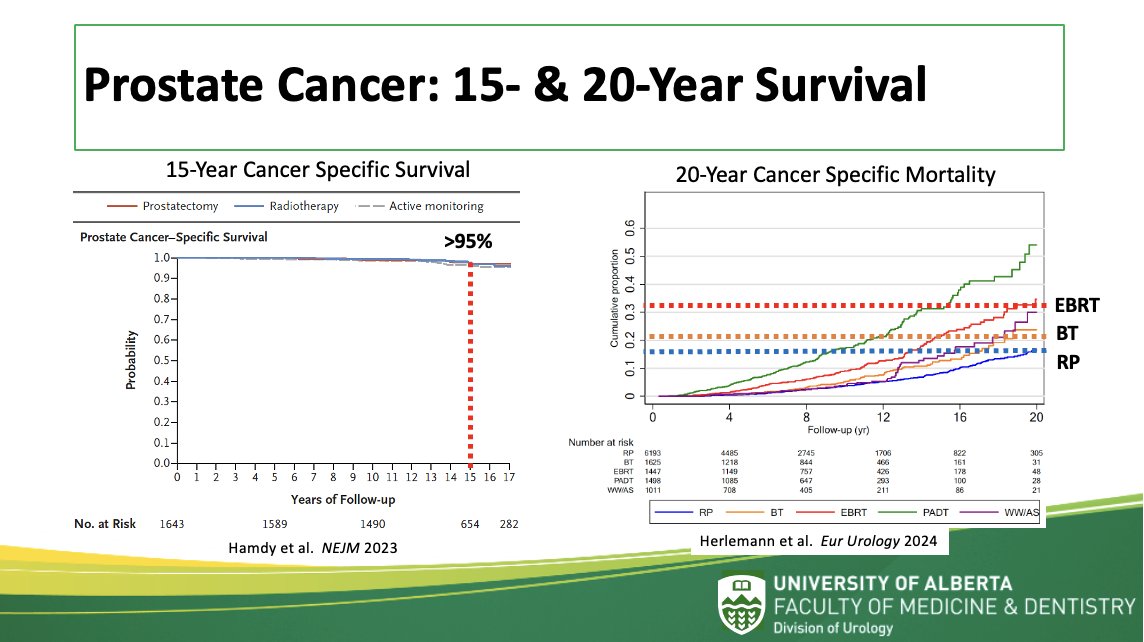
(UroToday.com) Dr. Keith Rourke from the University of Alberta presented on the topic of radiation-induced complications after prostate cancer (PCa) treatment. Dr. Rourke began by highlighting how it has become clear that the long term cancer specific survival for localized PCa is robust. The ProtecT trial demonstrated a 15-year cancer specific survival of over 95% regardless of treatment modality. The 20-year cancer-specific survival is around 80% for patients undergoing radical prostatectomy or brachytherapy and just under 70% for external beam radiation therapy (EBRT).
Dr. Rourke goes on to ask, “What are the 15- and 20-year harms of prostate cancer treatment?”
The rates of survival have created one of the largest groups of cancer survivors in Western society, with most patients surviving 15 years and beyond. Dr. Rourke quotes that with this in mind, “the choice of therapy involved weighing trade-offs between benefits and harms associated with treatments for localized prostate cancer”.
Guidelines such as the AUA/ASTRO guidelines make it clear that patients should be aware that all PCa treatments carry risk. The complications specifically mentioned are the “Big Three” of urinary incontinence, sexual dysfunction, and bowel dysfunction.
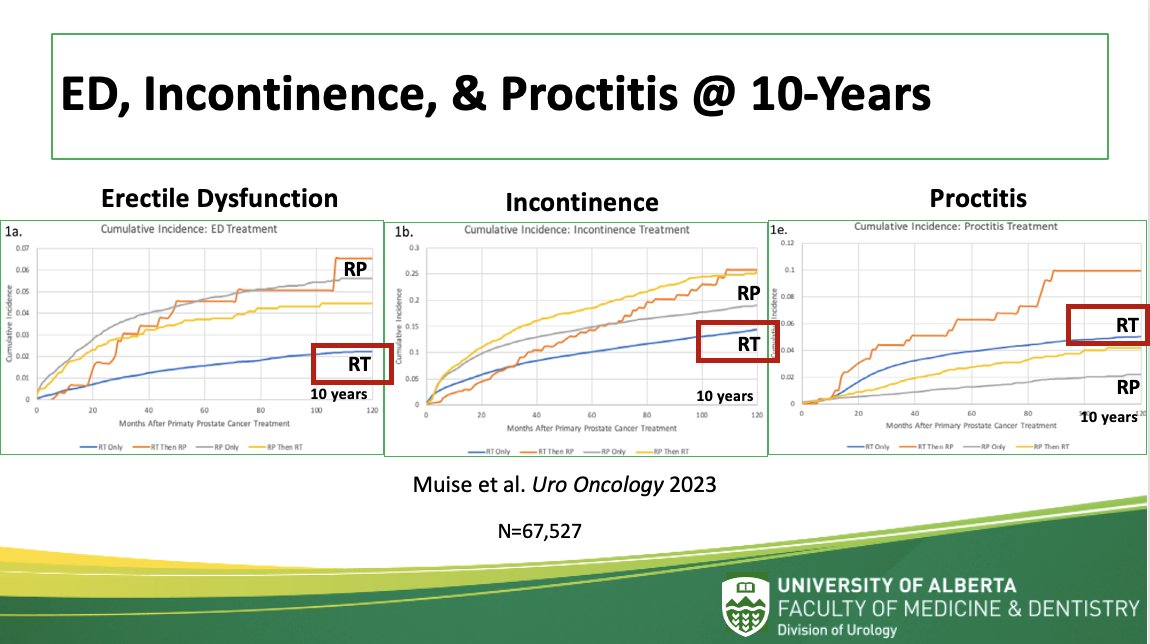
Dr. Rourke then goes in to examine these individually. He first mentions that a retrospective analysis from the SEER database of over 67,000 patients determined treatment rates for erectile dysfunction (ED), incontinence, and proctitis at 10 years post-treatment. Patients undergoing radiotherapy (RT) had lower rates of both ED and incontinence compared to radical prostatectomy (RP) alone. However, they did have higher rates of proctitis. Combined therapy fared worse in every aspect. Overall, this would suggest lower morbidity of RT at least at 10 years when examining these three outcomes alone.
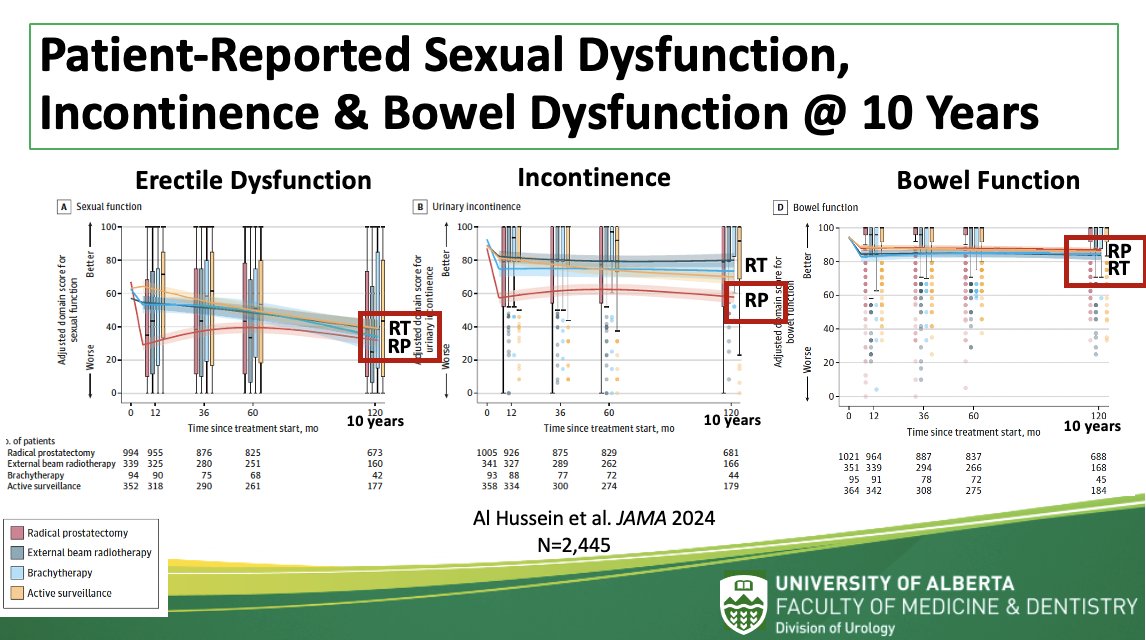
From a patient perspective, the CEASAR study examined similar adverse events using patient-reported outcomes. Among patients treated for localized PCa, radical prostatectomy was associated with worse urinary incontinence at 10 years, but similar sexual and bowel function when compared to patients undergoing radiation. On balance, based on these 3 measures, patients undergoing radiation would seem to have better functional outcomes at 10 years.
Dr. Rourke poses the questions, “However, is 10-years follow up considered long-term when considering the high rates of cancer-free survival? Also, do the BIG THREE functional outcomes fully encompass the entire spectrum of complications?”
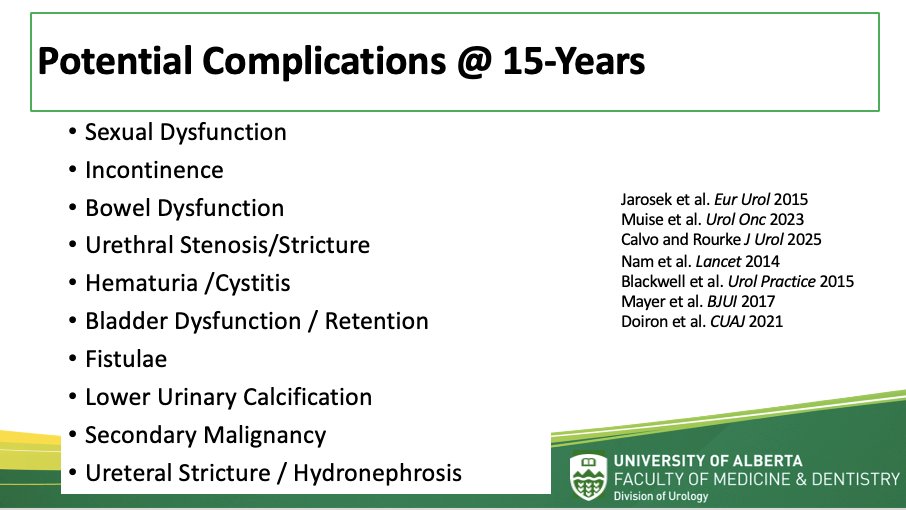
“Likely not”, he answers. The full spectrum of complications also includes urethral stenosis, hematuria/cystitis, bladder dysfunction, fistulae, lower urinary calcifications, and secondary malignancy. The upper tract is also not exempt from adverse events.
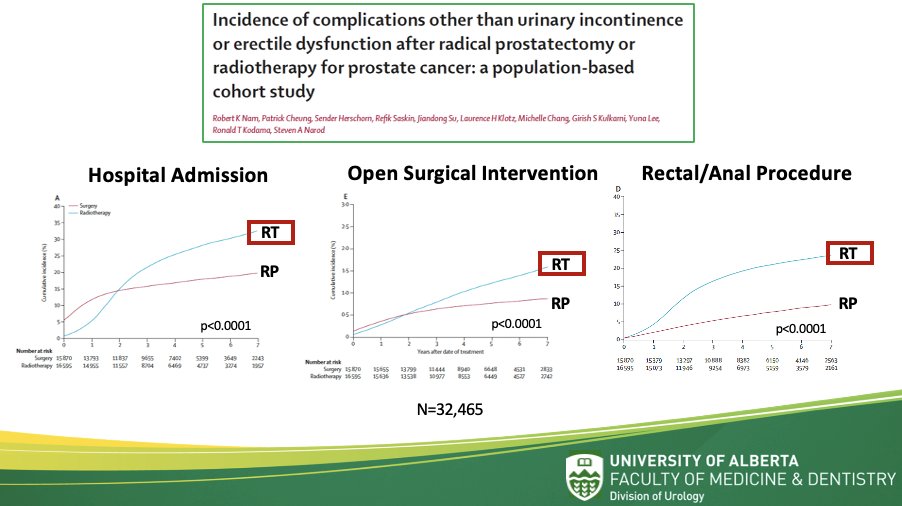
Dr. Rourke continues to highlight that the long-term complications of prostate cancer treatments extend well beyond the "Big Three." As patients progress past the 10-year mark, new and often more severe complications begin to emerge. These complications are multifocal, meaning that patients frequently experience multiple adverse outcomes concurrently, which complicates their overall care and treatment. A key finding in the literature is that complications associated with radiation therapy can appear insidiously and rarely in isolation, often necessitating long-term, multifaceted management strategies.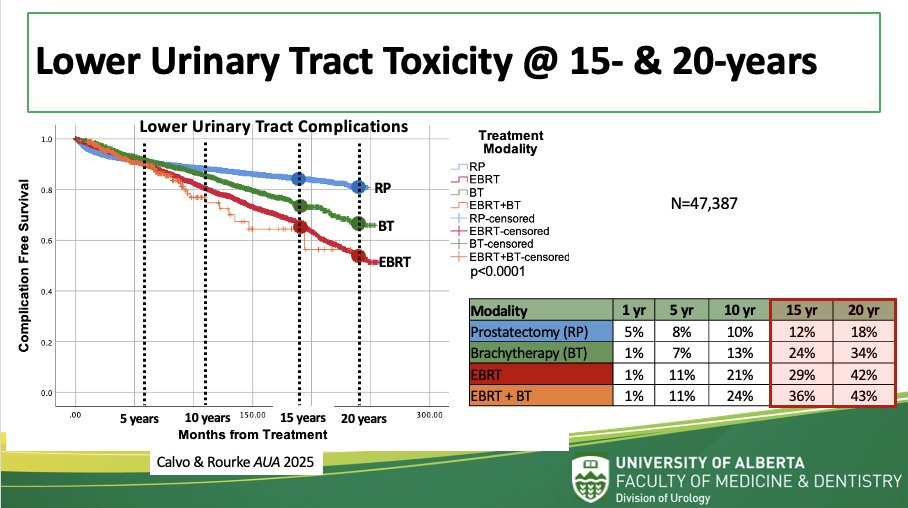
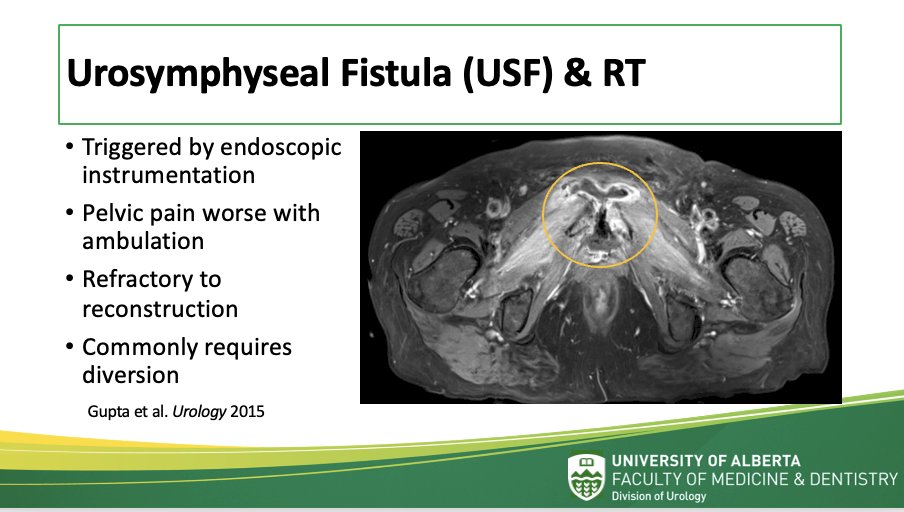
One of the most concerning complications after radiation therapy is the development of urethral stricture, which is particularly problematic for patients undergoing brachytherapy or EBRT. Radiation can lead to fibrosis, calcification, and in some cases, fistula formation. The underlying mechanisms include microvascular damage, obliterative endarteritis, and ischemia caused by radiation-induced cellular injury. Dr. Rourke references several studies, including Merrick et al. (2006) and Hindson et al. (2012), that highlight the increased risk of urethral stenosis post-radiotherapy.
Treatment options for urethral stenosis remain limited and often temporary. Dilations and direct visual internal urethrotomy (DVIU) are frequently used, though they are only successful in less than 5% of cases. Self-dilation, while sometimes employed, can be challenging for patients. Urethral reconstruction through urethroplasty is a more durable option, but these procedures are labor-intensive and not without their own set of risks. Dr. Rourke emphasizes that a large proportion of patients will require multiple interventions over the course of their lifetimes. The complexities of these treatments underscore the significant burden that radiation-induced urethral complications can impose on both patients and healthcare providers.
As patients progress to 15 or 20 years post-treatment, the incidence of bladder dysfunction rises. These complications can include hematuria, cystitis, and in severe cases, bladder retention or urinary diversion. Dr. Rourke stresses that radiation therapy is particularly harmful to the bladder, with long-term consequences that significantly affect patients' quality of life. In some instances, these complications necessitate invasive procedures such as bladder reconstruction or even cystectomy.
Additionally, secondary malignancies are a well-established risk following radiation therapy. The long latency period before the development of secondary cancers, such as colorectal, bladder, and rectal cancers, makes them particularly difficult to manage. Dr. Rourke cites studies that show an increased risk of secondary malignancies in patients treated with radiation, which becomes more apparent with time. This risk, while not negligible, remains one of the most significant challenges in radiation oncology, as it directly impacts patient survival in the long term.
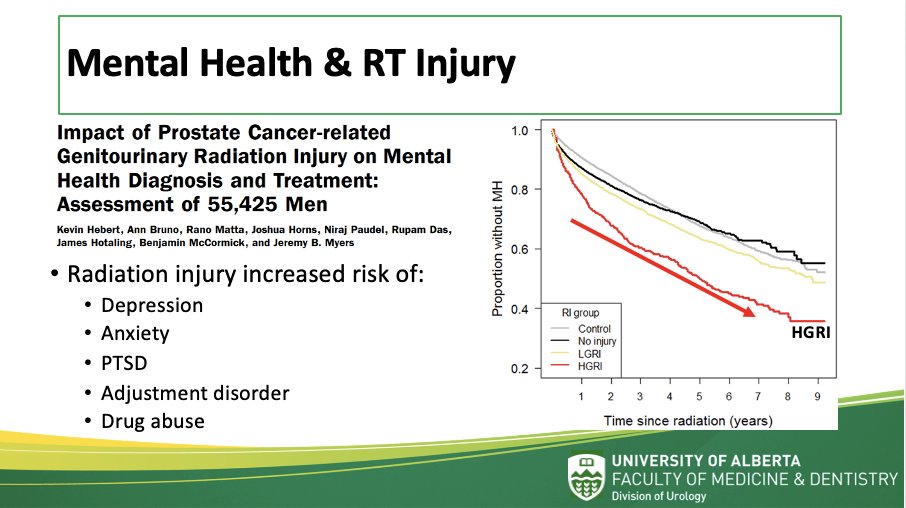
Dr. Rourke draws attention to another frequently underappreciated consequence of radiation therapy: its impact on patients' mental health. As patients experience complications such as incontinence, sexual dysfunction, and bowel issues, the psychological burden can be profound. Radiation-induced injuries are strongly associated with depression, anxiety, PTSD, and other mood disorders. Patients often feel unprepared for these challenges, which can lead to a delay in seeking help or treatment. A recent study from Utah examined the risk of mental health diagnoses and treatment in 55,425 men who underwent radiation treatment for prostate cancer. Radiation injury was independently associated with an increased risk of mental health diagnoses and treatments when compared to men without radiation injury, including depression, anxiety, PTSD, adjustment disorder, and drug abuse.

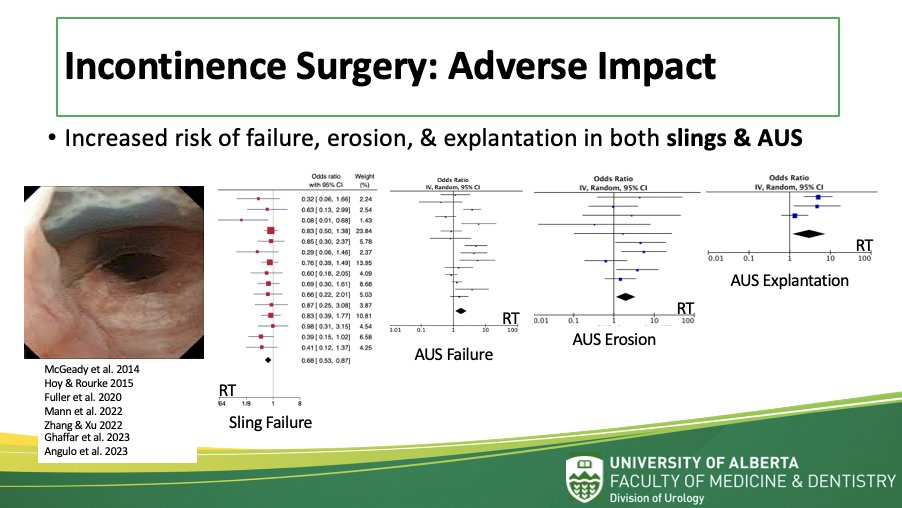
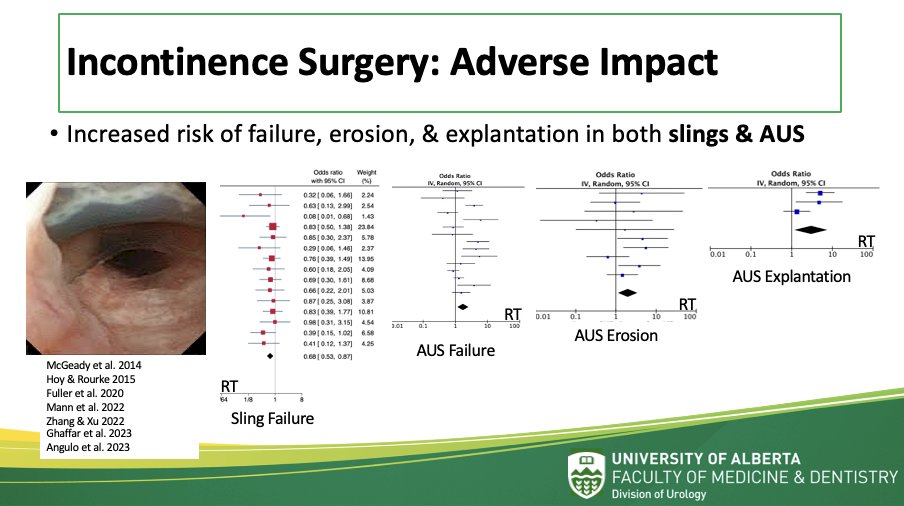
Another critical point Dr. Rourke emphasizes is the heightened risk of failure associated with secondary procedures, particularly incontinence surgeries. For patients who have undergone radiation therapy, the risk of failure, erosion, or explantation in both slings and artificial urinary sphincter (AUS) devices is considerably higher. This trend has been documented in multiple studies, and the added challenge of managing radiation-induced complications complicates the success rates of these devices. Dr. Rourke suggests that urologists must be particularly cautious when performing these secondary procedures, as radiation therapy can significantly alter the healing and integration processes of these implants.
Dr. Rourke concludes his presentation by discussing the long-term complications that can affect the upper urinary tract, which is often overlooked in the management of prostate cancer. These complications include ureteral stricture, hydronephrosis, and upper tract infections, which can develop as a result of the radiotherapy used to treat prostate cancer. The incidence of these issues increases over time, and as with lower urinary tract complications, management often requires a combination of surgical interventions and ongoing patient monitoring.
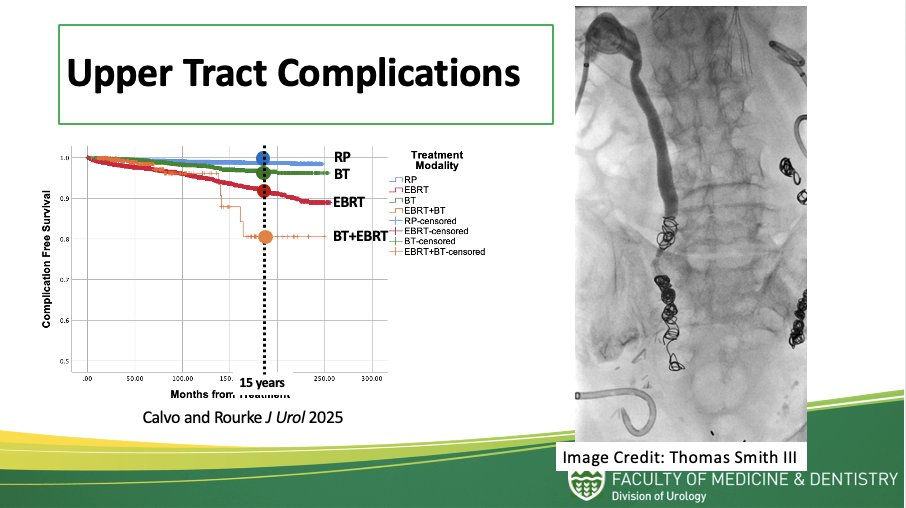
The cumulative effect of these upper tract complications can significantly diminish a patient’s quality of life, especially when combined with the other issues stemming from lower urinary tract dysfunction and sexual dysfunction. Dr. Rourke stresses that a holistic approach to care, incorporating both physical and mental health support, is crucial to managing these complex cases effectively.
Dr. Rourke’s presentation underscores the critical need for comprehensive, long-term monitoring of prostate cancer survivors, particularly those treated with radiation therapy. While the benefits of treatment are undeniable in terms of cancer survival, the spectrum of complications—many of which emerge only after a decade or more—requires urologists and healthcare providers to maintain a vigilant, proactive approach to care. By addressing both the physical and psychological challenges posed by radiation therapy, clinicians can help improve outcomes and quality of life for these patients, ensuring they receive the support they need long after their cancer treatment has ended.
In the long-term, men undergoing prostate cancer treatment are at risk for developing complications regardless of treatment modality. Cumulative risk increases up to 20 years after treatment and may be higher in patients undergoing RT, especially EBRT and combined modalities. When RT complications occur, they are usually delayed in onset, seldom isolated, and when combined with poor patient awareness, create the perfect storm of a uniquely challenging clinical condition.
This lecture serves as a call to action for urologists to integrate comprehensive care models that account for the broad range of complications arising from prostate cancer treatment, promoting better long-term outcomes and patient satisfaction.
Presented by: Keith Rourke, MD, Professor, Division of Urology, Department of Surgery, University of Alberta, Edmonton, Alberta, Canada
Written by: Eman N. Chaudhri, MD, Department of Urology, University of California Irvine, @EmanChaudhri on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025