(UroToday.com) The 2025 AUA annual meeting featured an advanced prostate cancer session and a presentation by Dr. Neal Shore discussing health-related quality of life, pain and safety outcomes in the phase 3 PSMAfore study of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer (mCRPC). 177Lu-PSMA-617 is a PSMA-targeted radioligand therapy for the treatment of patients with mCRPC. Previously, the phase 3 VISION study showed efficacy of 177Lu-PSMA-617 in patients with mCRPC who were previously treated with at least one androgen receptor pathway inhibitor and 1-2 taxane-based chemotherapies.1
In the PSMAfore study, taxane-naive, PSMA-positive patients with mCRPC who received 177Lu-PSMA-617 had prolonged radiographic progression-free survival versus those who received a change of androgen receptor pathway inhibitor [2]. In addition to extending survival and delaying disease progression, optimal treatment of mCRPC also includes consideration of patients’ health related quality of life. Symptomatic skeletal events significantly impact quality of life of individuals with bone metastasis, affecting up to 90% of patients with mCRPC. At the AUA 2025 annual meeting, Dr. Shore and colleagues presented data for time to first symptomatic skeletal event (excluding death) and post-hoc analyses for time to worsening (excluding clinical progression) in health-related quality of life and pain (data cut-off February 27, 2024).
Eligible patients for PSMAfore had mCRPC with =>1 PSMA-positive and no exclusionary PSMA-negative metastatic lesions, and were candidates for androgen receptor pathway inhibitor change after progression on one prior androgen receptor pathway inhibitor. Patients were randomized 1:1 to open-label 177Lu-PSMA-617 or androgen receptor pathway inhibitor change. Patients continued treatment until completion of 6 cycles of 177Lu-PSMA-617, unacceptable toxicity, radiographic progression, requirement for prohibited therapy or withdrawal. The primary endpoint was radiographic progression-free survival, and secondary endpoints included time to first symptomatic skeletal event, time to worsening in patient-reported health-related quality of life (FACT-P, EQ-5D-5L), and pain (BPI-SF).
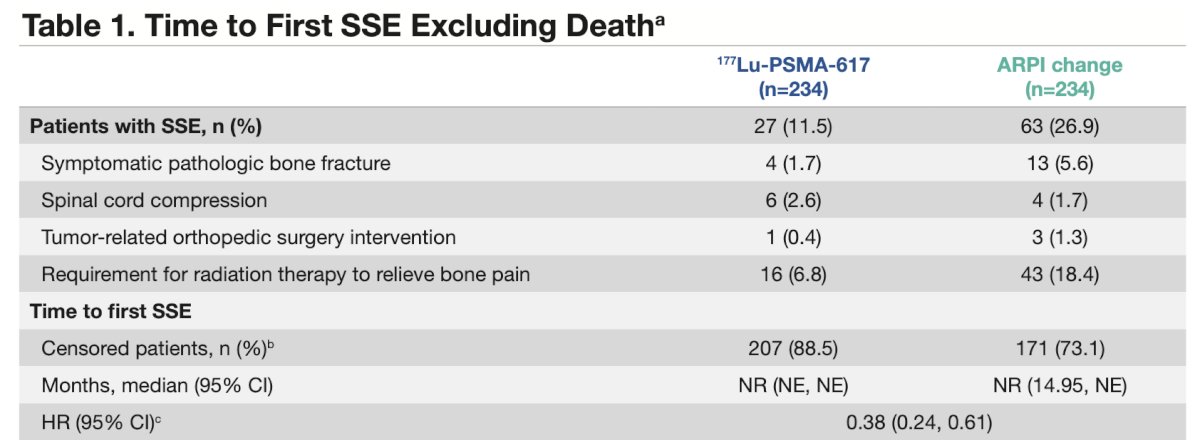
In total, 468 patients were randomized (234 in each arm). At the time of data cut-off, 57% of patients assigned to the androgen receptor pathway inhibitor change group had crossed over to receive 177Lu-PSMA-617. The median duration of follow-up was 24.11 months (IQR 7.36) in the 177Lu-PSMA-617 group and 24.13 months (IQR 7.13) in the androgen receptor pathway inhibitor change group. The median time to first symptomatic skeletal event was not estimable in both groups (HR 0.38; 95% CI 0.24–0.61):
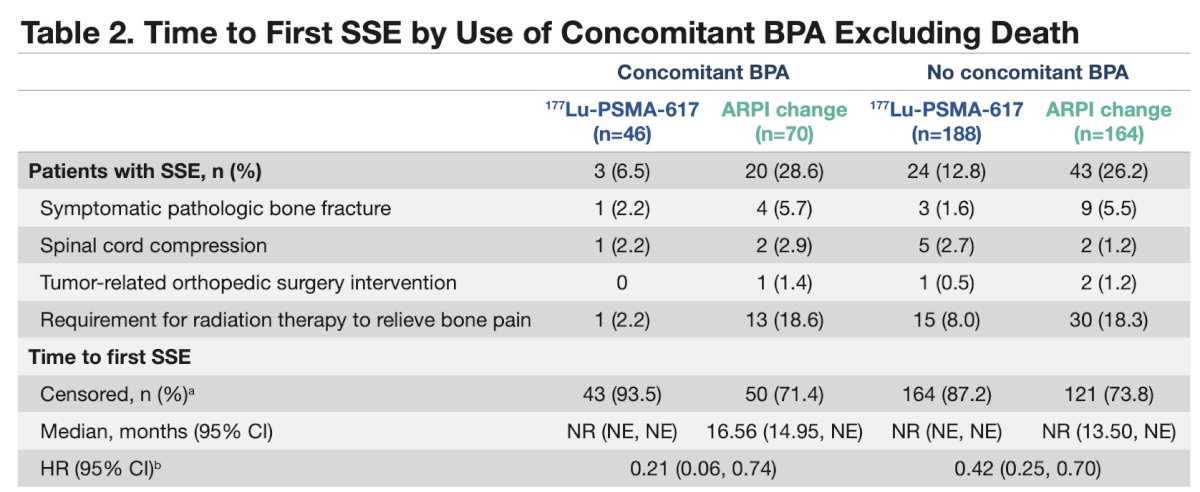
