(UroToday.com) The 2025 AUA annual meeting featured a radiation therapy for localized prostate cancer session and a presentation by Dr. Anne Hong discussing the safety of stabilized hyaluronic acid as a rectal spacer. Radiation therapy is a mainstay of treatment in prostate cancer, however, the rectum is at risk due to its proximity to the prostate. To protect the rectum, rectal spacers have demonstrated benefits, reducing the radiation dose on the rectum and thus reducing gastrointestinal side effects. Rectal spacers are generally a benign product; however, when placed in the incorrect position, they can be detrimental. Stabilized hyaluronic acid has recently been approved for use as a rectal spacer and reduces gastrointestinal toxicity in this setting.1 It has several advantages, including its reversibility using hyaluronidase. However, stabilized hyaluronic acid is not immune to rectal wall infiltration, and having access to hyaluronidase may be beneficial in cases of rectal wall infiltration. This study, presented at the AUA 2025 annual meeting, aimed to evaluate the management and outcomes of patients with rectal wall infiltration following stabilized hyaluronic acid rectal spacer insertion.
This was a retrospective analysis of prostate cancer patients who developed rectal wall infiltration after stabilized hyaluronic acid rectal spacer insertion between 2021 and 2024 in Australia. Data included patient characteristics, rectal wall infiltration grading according to the Fisher Valuck Criteria, rectal wall infiltration volume, management strategies (reversal versus observation), radiation therapy delays, and toxicities. Patients with rectal wall infiltrations were identified based on post-procedure MRI. The patients were followed during and post radiation therapy and assessed for rectal complications.
Among 5,788 stabilized hyaluronic acid spacer patients, there were 16 identified rectal wall infiltrations (0.3%):
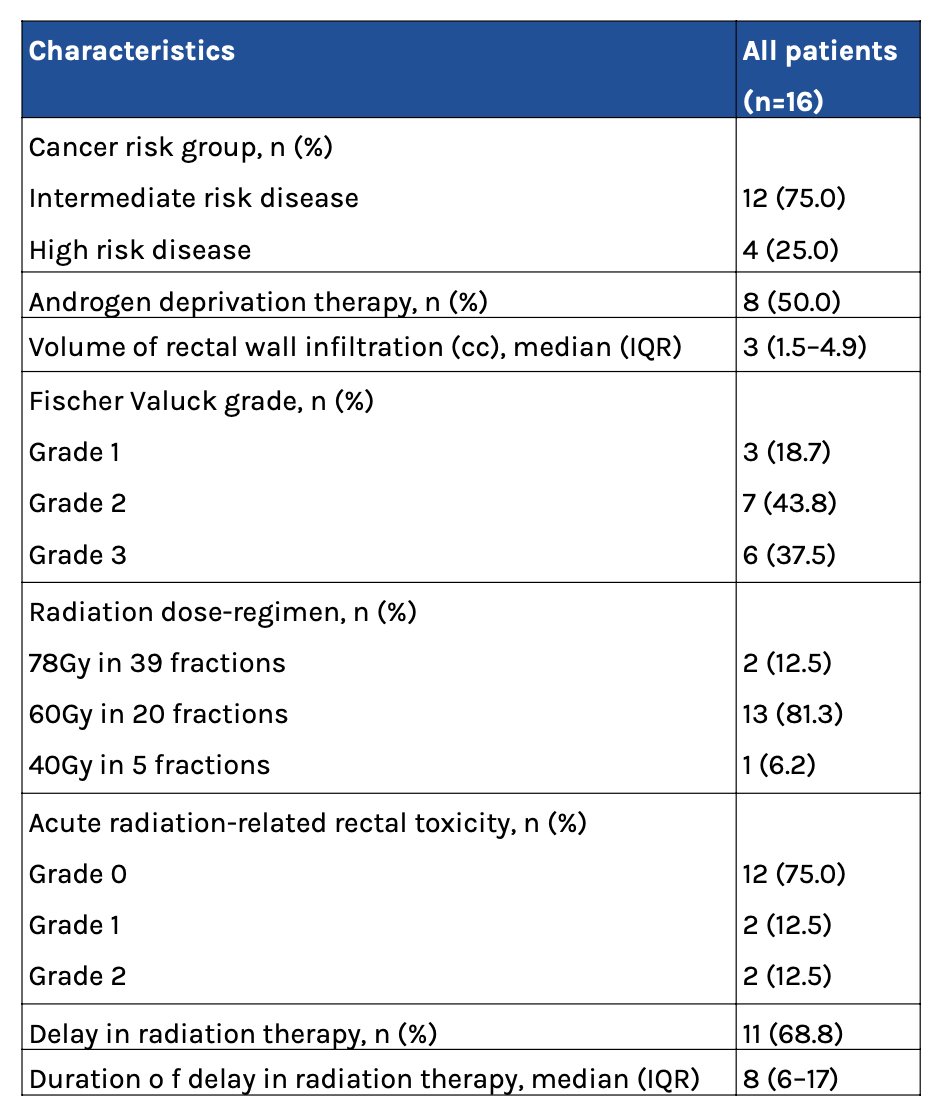
Three patients had grade 1 (18.7%), seven (43.8%) had grade 2, and six (37.5%) had grade 3 rectal wall infiltration (Fisher Valuck criteria), of which all patients were asymptomatic:
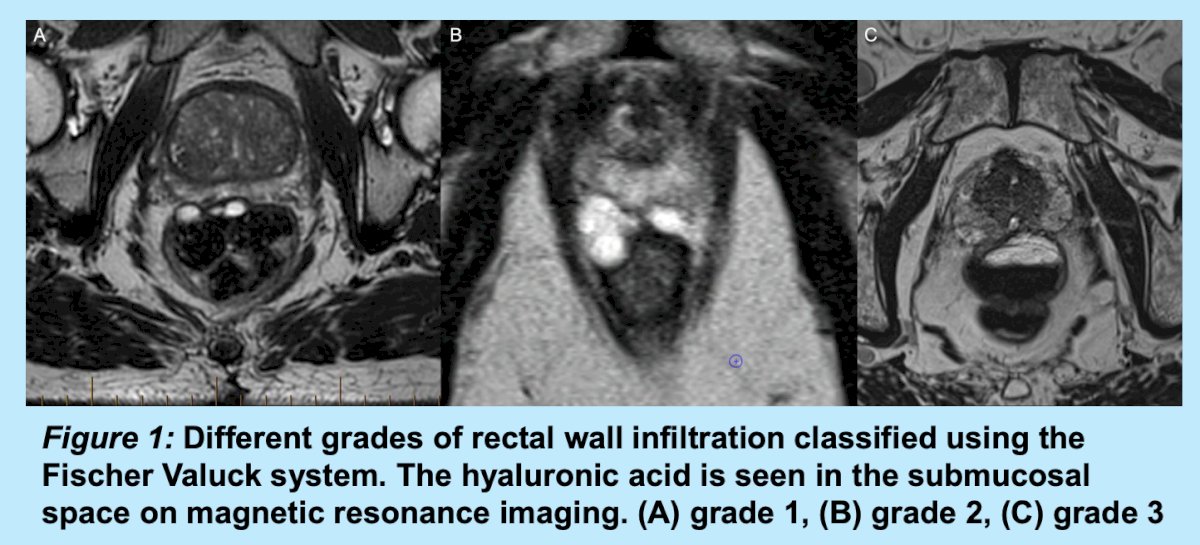
The median rectal wall infiltration volume was 3.0 ml (IQR 1.5–4.9 ml). A higher grade of rectal wall infiltration was correlated with a higher volume of rectal wall infiltration (Spearman’s rho = 0.93, p < 0.001). Digital rectal examination did not detect abnormalities in any patients. There were 12 patients (including all grade 3 rectal wall infiltrations) who received a sigmoidoscopy out of caution, and intact mucosa was confirmed in all cases:

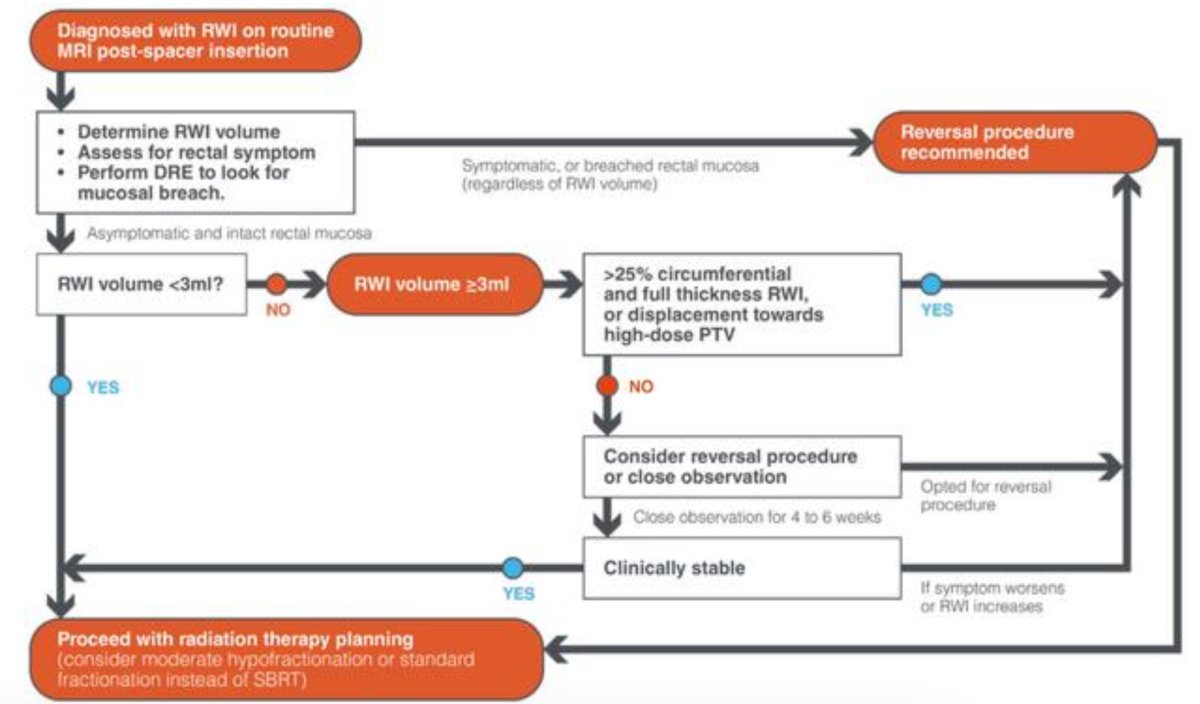
Patients with infiltration volumes of 3 mL or greater experienced delays more frequently, with 7 requiring reversal procedures. All successfully resumed radiation therapy without major complications. In contrast, 9 patients with infiltration volumes <3 mL had either no delays or short delays < 2 weeks. ROC analysis for rectal wall infiltration volume predicting delayed radiation therapy yielded an area under the curve of 0.764 (95% CI 0.523-1.00) with 3 mL as an optimal cutoff. Based on this data, a clinical decision pathway was constructed:
After reversal, one patient underwent successful reinsertion of stabilized hyaluronic acid, which was done with hydrodissection immediately prior, and the proceduralist rated the reinsertion procedure as “easy.” Subsequent pelvic MRI confirmed that the stabilized hyaluronic acid spacer was correctly placed prior to initiation of radiation therapy. On follow-up, acute rectal toxicity was experienced by four patients. Using the CTCAE score, two patients experienced grade 1 rectal toxicities and two patients experienced grade 2 rectal toxicities. No patients developed rectal ulcers, pelvic abscesses, or fistulas.
Dr. Hong concluded her presentation discussing the safety of stabilized hyaluronic acid as a rectal spacer with the following take home points:
- Stabilized hyaluronic acid is increasingly used as a rectal spacer to reduce radiation related gastrointestinal side effects in prostate cancer treatment. Rectal wall infiltration is uncommon but a potentially serious complication. However, rectal wall infiltration can be safely managed using either observation or reversal
- Sigmoidoscopy may not be routinely required if the patient is asymptomatic and digital rectal exam is normal
- The decision to reverse rectal wall infiltration is dependent on the patient’s symptoms, clinical assessment, and volume of rectal wall infiltration
- It is possible to re-insert stabilized hyaluronic acid after a reversal procedure
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References: