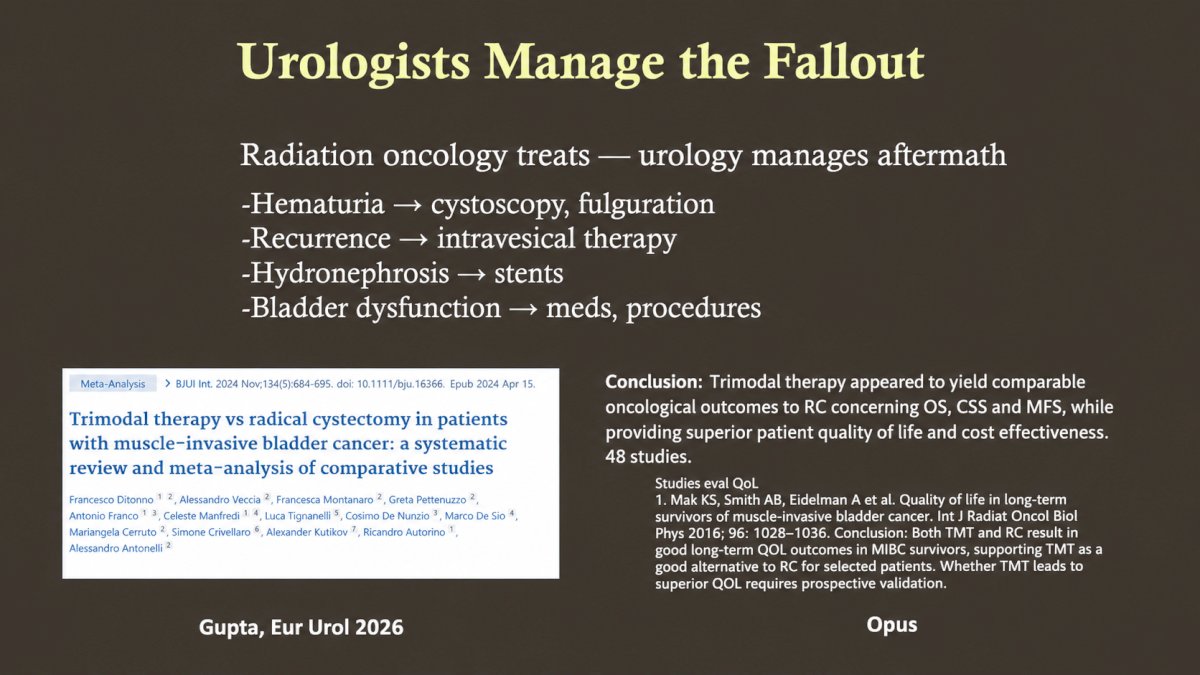
Dr. Janet Kukreja, a urologist at The University of Colorado, argued that radiation toxicity is real and that the burden of managing these complications largely falls on patients and urologists. She emphasized that while TMT is an effective oncologic strategy, treatment-related toxicity is often under-discussed and under-owned. According to Dr. Kukreja, patients frequently assume that preserving the bladder means preserving normal bladder function; however, the reality may include chronic lower urinary tract symptoms, recurrent hematuria, radiation-induced fibrosis, repeated procedures, recurrent non–muscle-invasive bladder cancer, and the need for additional intravesical therapies in an already compromised bladder.