Similar results were seen in subgroups of patients who did and did not receive a concomitant bone protective agent:
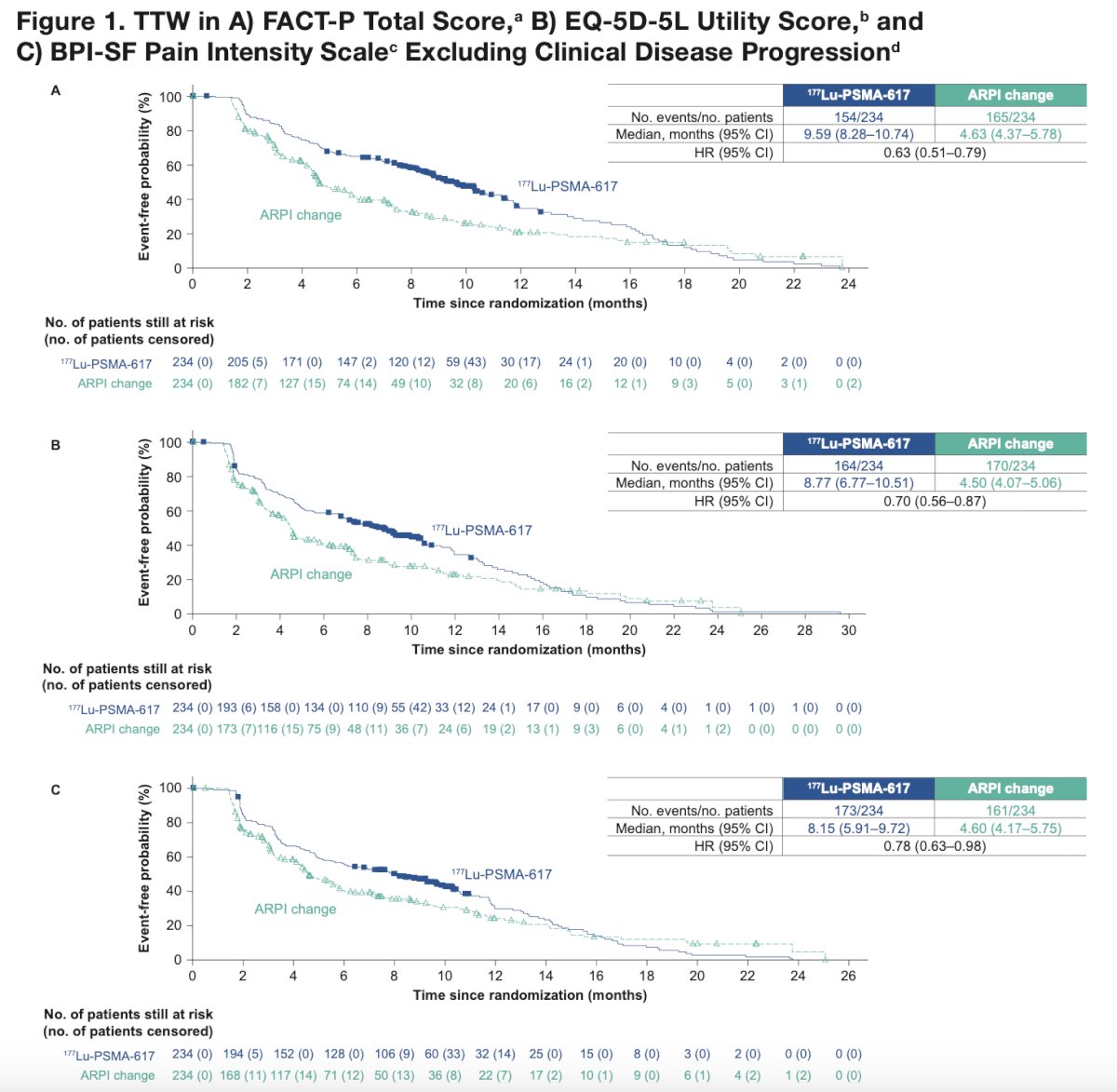
Median time to worsening in FACT-P total score was 9.6 versus 4.6 months (HR 0.63, 95% CI 0.51–0.79), in EQ-5D-5L utility score was 8.8 versus 4.5 months (HR 0.70, 95% CI 0.56–0.87), and in BPI-SF pain intensity was 8.2 versus 4.6 months (HR 0.78, 95% CI 0.63–0.98) in the 177Lu-PSMA-617 versus androgen receptor pathway inhibitor change groups, respectively:
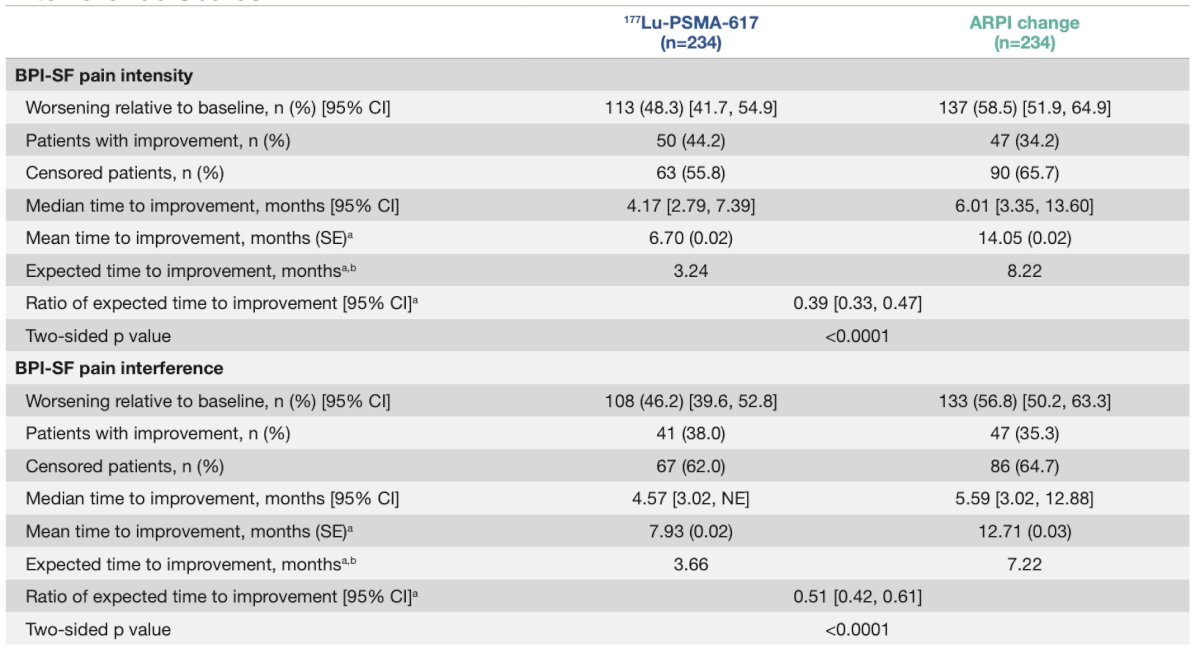
After initial worsening in BPI-SF pain intensity (excluding clinical progression or death), the median time to improvement was 4.2 versus 6.0 months in the 177Lu-PSMA-617 versus androgen receptor pathway inhibitor change groups, respectively. The median time to improvement after initial worsening in BPI-SF pain interference was 4.6 months in the 177Lu-PSMA-617 group and 5.6 months in the androgen receptor pathway inhibitor group:
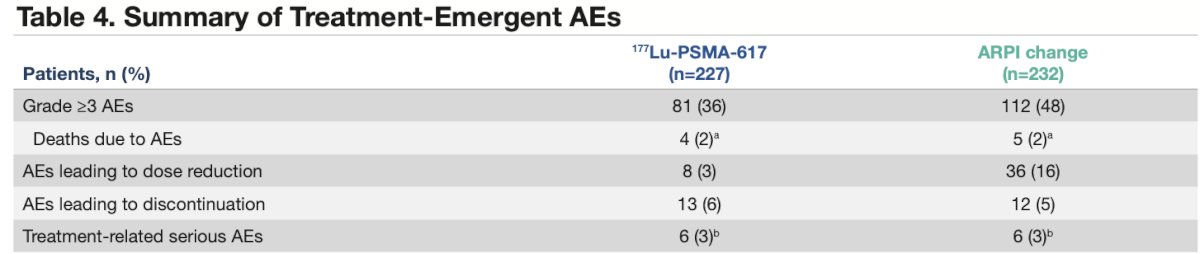
Lower incidences of grade =>3 treatment-emergent adverse events and serious adverse events were observed in the 177Lu-PSMA-617 group versus the androgen receptor pathway inhibitor change group, as previously published. The proportion of patients who experienced treatment emergent adverse events leading to treatment discontinuation was low and comparable between groups:
Dr. Shore concluded his presentation discussing health-related quality of life, pain and safety outcomes in the phase 3 PSMAfore study of 177Lu-PSMA-617 in patients with mCRPC with the following take home points:
- Post-hoc analyses of PSMA-positive, taxane-naive patients with mCRPC who received 177Lu-PSMA-617 showed a delayed time to first symptomatic skeletal event, with or without a concomitant bone protective agent, and longer time to worsening in patient-reported health-related quality of life and pain
- 177Lu-PSMA-617 led to shorter median time to improvement after worsening in pain intensity and a favorable safety profile compared with androgen receptor pathway inhibitor change
- Together with the previously reported significant prolongation of radiographic progression free survival (primary endpoint) in PSMAfore, these results support the use of 177Lu-PSMA-617 as a treatment option for taxane-naïve patients with mCRPC who have disease progression once on an androgen receptor pathway inhibitor and who are candidates for androgen receptor pathway inhibitor change
Presented by: Neal Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), Medical Director for the Carolina Urologic Research Center, AUC Urology Specialists, Myrtle Beach, South Carolina
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
Related content: Health-Related Quality Outcomes for Pre-Chemotherapy mCRPC Treatment - Neal Shore
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.