(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Society of Urologic Oncology (SUO) Session. Dr. Trinity Bivalacqua presented The First Results from CORE-008 Cohort CX- Phase 2 Study of Intravesical Cretostimogene Grenadenorepvec with Gemcitabine in Patients with High-Risk BCG-Exposed or BCG-Unresponsive Non-Muscle Invasive Bladder Cancer.
Dr. Bivalacqua began by highlighting the rationale for novel intravesical combination strategies in high-risk NMIBC. He noted that the efficacy and safety of cretostimogene monotherapy, as well as combinations with pembrolizumab in high-risk BCG-unresponsive NMIBC and nivolumab in MIBC, have previously been reported. Despite these encouraging results, he emphasized that additional intravesical therapeutic approaches leveraging complementary mechanisms of action and potential immune-modulating synergy remain needed in high-risk NMIBC.1,2
He noted that preclinical data demonstrated enhanced antitumor activity when cretostimogene was combined with gemcitabine compared with cretostimogene alone. In vitro studies across multiple bladder cancer cell lines showed improved treatment response with the combination strategy, along with increased G0/G1 cell-cycle arrest and higher rates of apoptosis, supporting a potential synergistic effect between these agents as shown below.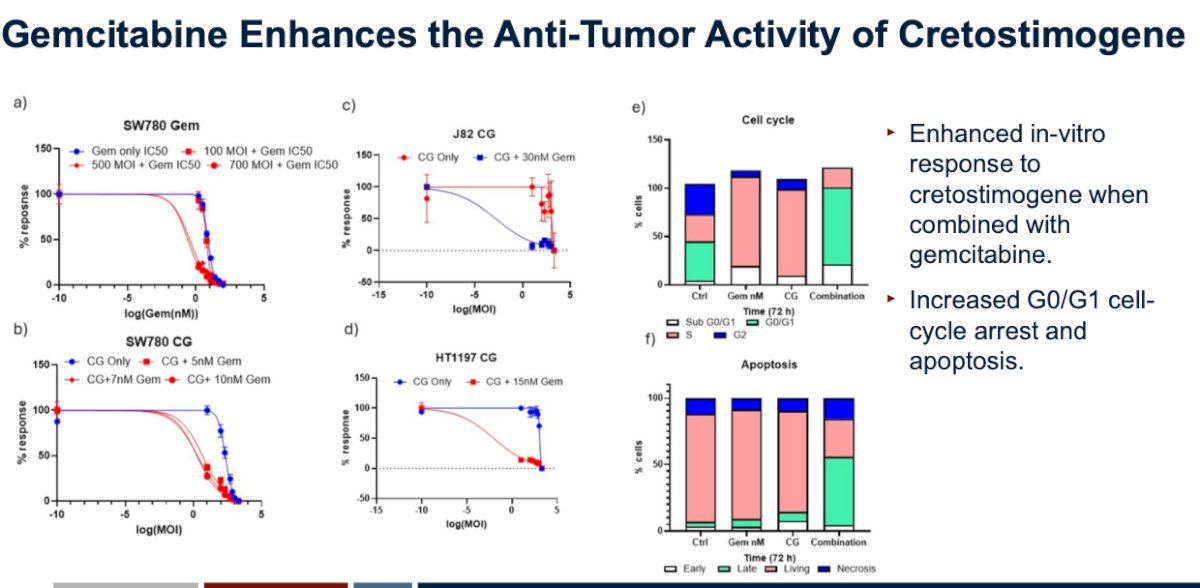
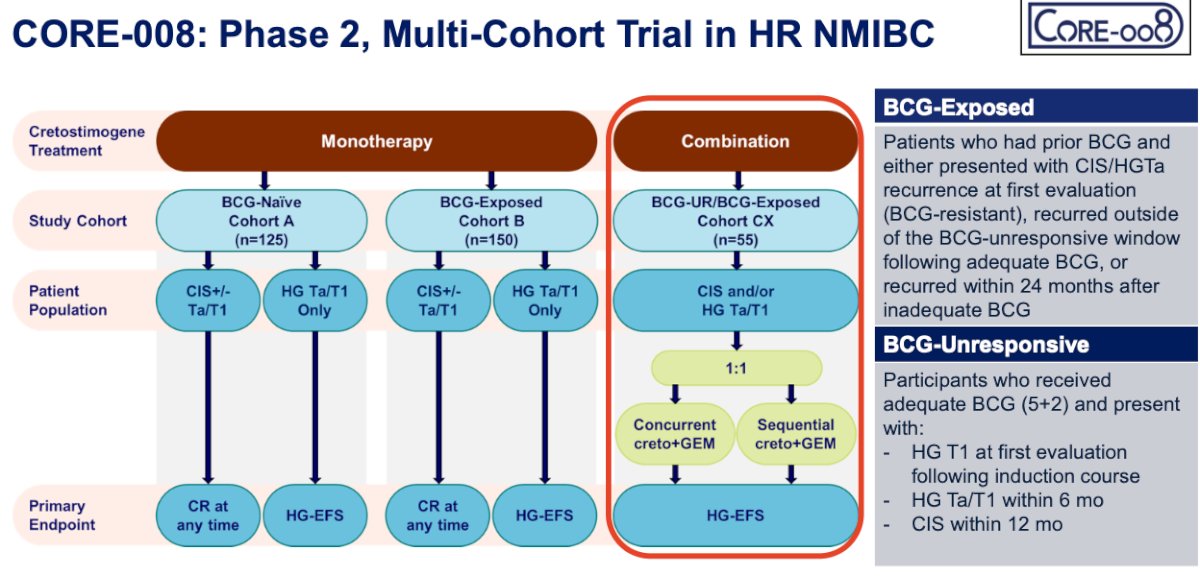
CORE-008 is an ongoing phase 2 multi-cohort study evaluating cretostimogene-based treatment strategies in patients with high-risk NMIBC. The trial includes both BCG-naïve and BCG-exposed cohorts receiving cretostimogene monotherapy, as well as a combination cohort for patients with BCG-unresponsive or BCG-exposed disease treated with cretostimogene plus gemcitabine. The combination cohort enrolled patients with CIS and/or high-grade Ta/T1 disease and evaluated both concurrent and sequential administration of cretostimogene with gemcitabine in a 1:1 design. Primary endpoints varied by cohort and included complete response at any time for CIS-containing disease and high-grade event-free survival for papillary-only disease.
Specifically, Cohort CX is investigating cretostimogene combined with intravesical gemcitabine in patients with BCG-exposed or BCG-unresponsive disease. This combination is hypothesized to provide synergistic anti-tumor activity through complementary immune-modulating mechanisms while maintaining an intravesical-only treatment approach aimed at minimizing systemic toxicity. The trial design is shown below.
Treatment was administered during both induction and maintenance phases using either a concurrent or sequential combination strategy. In the concurrent cohort, patients received intravesical cretostimogene and gemcitabine together during scheduled treatment visits. In the sequential cohort, treatment began with intravesical cretostimogene followed by gemcitabine administration. Induction consisted of 6 weekly instillations, followed by maintenance treatments administered every 3 months through 24 months, with extended maintenance and long-term follow-up thereafter.
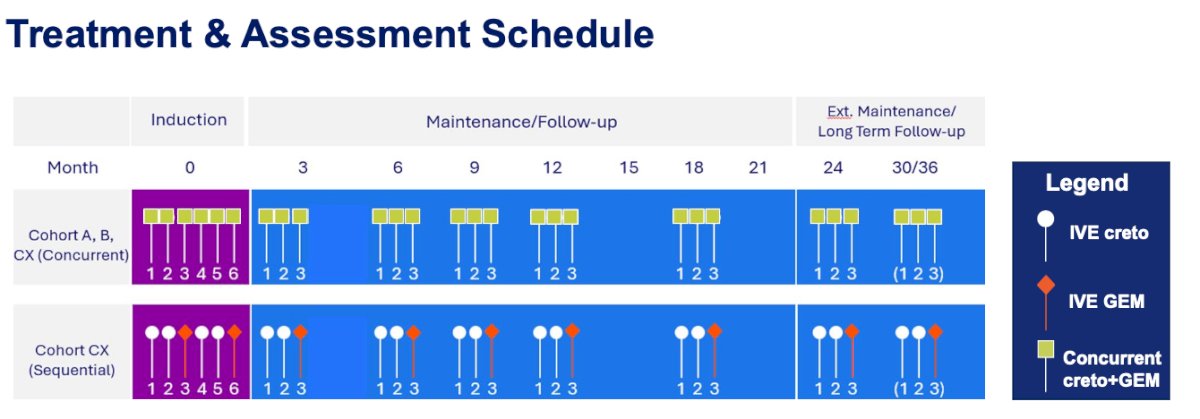
Dr. Bivalacqua noted that re-induction was permitted for patients with persistent high-grade Ta disease and/or CIS at the 3-month evaluation. Surveillance included cystoscopy and cytology every 3 months and CT or MR urography every 6 months. Importantly, treatment was administered in the clinic setting, with patients allowed to void at home during maintenance therapy.
The study included 55 patients enrolled across multiple sites in the United States, including both community and academic centers. The cohort was predominantly male (78.2%), White (92.7%), and older than 65 years (81.8%), with a median age of 75 years. Most patients had excellent performance status, with 87.3% having an ECOG performance status of 0.
At study entry, disease characteristics were well balanced between treatment arms, with 50.9% of patients presenting with CIS ± high-grade Ta/T1 disease and 49.1% with papillary-only high-grade Ta/T1 disease. The median number of prior BCG doses was 7, with 65.5% of patients classified as BCG-exposed and 34.5% meeting criteria for BCG-unresponsive disease.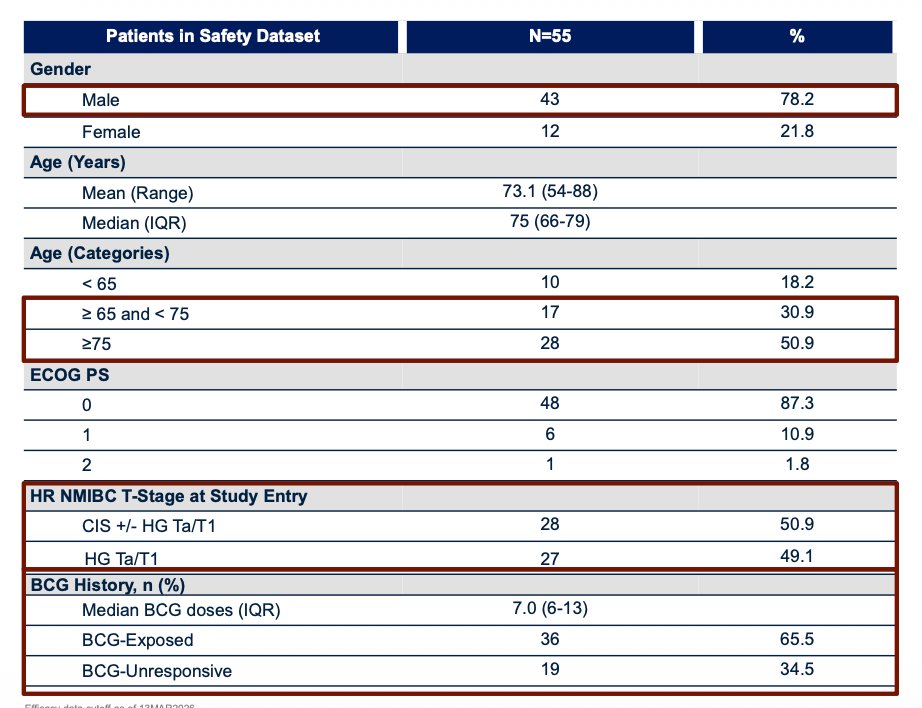
At a median follow-up of 6.6 months, the combination strategy demonstrated encouraging early disease control, with estimated high-grade event-free survival rates of 96.0% at 3 months and 89.5% at 6 months in the intention-to-treat population. Dr. Bivalacqua noted that outcomes were consistent between the concurrent and sequential treatment arms, with no significant differences observed between groups.
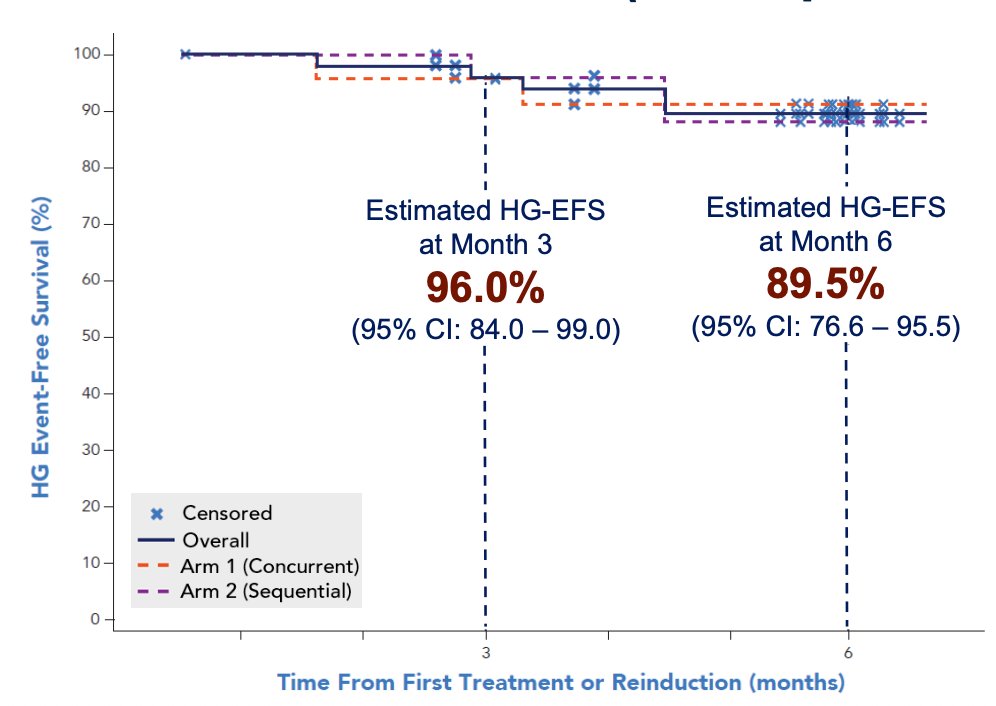
Importantly, responses appeared similar across both BCG-unresponsive and BCG-exposed subgroups. No treatment-related progression to MIBC or metastatic urothelial carcinoma was observed, although 2 patients experienced NMIBC stage reclassification during follow-up.
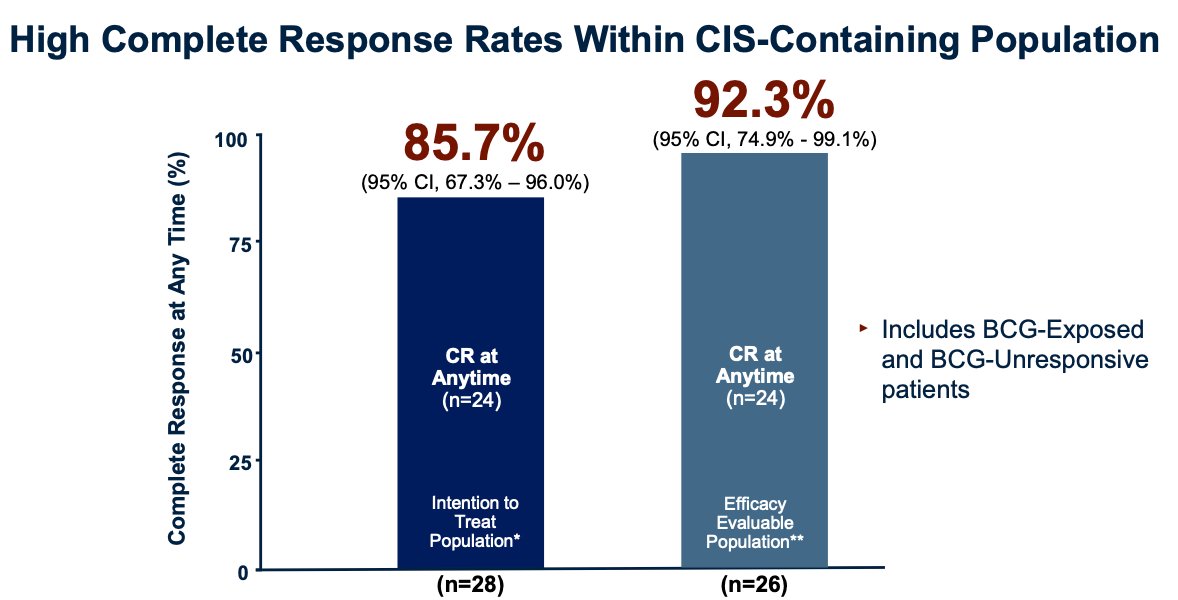
Among patients with CIS-containing disease, the combination strategy demonstrated high complete response rates. In the intention-to-treat population, 85.7% of patients achieved a complete response at any time, increasing to 92.3% among evaluable patients. Dr. Bivalacqua noted that these results included both BCG-exposed and BCG-unresponsive patients, further supporting the promising activity of cretostimogene plus gemcitabine in this high-risk population.
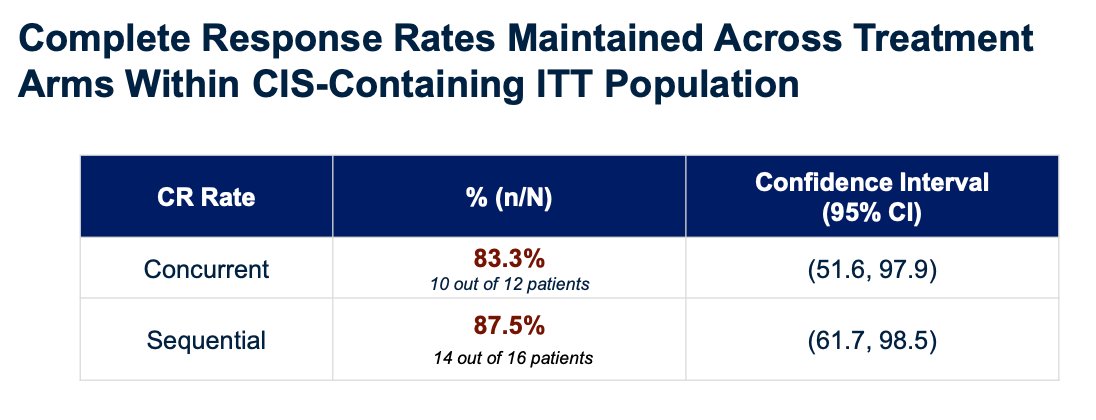
Complete response rates remained high across both treatment strategies within the CIS-containing intention-to-treat population. Complete response at any time was achieved in 83.3% of patients treated with concurrent therapy and 87.5% of those treated with sequential therapy, with overlapping confidence intervals between groups. Dr. Bivalacqua noted that these findings were directionally consistent with the high-grade event-free survival results observed in the overall study population, as shown below.
From a safety standpoint, the combination regimen demonstrated a favorable and well-tolerated profile, with no grade ≥3 treatment-related adverse events, serious adverse events, or treatment-related deaths reported. Overall, 65.5% of patients experienced at least one treatment-related adverse event, all of which were grade 1–2. The most common toxicities included bladder spasms, dysuria, pollakiuria, fatigue, urinary urgency, and hematuria.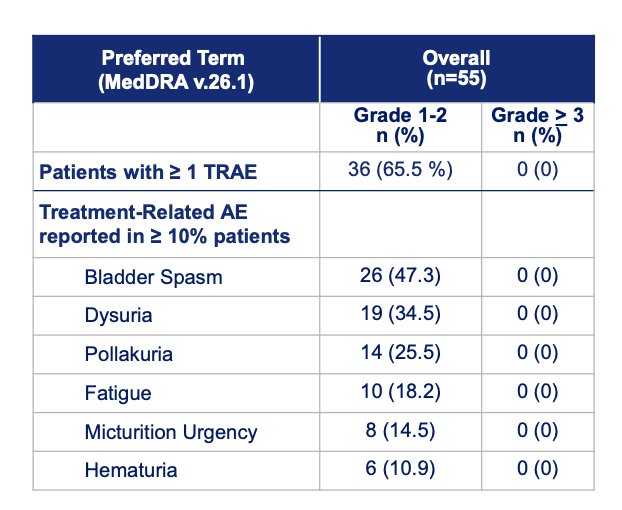
Importantly, 85.5% of patients completed all protocol-defined treatments. No patients discontinued treatment in the sequential arm due to treatment-related adverse events, while 4 patients in the concurrent arm withdrew because of persistent grade 1–2 localized urinary symptoms. Dr. Bivalacqua also noted that the overall proportion of adverse events was similar between treatment arms.
Dr. Bivalacqua concluded his presentation with the following key messages:
- The combination of cretostimogene and gemcitabine demonstrated encouraging efficacy and a favorable safety profile in patients with BCG-exposed and BCG-unresponsive NMIBC
- Comparable clinical activity was observed between the concurrent and sequential treatment strategies
- Sequential administration of intravesical cretostimogene followed by gemcitabine was well tolerated and supports the feasibility of intravesical-only combination treatment approaches
- Ongoing follow-up will further characterize the long-term durability and oncologic outcomes associated with this strategy
Presented by: Trinity Bivalacqua, MD, PhD, Director of Urologic Oncology, Co-Director of the Genitourinary Cancer Service Line, Abramson Cancer Center, Professor of Surgery, Hospital of the University of Pennsylvania, Philadelphia, PA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Related content: CORE-008 Cohort CX: Early Results of Cretostimogene plus Gemcitabine in BCG-Unresponsive and BCG-Exposed NMIBC - Trinity Bivalacqua
CORE-008 CX Early Efficacy and Tolerability Data - Aaron Berger
Reference:
- Li R, Shah PH, Stewart TF, Nam JK, Bivalacqua TJ, Lamm DL, Uchio EM, Geynisman DM, Jacob JM, Meeks JJ, Dickstein R, Pearce SM, Kang SH, Jung SI, Kamat AM, Burke JM, Keegan KA, Steinberg GD. Oncolytic adenoviral therapy plus pembrolizumab in BCG-unresponsive non-muscle-invasive bladder cancer: the phase 2 CORE-001 trial. Nat Med. 2024 Aug;30(8):2216-2223. doi: 10.1038/s41591-024-03025-3. Epub 2024 Jun 6. Erratum in: Nat Med. 2024 Aug;30(8):2372. doi: 10.1038/s41591-024-03137-w. Erratum in: Nat Med. 2024 Aug;30(8):2377. doi: 10.1038/s41591-024-03157-6. PMID: 38844794.
- Escobar D, Doshi C, Zahir M, Daneshmand S. Modern management of BCG-refractory non-muscle-invasive urothelial carcinoma of the urinary bladder. Urologie. 2026 Feb;65(2):162-170. doi: 10.1007/s00120-025-02625-2. Epub 2025 Jun 23. PMID: 40549001; PMCID: PMC12894138.