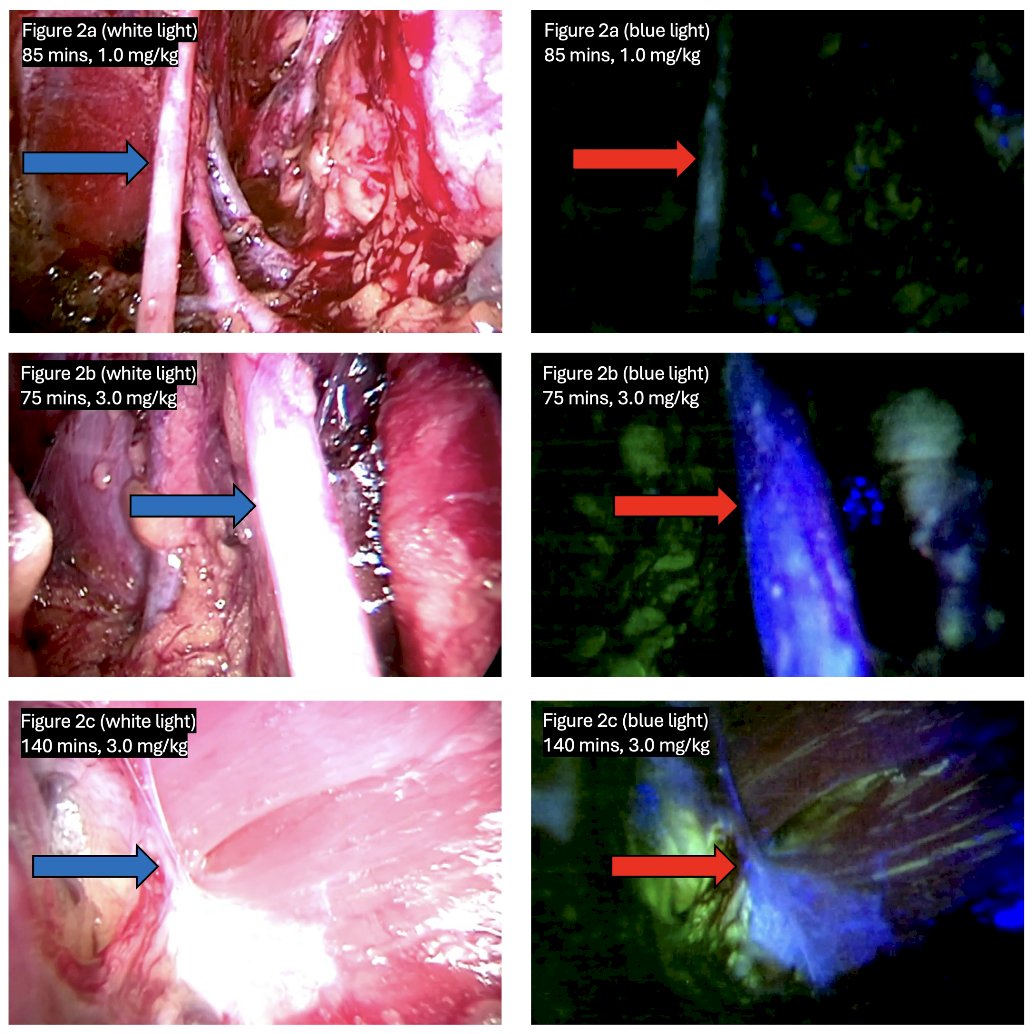
(UroToday.com) The 2025 AUA annual meeting featured a prostate cancer session and a presentation by Dr. Samuel Gold discussing a phase I trial of rizedisben in robotic radical prostatectomy. Rizedisben is a novel myelin-binding fluorophore that fluoresces in the blue light (370-425 nm) spectrum. Iatrogenic nerve injury is a leading cause of morbidity associated with many surgical procedures, thus, fluorescence-guided surgery utilizes enhanced visualization of critical structures to reduce iatrogenic injury or improve critical excisions. The objective of this study, presented at the AUA annual meeting, was to determine the safety of intravenous administration of rizedisben and to determine optimal dose level for sustained fluorescence of nerve structures during intraoperative visualization.
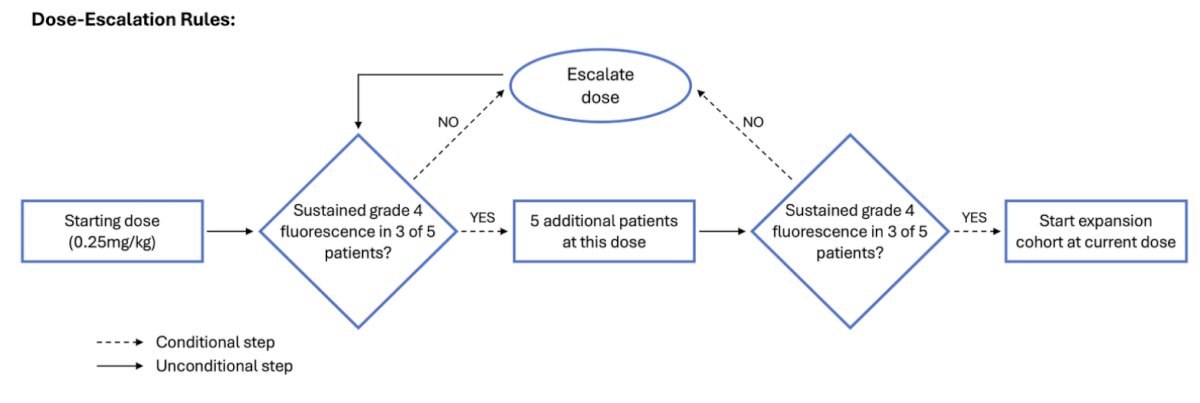
This was a single-arm, open-label phase I study of intravenous administration of rizedisben use in robotic assisted radical prostatectomy, injected at the time of robot docking. Dose escalation proceeded until optimal dose was achieved, at which time, assessment of neurovascular bundles was included. The effective dose was defined as sustained fluorescence in >=3 of 5 patients in 2 consecutive cohorts, provided <20% of patients experienced Clavien-Dindo grade >=2 toxicities. Fluorescence assessments of the obturator nerve were performed via blue light camera, and were measured subjectively via a Likert scale (1-5 points) intraoperatively by the surgical team and objectively via post hoc ImageJ analysis of operative images at the corresponding time points. Sustained fluorescence was defined as a subjective score >=4 points (moderate or better fluorescence) for >=90 minutes:
At each dose, if >=3 of 5 patients achieved sustained fluorescence, a second 5-patient cohort was added at that dose. Dose-response was estimated using general estimating equations, with both a linear and quadratic term for time. The dose escalation protocol is as follows:
From January 2023 to October 2024, 38 patients were enrolled and completed the protocol:
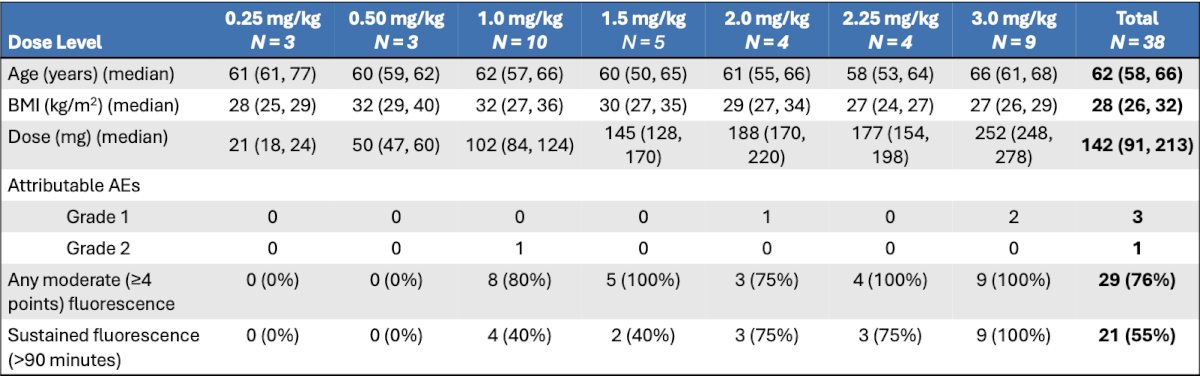
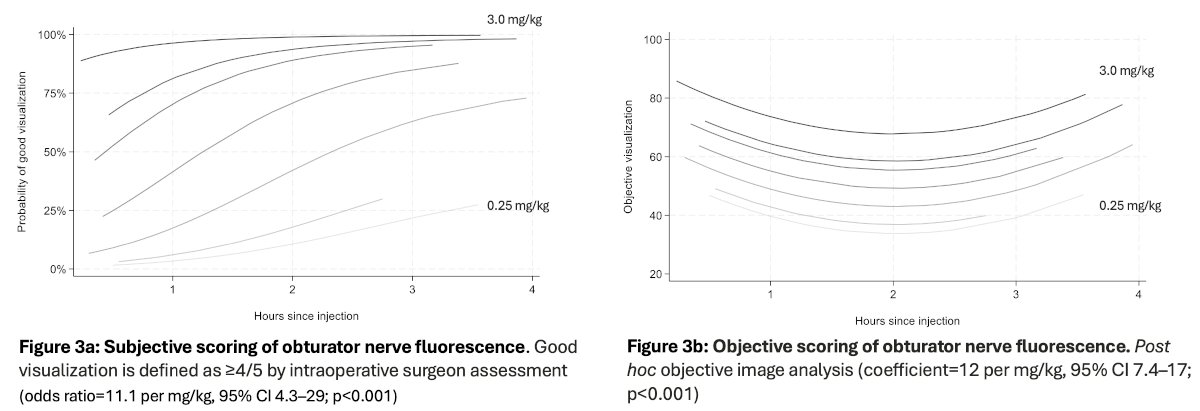
Dosing was escalated from 0.25 to 3.0 mg/kg, and sustained fluorescence of the obturator nerve was achieved in 41/42 observations at the clinically effective dose of 3.0 mg/kg (at 14 to 210 minutes post-injection). Significant increases in fluorescence were seen with increasing dose levels both subjectively and objectively:
Neurovascular bundles demonstrated minimal fluorescence (3 points) in 5 patients (56%) and moderate fluorescence (4 points) in 3 patients (33%) at 3.0 mg/kg. One adverse event, grade 1 photophobia, was deemed “definitely” related to rizedisben, and one grade 2 rash was seen in a patient with significant dermatologic history, was deemed “possibly” related to rizedisben. There were no neurologic changes observed in any patients.
Dr. Gold concluded his presentation discussing a phase I trial of rizedisben in robotic radical prostatectomy with the following take home messages:
- In a phase I trial, the optimal dose of Rizedisben was achieved at 3.0 mg/kg with minimal toxicity and sustained fluorescence of the obturator nerve
- Neurovascular bundles also demonstrated fluorescent signal, with future work to define effects on operative technique and outcomes
- Phase II trials in open and laparoscopic surgeries are in progress
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025