The RADICALS-HD trial demonstrated that the use of 24 months of ADT, compared to 6 months, in combination with radiotherapy in the post-operative setting was associated with significant improvements in metastasis-free survival.1 However, whether these findings are generalizable to patients harboring nodal metastases (pN1) after radical prostatectomy remains unknown, since only 3-8% of the entire RADICALS-HD cohort included patients with pN1 disease. Thus, the objective of this study was to evaluate whether long-term ADT was associated with improved survival outcomes in a pN1 patient cohort.
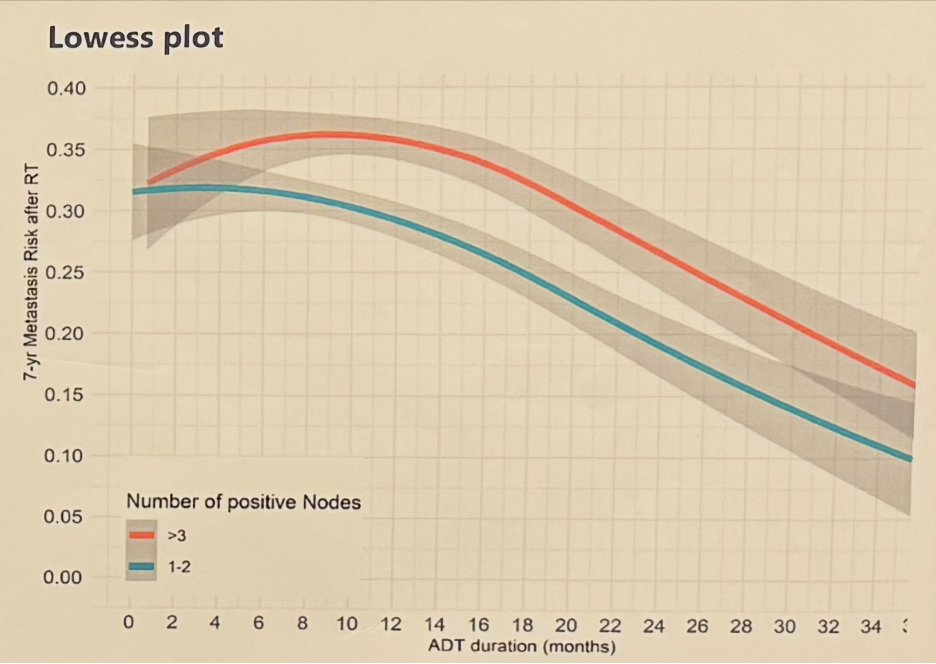
This was a single center, retrospective analysis of 588 pN1 patients receiving post-operative radiotherapy + ADT between 1987 and 2023. Survival analyses using Kaplan-Meier curves and multivariable Cox regression modeling, adjusted for age, pT stage, pathologic Gleason Score, and number of positive nodes, were performed. The Lowess function was used to explore the relationship between the duration of ADT use and the 7-year rate of metastatic progression. An interaction test was performed to evaluate whether the impact of ADT duration varied by the number of positive nodes (1–2 versus >2).
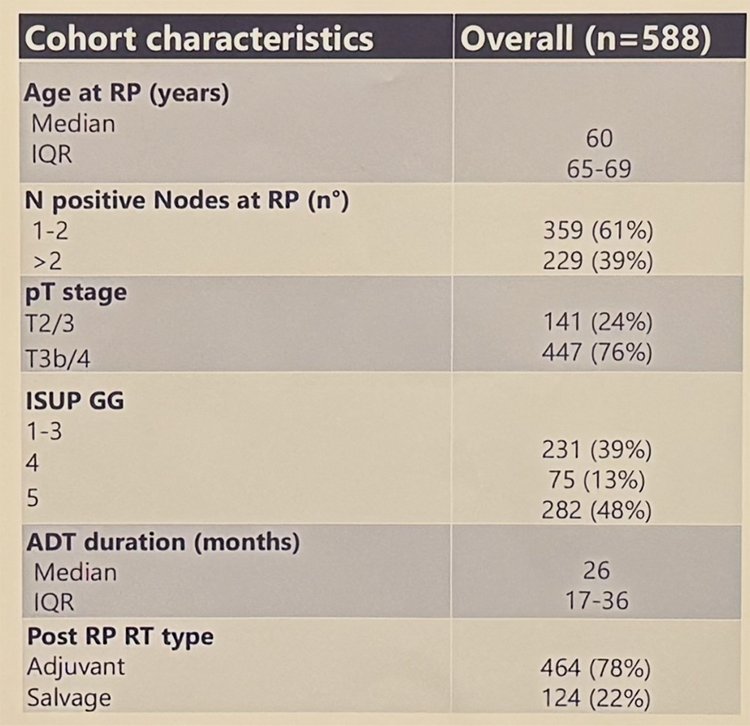
The baseline patient characteristics are summarized in the table below. 61% of patients had 1-2 pathologically positive nodes, and 39% had >2 nodes involved. 76% had pT3b-4 disease. The median ADT duration was 26 months (IQR: 17–36). 78% of patients received radiotherapy in the adjuvant setting and 22% in the salvage setting.
The 7-year metastasis-free survival rate was 72% (95% CI: 68-76%). On multivariable analysis, longer ADT use (2-months units) was associated with reduced rates of metastases (HR: 0.93, 95% CI: 0.90–0.97, p=0.03). The beneficial effect of ADT was visible after 12 months of treatment, without a visible plateau up to 36 months of treatment, and did not significantly vary by the nodal burden (p-value for interaction test >0.05).
Based on these results, Dr. Barletta concluded that in node-positive patients receiving post-operative radiotherapy + ADT, a longer duration of ADT use was associated with an improved survival benefit, with no plateau effect observed and no differential benefit by nodal disease burden.
Presented by: Francesco Barletta, MD, Urology Resident and Clinical Researcher, The IRCCS Ospedale San Raffaele, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References: