(UroToday.com) The American Urological Association's 2026 Annual Meeting, in Washington D.C., was host to the Clinical Trials in Progress: Bladder Cancer Session. Dr. Mark Tyson presented the trial in progress SWOG S2611 (ARCIS) A Randomized Comparison of Intravesical Therapies: A phase III study of cretostimogene grenadenorepvec/gemcitabine (CRETO-GEM) versus gemcitabine/docetaxel (GEM-DOCE) for the treatment of BCG-unresponsive and BCG-exposed NMIBC.
Dr. Tyson explained the rationale for the ARCIS trial in BCG-unresponsive NMIBC, emphasizing the continued need for durable bladder-sparing treatment strategies in this disease space. He noted that intravesical gemcitabine plus docetaxel (GEM-DOCE) has emerged as a commonly utilized community standard, although supporting data have largely been derived from non-randomized studies.
He further highlighted that the combination of cretostimogene plus gemcitabine (CRETO-GEM) represents a biologically rational therapeutic approach, supported by complementary mechanisms of action and encouraging early clinical activity. Given the absence of prospective head-to-head comparative evidence, the NCI CTEPM called for randomized data, leading to the development of ARCIS as an FDA-aligned phase 3 randomized controlled trial.
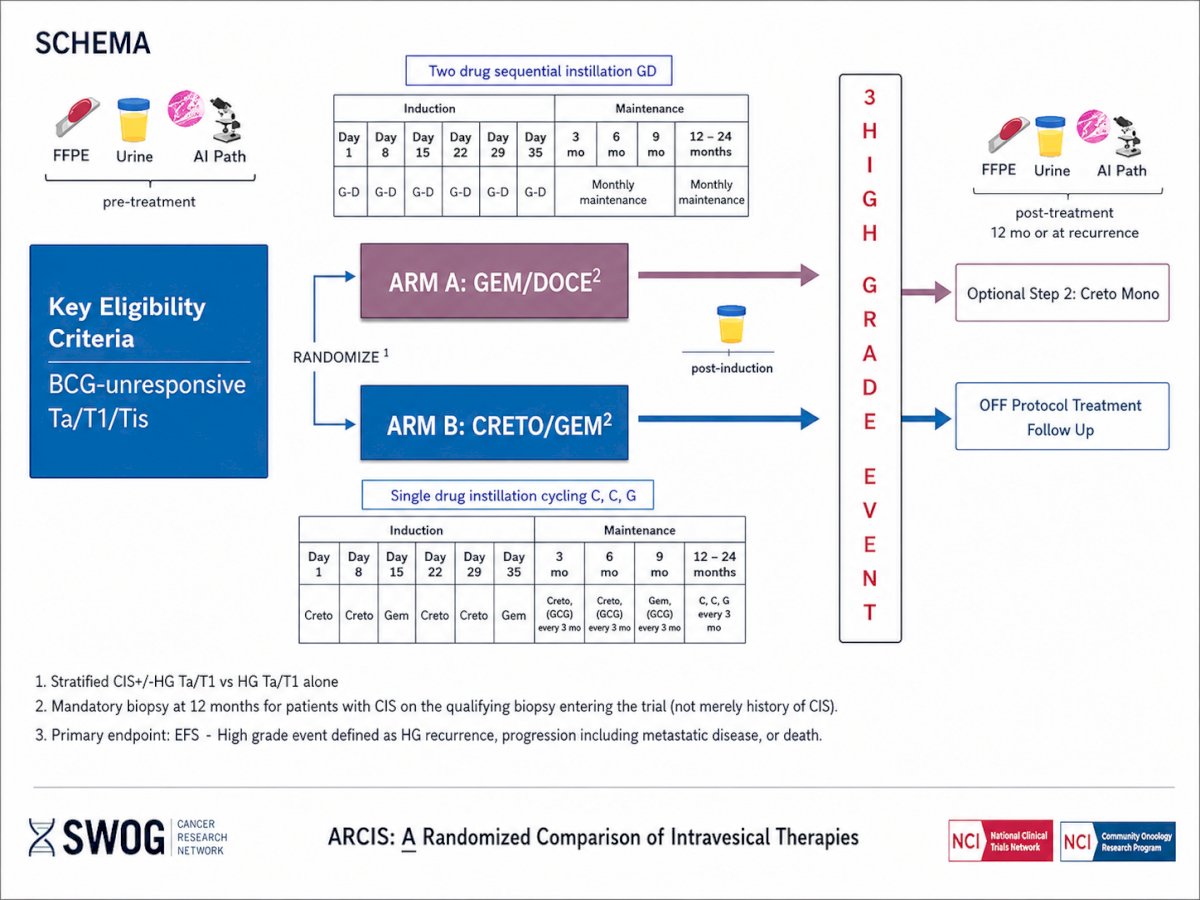
ARCIS is a randomized phase 3 trial evaluating intravesical GEM/DOCE versus CRETO/GEM in patients with BCG-unresponsive NMIBC, including Ta, T1, and Tis disease. Eligible patients undergo pretreatment specimen collection, including FFPE tissue, urine testing, and AI-assisted pathology assessment, prior to randomization in a 1:1 fashion to one of two treatment arms.
Arm A consists of sequential intravesical gemcitabine plus docetaxel (GEM/DOCE). During induction, patients receive weekly treatments on days 1, 8, 15, 22, 29, and 35. Maintenance therapy includes monthly instillations at months 3, 6, 9, and 12, followed by continued monthly maintenance from months 12 through 24. Arm B evaluates cretostimogene plus gemcitabine (CRETO/GEM) using a single-drug sequential cycling strategy during induction, alternating cretostimogene and gemcitabine weekly over 6 weeks. Maintenance therapy includes cretostimogene with or without gemcitabine administered every 3 months through 24 months.
Post-induction evaluation includes urine assessment, followed by ongoing surveillance for high-grade events. Patients who remain free of high-grade recurrence continue protocol therapy, whereas those with recurrence undergo post-treatment tissue and urine collection at 12 months or at the time of recurrence. An optional second step allows patients to receive cretostimogene monotherapy, while others transition to off-protocol treatment and follow-up.
The study stratifies patients according to the presence of CIS with or without high-grade Ta/T1 disease versus high-grade Ta/T1 disease alone. Mandatory biopsy at 12 months is required for patients with CIS identified on qualifying biopsy at trial entry. The primary endpoint is event-free survival, with high-grade events defined as high-grade recurrence, progression including metastatic disease, or death. The study schema is shown below:
Lastly, Dr. Tyson reviewed the statistical design of the ARCIS trial. The study is powered to detect an improvement in 2-year event-free survival from 40% with GEM/DOCE to 55% with CRETO/GEM, corresponding to a hazard ratio of 0.65. The trial was designed with a one-sided alpha of 0.023 and a statistical power of 87%. The planned sample size is 308 total patients, including approximately 140 patients per treatment arm, with an additional 10% enrollment cushion. Interim analyses are planned after 25%, 50%, and 75% of expected event-free survival events have occurred. Dr. Tyson also noted that drug supply and logistical support for the study are being provided by CG Oncology.
Presented by: Mark Tyson II, MD, MPH, Urologic Oncologist, Mayo Clinic, Scottsdale, AZ
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.