(UroToday.com) The 2025 AUA annual meeting featured an advanced prostate cancer session and a presentation by Dr. Neal Shore discussing ultra-low PSA response (<0.02 ng/mL) with darolutamide plus ADT in ARANOTE. In the phase 3 ARANOTE trial, darolutamide + ADT significantly reduced risk of radiological progression or death by 46% (HR 0.54, 95% CI 0.41–0.71, p < 0.0001) versus placebo + ADT in patients with mHSPC.1 Time to PSA progression was also longer with darolutamide versus placebo (HR 0.31, 95% CI 0.23–0.41), and more darolutamide patients achieved PSA <0.2 ng/mL (62.6%) versus placebo patients (18.5%). Importantly, achievement of PSA < 0.2 ng/mL with darolutamide correlated with clinical benefit. The incidence of treatment-emergent adverse events was low and similar between groups, with fewer patients discontinuing darolutamide (6.1%) versus placebo (9.0%) due to treatment emergent adverse events. At the AUA 2025 annual meeting, Dr. Shore and colleagues reported post hoc analyses of ultra-low PSA responses (<0.02 ng/mL) and their correlation with outcomes in ARANOTE.
Rates of PSA <0.02 ng/mL were evaluated at 24, 36, and 48 weeks and at any time. Ultra-low PSA responses were also assessed by baseline PSA group, defined as < first quartile (Q1: <4.1 ng/mL), between Q1 and median (Q2: 4.1 to <21.3 ng/mL), and => median (Q3 and Q4: =>21.3 