(UroToday.com) Austin Drysch, from Northwestern University Feinberg School of Medicine, presented an important study evaluating how prior holmium laser enucleation of the prostate (HoLEP) affects the performance of prostate multiparametric MRI (mpMRI) and the associated Prostate Imaging Reporting & Data System (PI-RADS) score for detecting clinically significant prostate cancer (csPCa).
Given that HoLEP significantly alters prostate anatomy and is recommended by AUA guidelines for treating bladder outlet obstruction across all prostate sizes, understanding its impact on prostate cancer detection is essential.
The study queried the Northwestern Electronic Data Warehouse to identify patients who underwent mpMRI followed by prostate biopsy. Data collected included demographics, mpMRI findings (specifically PI-RADS scores), and biopsy pathology (Gleason grade [GG]). Patients were stratified based on whether they had undergone prior HoLEP, and the primary outcome was detection of csPCa, defined as GG ≥2, on biopsy.
![The study queried the Northwestern Electronic Data Warehouse to identify patients who underwent mpMRI followed by prostate biopsy. Data collected included demographics, mpMRI findings (specifically PI-RADS scores), and biopsy pathology (Gleason grade [GG]). Patients were stratified based on whether they had undergone prior HoLEP, and the primary outcome was detection of csPCa, defined as GG ≥2, on biopsy.](/images/com-doc-importer/206-aua-2025/aua-2025-impact-of-prior-holmium-laser-enucleation-of-the-prostate-holep-on-the-accuracy-of-pi-rads-for-assessing-clinically-significant-prostate-cancer/image-0.jpg)
Logistic regression analysis was performed to evaluate the impact of prior HoLEP on csPCa detection, adjusting for clinical variables such as age, race, family history of prostate cancer, PSA density, and PI-RADS score.
Out of 7,790 patients who met inclusion criteria, 43 patients (0.6%) had a history of HoLEP. Among these, HoLEP pathology revealed GG1 disease in 46.5% of patients, GG2 in 48.8%, and GG3 in 4.7%. The average time from HoLEP to subsequent mpMRI was 7.4 months.
As expected, the HoLEP group had significantly lower prostate volume (23.0 cm³ vs. 48.0 cm³; p<0.001) and PSA density (0.04 vs. 0.12; p<0.001) compared to controls.
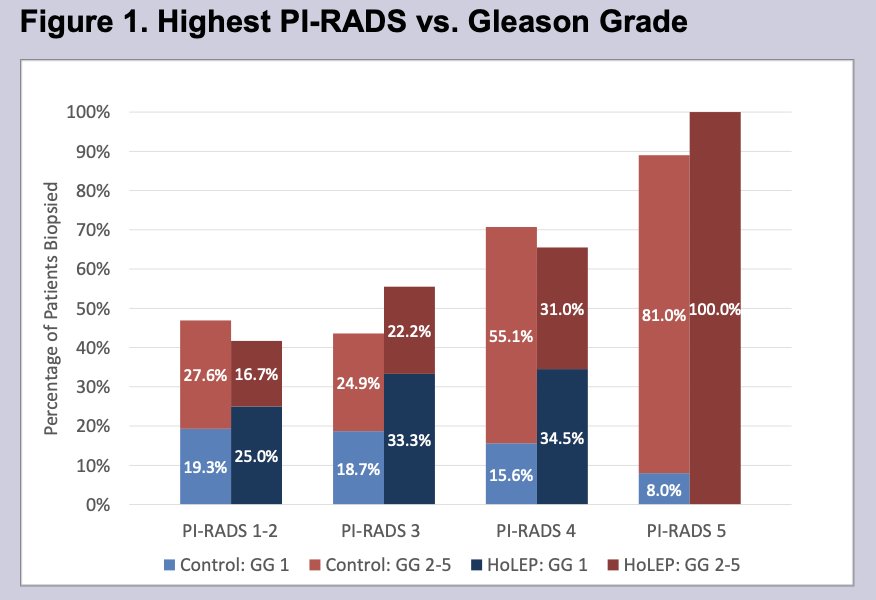
- When stratified by PI-RADS score, rates of csPCa detection were comparable between HoLEP and non-HoLEP patients (Figure 1).
- However, overall csPCa detection was significantly lower among patients with prior HoLEP (25.6% vs. 50.7%; p=0.001) (Table 1).
On univariable logistic regression, prior HoLEP was associated with significantly lower odds of csPCa detection (OR=0.33; 95% CI: 0.16–0.64). However, on multivariable analysis adjusting for other clinical factors, the association was no longer statistically significant (OR=0.77; 95% CI: 0.33–1.65).
The presenter noted that though csPCa detection was significantly lower for the cohort of patients with prior HoLEP, this was likely a result of PCa screening prior to any type of surgical intervention, namely, HoLEP.
Despite the anatomical changes caused by HoLEP, PI-RADS scoring on mpMRI remains an effective tool for assessing the risk of clinically significant prostate cancer. Although overall csPCa detection rates were lower in the HoLEP cohort, this difference may reflect a lower proportion of high-risk (PI-RADS 5) lesions within the group rather than reduced accuracy of the imaging modality itself.
This study supports the continued use of mpMRI and PI-RADS scoring even in patients with a history of HoLEP, while highlighting important considerations in interpreting cancer risk in this unique patient population.
Following his insightful presentation, Dr. Eric Kim of the University of Nevada suggested “it would be great in the 43 patients if you guys can somehow figure out the indication for follow up” which Mr. Drysch was well prepared to answer and responded, “In general it is detection of prostate cancer on the HoLEP specimen… 25 patients had GG1, 25 patients had GG2, and 2 had GG3.”
Presented by: Austin Drysch, MS3, Northwestern University Feinberg School of Medicine, Chicago, IL
Written by: Mark Sarwat Hana, Assistant Research Specialist, Department of Urology, University of California, Irvine, at the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.