(UroToday.com) The 2025 AUA annual meeting featured an advanced prostate cancer session and a presentation by Dr. Christopher Pieczonka discussing data from the prespecified third interim analysis of the darolutamide observational (DAROL) study in North American patients with non metastatic castration resistant prostate cancer (nmCRPC). Darolutamide is a highly potent androgen receptor inhibitor that is structurally distinct by design, with low blood-brain barrier penetration and limited potential for drug-drug interactions.
Darolutamide is approved for treatment of nmCRPC based on significantly prolonged metastasis-free survival, overall survival, and favorable safety and tolerability in the phase 3 ARAMIS study.1,2 The DAROL study is assessing the real-world safety and effectiveness of darolutamide in patients with nmCRPC. At the 2025 AUA annual meeting, Dr. Pieczonka and colleagues reported a subgroup analysis of North American patients from the prespecified third interim analysis.
DAROL is an ongoing, global, open-label, single-arm, non-interventional study in patients aged =>18 years with nmCRPC for whom the decision to be treated with darolutamide was made pre-enrollment. The primary endpoint is safety, including incidence and severity of treatment-emergent adverse events. Secondary endpoints include overall survival, metastasis-free survival, PSA progression, and PSA response. The third interim analysis was conducted when 550 patients completed =>6 months of treatment (data cut-off July 17, 2023):
Of 550 patients, 191 (35%) were from North America (Canada n = 67, USA n = 124). Patient and disease characteristics were generally similar between the North American subgroup and the overall population, and 13% of North American patients were black/African American (overall 5%). Baseline PSA levels (median 3.9 versus 4.1 ng/mL), PSA doubling time (median 5.3 versus 5.4 months), and ECOG 0 (67% versus 64%) were similar in the North American and overall population:

The median time to darolutamide discontinuation or death was not reached (95% CI 26.1 – not estimable) in the North American subgroup and 29.9 months (95% CI 26.7 – not estimable) in the overall population: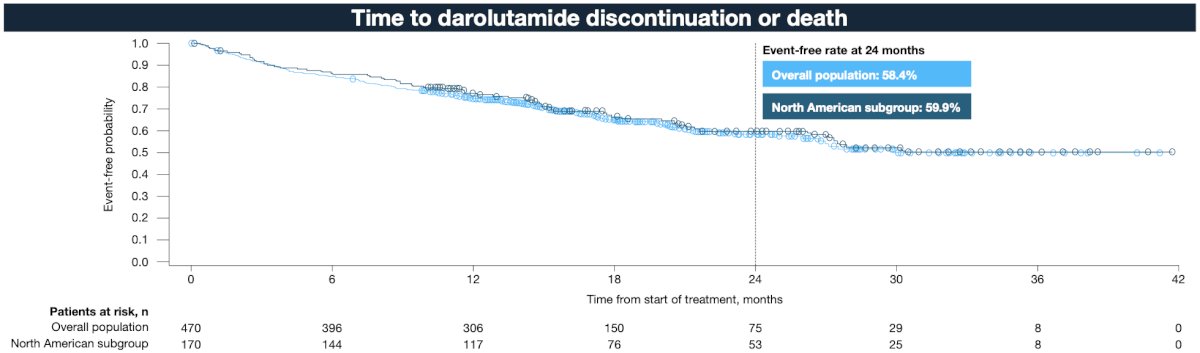
Of the patients who experienced treatment-emergent adverse events (North American 135/191 versus overall 313/550), most were grade 1/2 (North American 69% versus overall 67%), and a similar proportion of patients discontinued treatment due to treatment-emergent adverse events (North American 6% versus overall 7%). With the exception of fatigue (26%), incidences of treatment-emergent adverse events commonly associated with androgen receptor inhibitor therapy were low (<6%) in the North American subgroup and consistent with the overall population:
At 24 months, overall survival rates were similar in the North American subgroup (86.0%) versus the overall population (87.6%):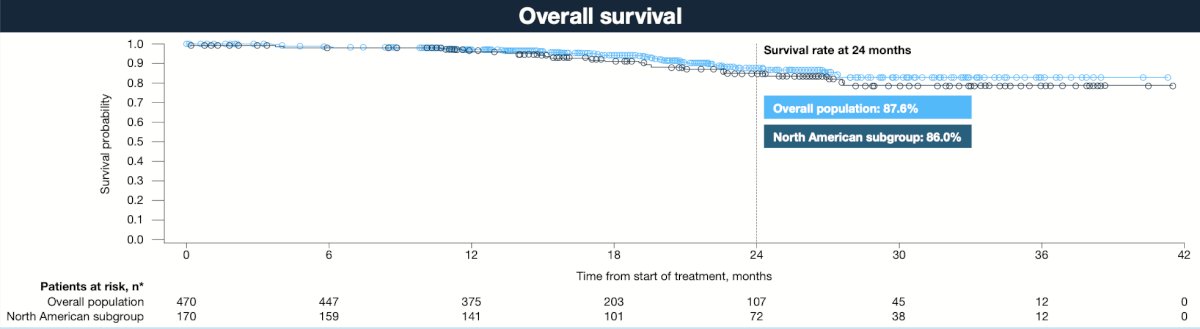
Metastasis free survival and mCRPC-free rates at 24 months were slightly lower in the North American subgroup: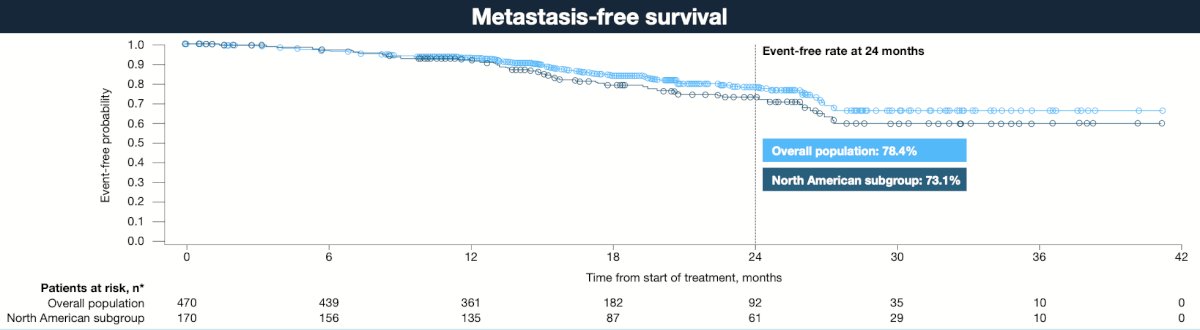

PSA undetectable and progression free rates were slightly higher in the North American subgroup: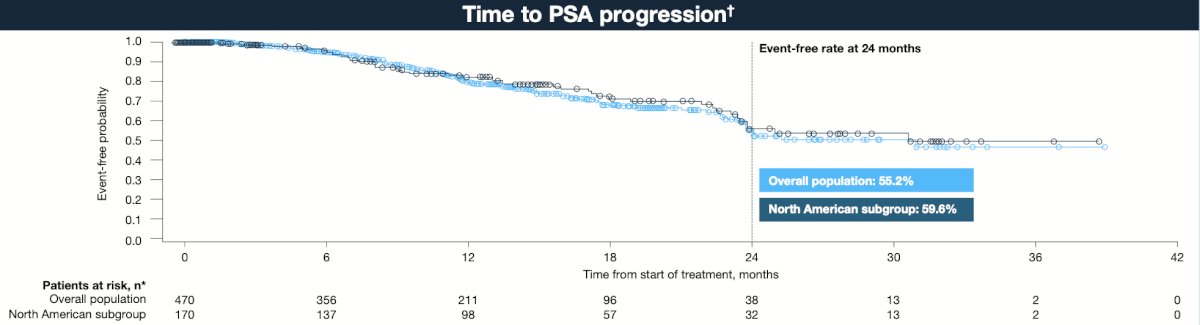
The median time to undetectable PSA (<0.2 ng/mL) was 12.6 months in the North American subgroup and 16.5 months in the overall population:
The proportions of patients who achieved 50% or 90% reductions in PSA from baseline were similar in the North American subgroup and in the overall population:
Dr. Pieczonka concluded his presentation discussing data from the prespecified third interim analysis of the darolutamide observational (DAROL) study in patients with nmCRPC with the following take-home points:
- Under real-world conditions, darolutamide was well tolerated in the North American subgroup and had a favorable safety profile, consistent with the established safety profile of the compound, without any new safety findings
- Effectiveness findings from the DAROL third interim analysis, North American subgroup, were generally similar to those of the overall population
- These results confirm the findings of the phase 3 ARAMIS trial in a clinically diverse, real world North American population
Presented by: Christopher Pieczonka, MD, Associated Medical Professionals of NY, Syracuse, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
References:
- Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235-1246.
- Fizazi K, Shore N, Tammela TL, et al. Nonmetastatic, Castration-Resistant Prostate Cancer and Survival with Darolutamide. N Engl J Med. 2020 Sep 10;383(11):1040-1049.