ng/mL). Relevant clinical outcomes (radiological progression-free survival, time to mCRPC, and time to PSA progression) were correlated with PSA responses (PSA <0.02 ng/mL, PSA =>0.02 to <0.2 ng/mL, and PSA =>0.2 ng/mL) in darolutamide patients. Time to PSA progression was defined as the time from randomization to first PSA progression (>=25% increased above the nadir value, confirmed by a second value >=3 weeks later, and an increase in absolute PSA >=2 ng/mL above nadir >=12 weeks from baseline). A 36-week landmark analysis evaluated the risk of survival bias using an unstratified Cox regression model.
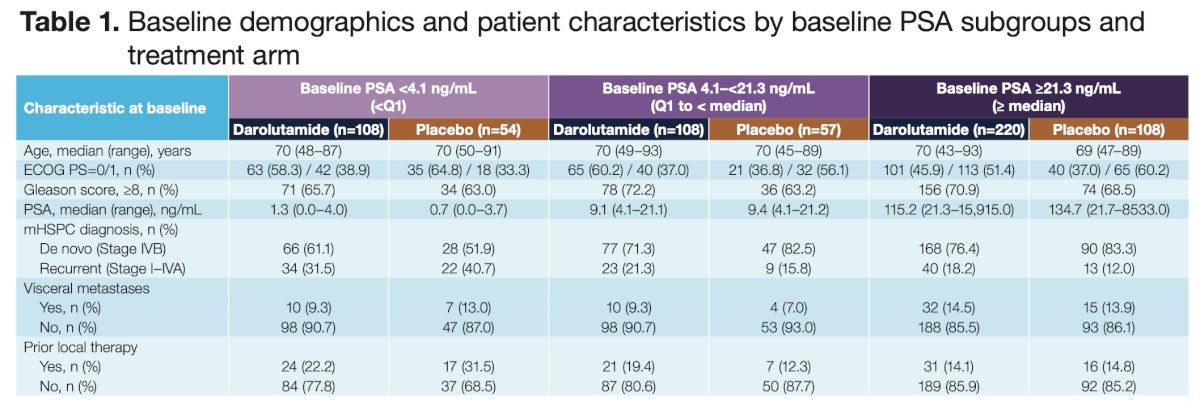
Of 669 randomized patients, 434 of 446 darolutamide and 218 of 223 placebo patients had a baseline PSA =>0.02 ng/mL. Median baseline PSA was 21.4 and 21.2 ng/mL in the darolutamide and placebo groups, respectively. At baseline, disease characteristics of patients by baseline PSA subgroups were generally similar, except fewer patients with PSA <4.1 ng/mL had de novo disease compared with groups with PSA >=4.1 ng/mL:
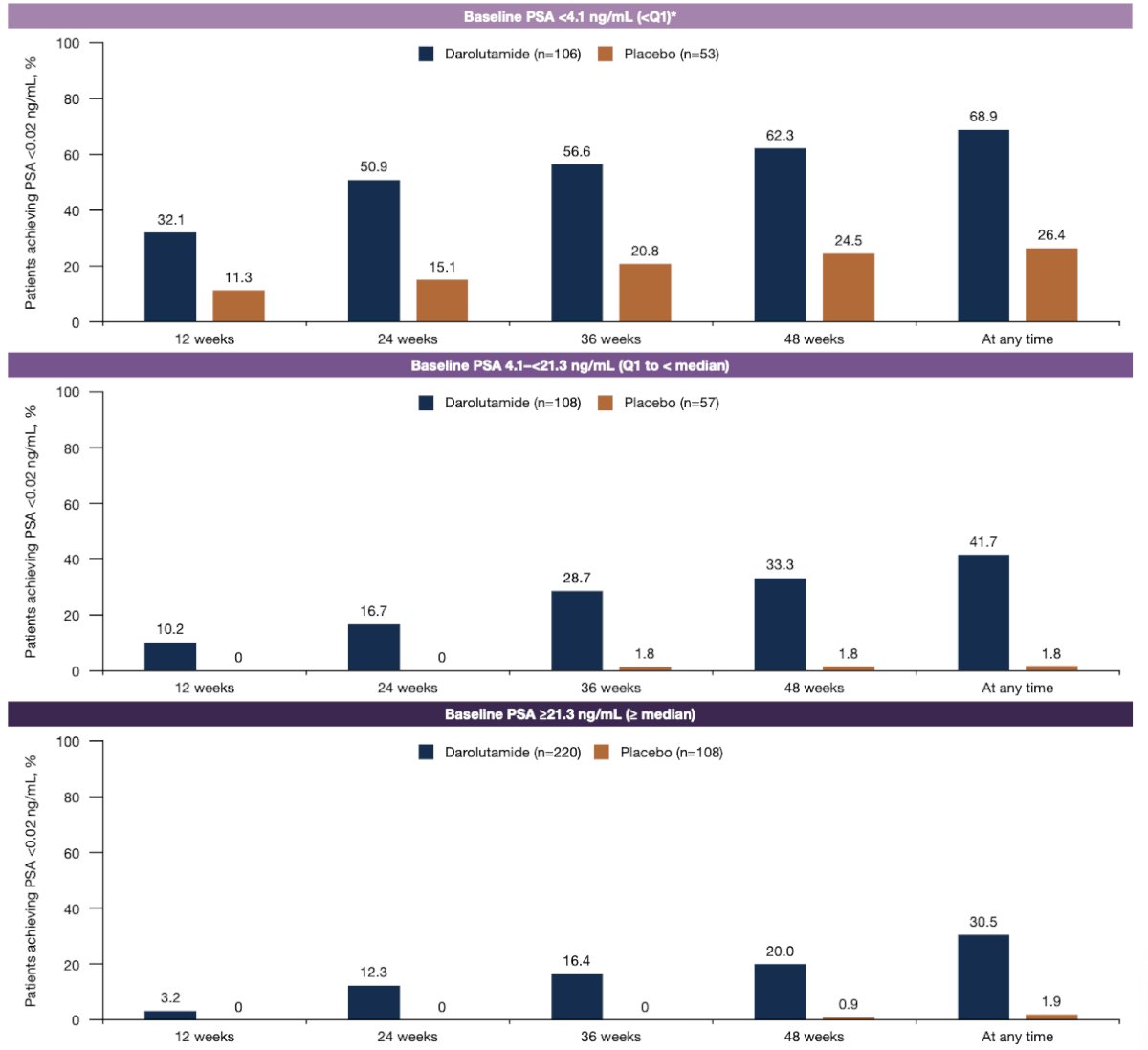
Darolutamide + ADT resulted in higher rates of ultra-low PSA responses versus ADT alone at all time points, and ultra-low PSA response rates increased with time, regardless of baseline PSA level. There were <2% of patients with baseline PSA >=4.1 ng/mL and treated with ADT alone who reached PSA <0.02 ng/mL at any time. There as 30.5% of patients treated with darolutamide + ADT and baseline PSA >21.3 ng/mL that reached PSA levels <0.02 ng/mL at any time:
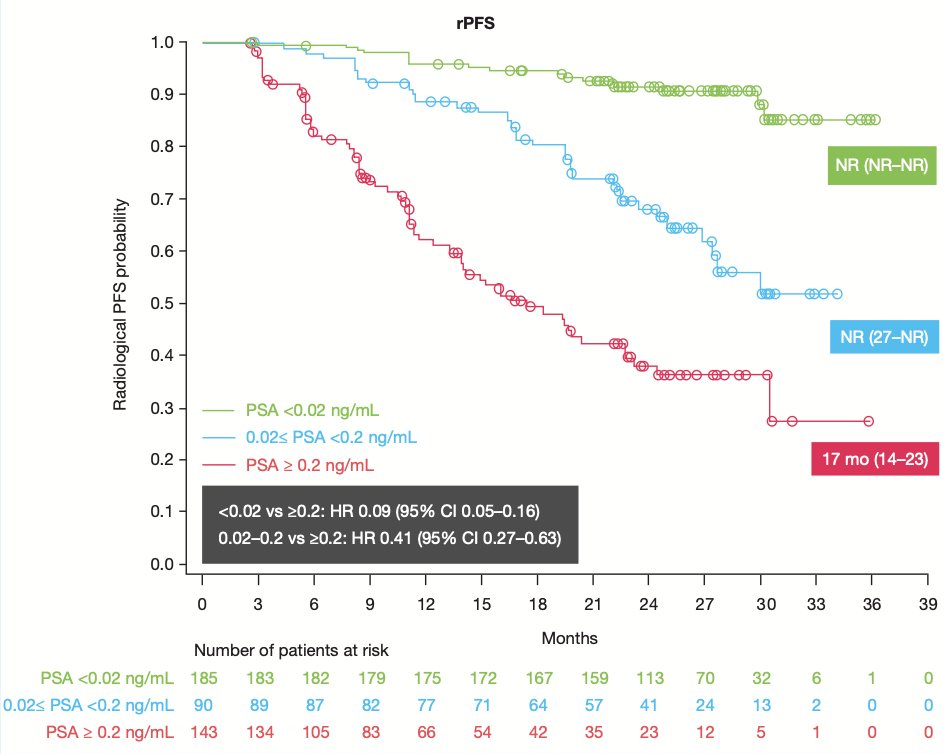
Patients treated with darolutamide who reached ultra-low PSA at any time had lower risk of radiological progression or death versus those with PSA >=0.2 ng/mL, with a risk reduction of 91%, as did patients who reached PSA between 0.02 and 0.2 ng/mL versus those with PSA >=0.2 ng/mL, with a risk reduction of 59%:
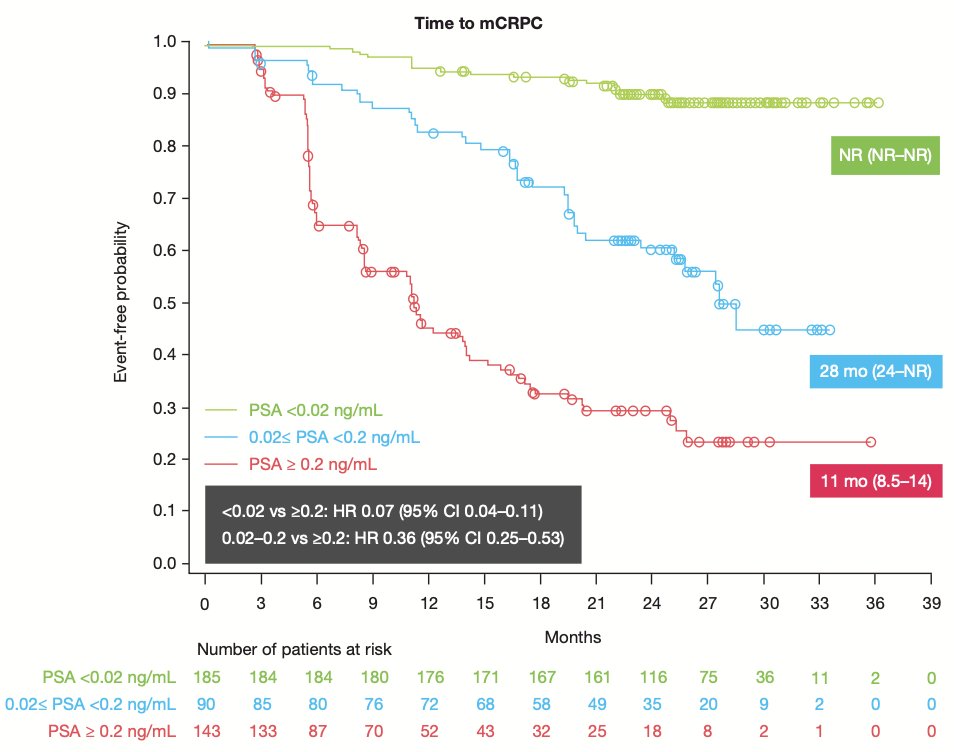
Patients treated with darolutamide who reached ultra-low PSA had a longer time to mCRPC versus those with PSA >=0.2 ng/mL, with a risk reduction of 93%, as did patients who reached PSA between 0.02 and 0.2 ng/mL versus those with PSA >=0.2 ng/mL, with a risk reduction of 64%:
Patients treated with darolutamide who reached an ultra-low PSA <0.02 ng/mL also had a longer time to PSA progression versus those with PSA >=0.2 ng/mL, with a risk reduction of 98%, as did patients who reached PSA between 0.02 and 0.2 ng/mL versus those with PSA >= 0.2 ng/mL, with a risk reduction of 79%:
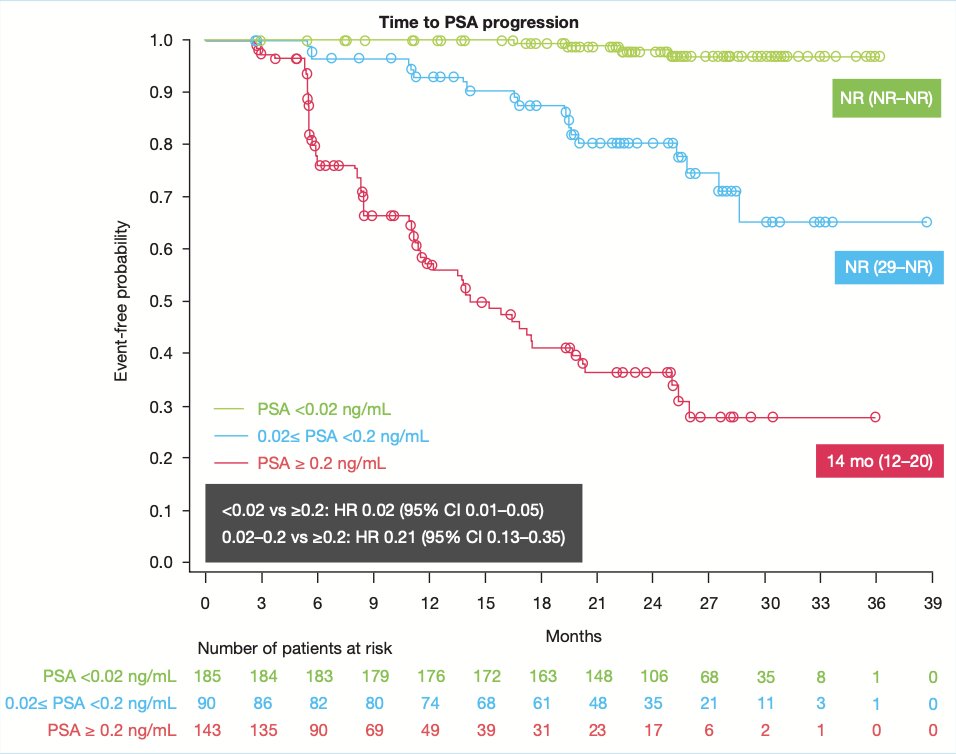
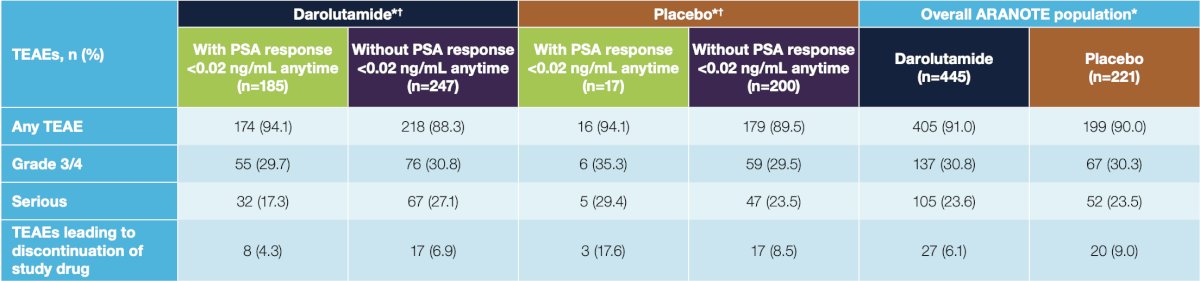
