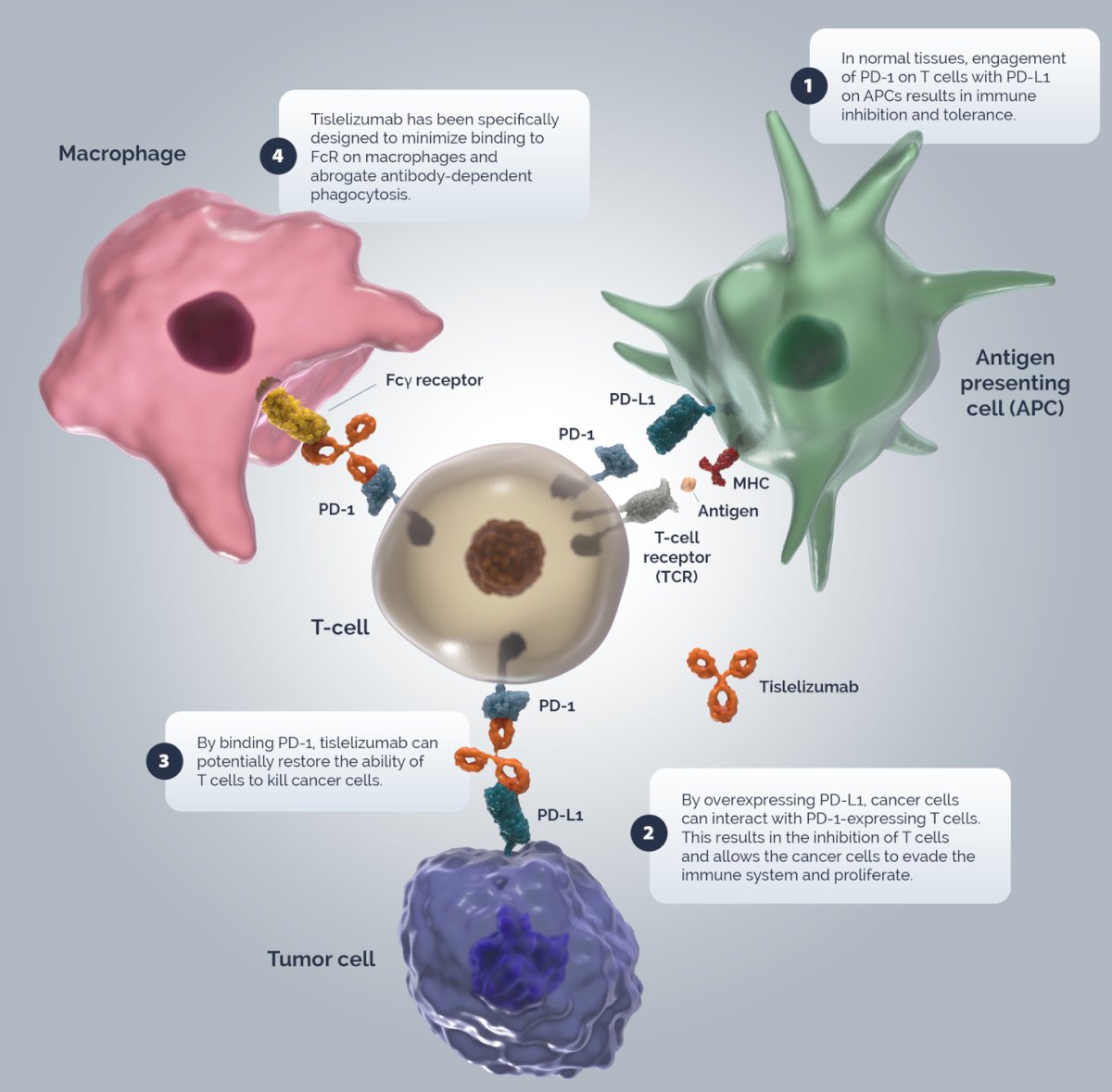
(UroToday.com) The 2025 AUA annual meeting featured an upper tract urothelial carcinoma session and a presentation by Dr. Jiwei Huang discussing results of a phase II study of tislelizumab as neoadjuvant treatment for cisplatin-ineligible high-risk upper tract urothelial carcinoma. Tislelizumab is a humanized IgG4 anti-PD-1 monoclonal antibody, with the following proposed mechanism of action:
This single-arm, phase II trial (NCT04672330) recruited 20 patients with high-risk upper tract urothelial carcinoma for enrollment. Eligibility criteria included high-risk upper tract urothelial carcinoma (defined as high-grade upper tract urothelial carcinoma confirmed by endoscopic biopsy or urinary cytology, radiographic evidence of invasion [cT2-T4N0-2M0], and/or hydronephrosis), an ECOG performance status of 0-2, no prior systemic therapy, and cisplatin ineligibility. Patients were given tislelizumab 200 mg IV every 3 weeks for at most 4 cycles, followed by surgery. Contrast-enhanced MRI was performed before the third dose and again before surgery. The primary endpoint was pathological complete response rate (ypT0N0), and secondary endpoints included pathological response rate (≤ypT1N0), objective response rate, disease-free survival, safety profile, and perioperative complications. Multiplex immunofluorescence was used to assess immune cell populations in the tumor microenvironment.
Among the 20 patients, 13 underwent radical nephroureterectomy, 1 received endoscopic ablation, and 3 had segmental ureteral resection. Three patients declined surgery due to disease progression or adverse events. The pathological complete response rate was 20%, with 45% of patients restaged to ≤pT1. The following spider plot of tumor response shows the percent change of maximal tumor diameter:
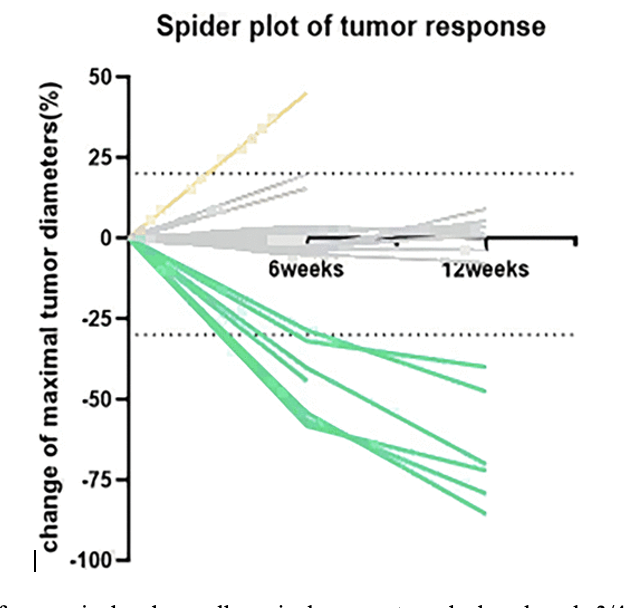
Median disease-free survival and overall survival were not reached, and grade 3/4 treatment-related adverse events occurred in 15% of patients. MRI analysis revealed higher ADC entropy in patients with partial response. Exploratory analysis showed increased PD-L1 + CD68+ macrophages and PD-1 + CD8+ T cells in the tumor stroma of partial and complete responders.
Dr. Huang concluded this presentation discussing results of a phase II study of tislelizumab as neoadjuvant treatment for cisplatin-ineligible high-risk upper tract urothelial carcinoma with the following take-home points:
- Neoadjuvant tislelizumab showed promising efficacy and manageable toxicity in high-risk, cisplatin-ineligible upper tract urothelial carcinoma patients
- Increased ADC entropy on MRI and the presence of PD-L1 + CD68+ macrophages in the tumor stroma may serve as potential predictors of response to neoadjuvant tislelizumab
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.