Dr. Kukreja also highlighted the financial implications of bladder preservation, citing evidence that one-year management costs may exceed $200,000 and can surpass those associated with radical cystectomy because of higher outpatient utilization, imaging, and medication costs.1 In her view, although radiation oncology delivers treatment, urologists are often responsible for managing the aftermath:
- Hematuria requiring cystoscopy and fulguration
- Recurrences necessitating TURBT and intravesical therapy
- Hydronephrosis managed with ureteral stenting
- Bladder dysfunction treated with medications and procedural interventions
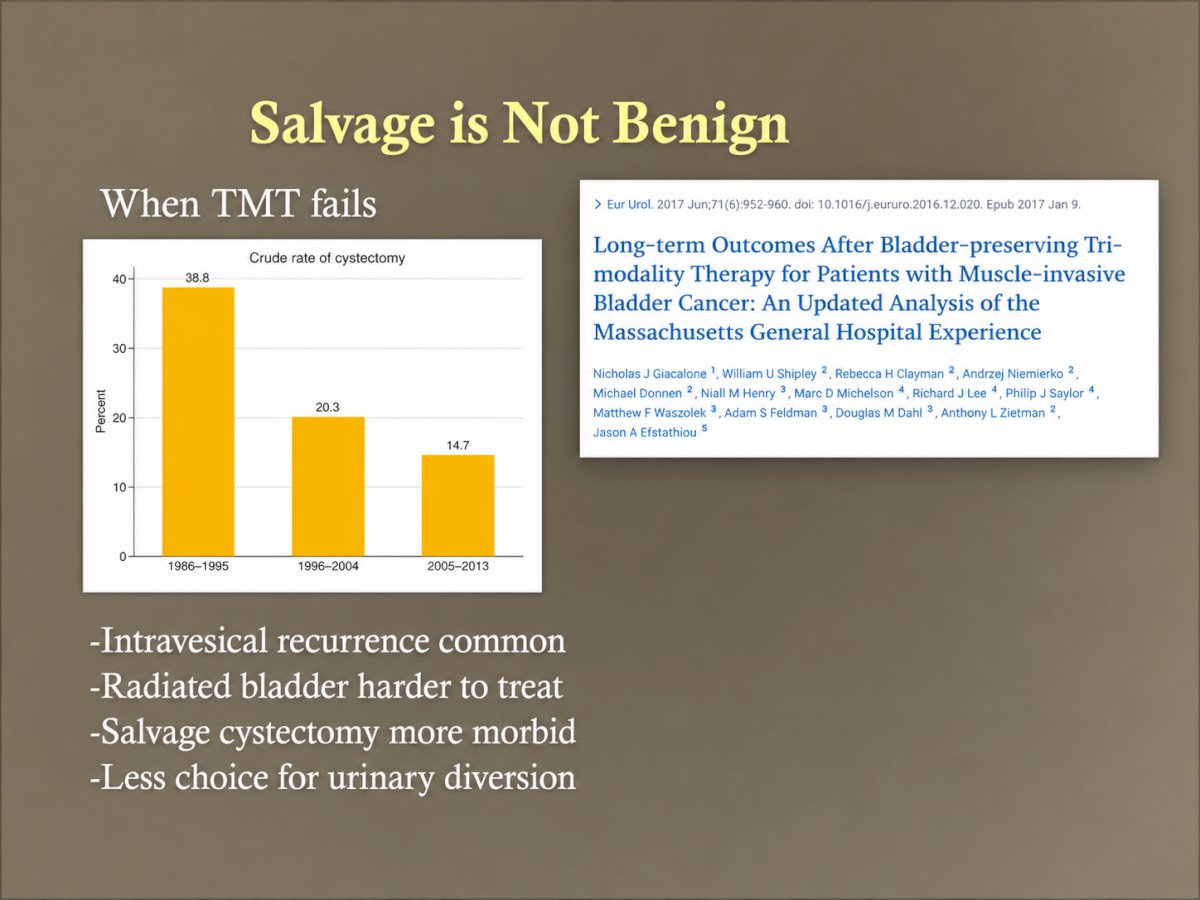
She cautioned that outcomes reported in prospective trials may not fully reflect real-world practice, where patients are older, have more comorbidities, and may receive less standardized care, potentially leading to a higher complication burden. Dr. Kukreja further stressed that salvage cystectomy is “not benign.” When TMT fails, intravesical recurrence is common, surgery in a radiated pelvis is technically more challenging, morbidity is increased, and urinary diversion options may be more limited. Her concluding message was that patients deserve candid counseling: toxicity is real and often chronic, management is ongoing, and urology remains central throughout the survivorship journey.
Dr. Leslie Ballas, a radiation oncologist at Cedars-Sinai Medical Center, presented the counterargument that toxicity should not be used as a reason to discourage appropriately selected patients from pursuing TMT. She emphasized that bladder preservation is associated with meaningful quality-of-life advantages and that responsibility for post-treatment care should be shared among all members of the multidisciplinary team.
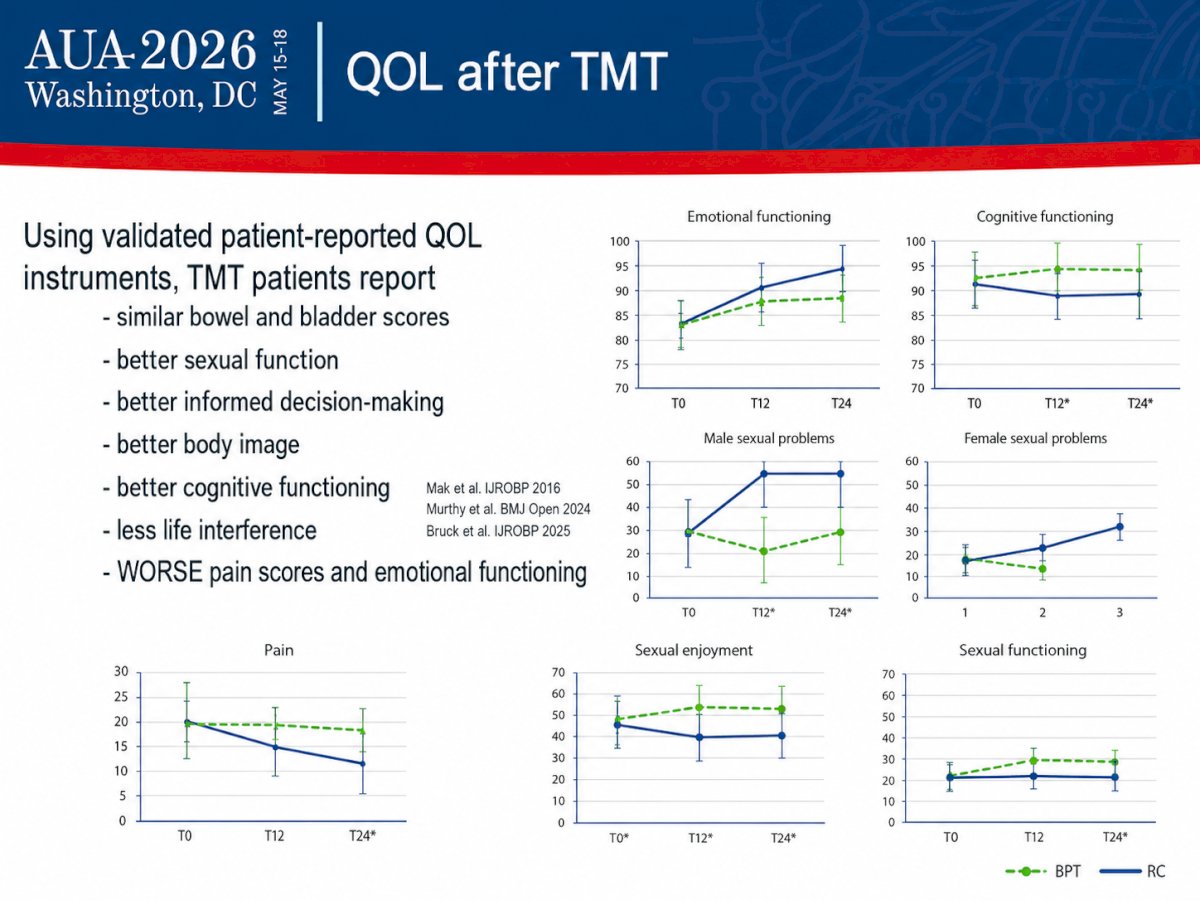
Using validated patient-reported outcome instruments, Dr. Ballas reviewed data demonstrating that patients treated with TMT report similar bowel and urinary function compared with those undergoing radical cystectomy, while experiencing better sexual function, improved body image, enhanced cognitive functioning, more informed decision-making, and less interference with daily life.2-4 She acknowledged that some studies have reported worse pain scores and emotional functioning, but overall quality-of-life metrics favor bladder preservation.
Addressing concerns regarding delayed surgery, Dr. Ballas noted that salvage cystectomy due to a contracted bladder occurs in only 1–2% of patients, while salvage cystectomy for recurrent muscle-invasive disease has remained consistently below 15% in contemporary series since 2005. Non–muscle-invasive recurrences occur in approximately 20% of patients and can often be effectively managed with intravesical therapy.5
Dr. Ballas emphasized that minimizing toxicity begins with thoughtful patient selection. Favorable features for either radical cystectomy or TMT include good performance status, clinical T2 disease, and unifocal tumors. Factors that may favor radical cystectomy include poor baseline bladder function, inflammatory bowel disease, and prior pelvic radiation. Conversely, TMT may be particularly attractive for patients at high surgical risk or those with a strong desire to preserve their native bladder. Unfavorable features for either strategy include carcinoma in situ, hydronephrosis, T3–T4 disease, multifocal tumors, poor renal function, and poor performance status.

She also highlighted advances in radiation technology and biomarker development, including image-guided and adaptive radiotherapy, improved treatment planning, and emerging miRNA and SNP-based signatures capable of identifying patients at elevated risk of radiation toxicity. These tools may allow increasingly personalized treatment approaches aimed at maximizing efficacy while minimizing adverse quality-of-life outcomes.
In addressing Dr. Boorjian’s central question— “Who’s the quarterback?”—Dr. Ballas argued that there should not be a single quarterback. Rather, all providers should follow patients more closely, and optimal care requires communication, collaboration, and leveraging each specialty’s expertise. In her view, urologists, radiation oncologists, and medical oncologists should function as an integrated team to monitor patients and manage treatment-related complications.
This debate underscored the increasing importance of multidisciplinary collaboration as bladder-preserving approaches continue to gain momentum in the management of muscle-invasive bladder cancer. Dr. Kukreja emphasized that while TMT is oncologically effective, its downstream toxicities are genuine, often chronic, and frequently managed by urologists, who remain central to patient care long after treatment is completed. Dr. Ballas countered that toxicity should not deter clinicians from recommending TMT to appropriately selected patients, highlighting favorable quality-of-life outcomes, low contemporary rates of salvage cystectomy, and ongoing advances in radiation delivery and biomarker-driven risk stratification.
Ultimately, both speakers converged on a common principle: patients considering trimodality therapy deserve comprehensive counseling regarding not only oncologic outcomes, but also the functional, quality-of-life, and survivorship implications of treatment. Regardless of who is labeled the “quarterback,” successful bladder preservation depends on close communication and coordinated care among urology, radiation oncology, and medical oncology.
Presented by:
- Stephen Boorjian, MD, Carl Rosen Professor and Chair of the Department of Urology, Mayo Clinic, Rochester, MN
- Janet Kukreja, MD, MPH, Associate Professor, Division of Urology, University of Colorado Anschutz School of Medicine, Denver, CO
- Leslie Ballas, MD, Professor, Department of Radiology, Director, Hematologic/Bone Marrow Transplant/Cellular Therapies Disease Research Group, Cedars-Sinai Medical Center, Los Angeles, CA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:- Scilipoti P, Moschini M, Li R, et al. The Financial Burden of Localized and Metastatic Bladder Cancer. Eur Urol. 2025;87(5):536-550.
- Mak RH, Hunt D, Shipley WU, et al. Long-Term Outcomes in Patients With Muscle-Invasive Bladder Cancer After Selective Bladder Preservation by Combined-Modality Therapy: A Pooled Analysis of Radiation Therapy Oncology Group Protocols. Int J Radiat Oncol Biol Phys. 2016;94(1):67-74.
- Murthy V, Tree AC, Huddart RA, et al. International Consensus on Clinical Trial Design for Bladder Preservation in Muscle-Invasive Bladder Cancer. BMJ Open. 2024;14:e086666.
- Bruck O, Murthy V, Huddart RA, et al. End Points for the Next-Generation Bladder-Sparing Perioperative Trials for Patients With Muscle-Invasive Bladder Cancer. Int J Radiat Oncol Biol Phys. 2025;123(3 Suppl):S1-S8.
- Zlotta AR, Ballas LK, Niemierko A, et al. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: a multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023; 24(6):669-681.