In landmark analyses, these associations held up in an assessment of the effect between PSA response levels at a 36-week landmark and subsequent time to event outcomes for darolutamide-treated patients (PSA <0.02 ng/mL versus PSA >0.2 ng/mL: radiographic progression free survival HR 0.20 95% CI 0.10-0.40; time to mCRPC HR 0.22, 95% CI 0.11-0.41; time to PSA progression HR 0.10, 95% CI 0.04-0.29). The safety profile of darolutamide was independent of PSA response, with lower treatment discontinuation rates due to treatment emergent adverse events versus placebo, consistent with the overall population:
Dr. Shore concluded his presentation discussing ultra-low PSA response with darolutamide plus ADT in ARANOTE with the following take home points:
- Regardless of baseline PSA, the proportion of patients reaching ultra-low PSA response of <0.02 ng/mL was higher with darolutamide treatment versus placebo and ultra-low PSA response rates increase with time
- Ultra-low PSA responses were associated with improved clinical outcomes for patients treated with darolutamide, prolonging radiographic progression free survival and delaying times to mCRPC and PSA progression
- Darolutamide was well tolerated across PSA response subgroups with lower treatment discontinuation rates due to treatment emergent adverse events versus placebo
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: ARANOTE Study Shows Benefits of Deep PSA Response with Darolutamide - Neal Shore
References: