(UroToday.com) The American Urologic Association (AUA) 2025 Annual Meeting held in Las Vegas, NV between April 26th and 29th, 2025 was host to The International Prostate Forum. Dr. Andrew Hahn discussed the underutilization of systemic therapy intensification in the metastatic hormone-sensitive setting despite the abundance of randomized trials demonstrating survival benefits for doublet and triplet therapy regimens in this setting.
Dr. Hahn began with a case presentation of an 84-year-old male who presented with a PSA of 271 ng/ml. He underwent a staging scan with a PSMA PET, which demonstrated evidence of widespread metastases. Following his diagnosis, he was started on degarelix and transitioned to leuprolide 4 weeks later.

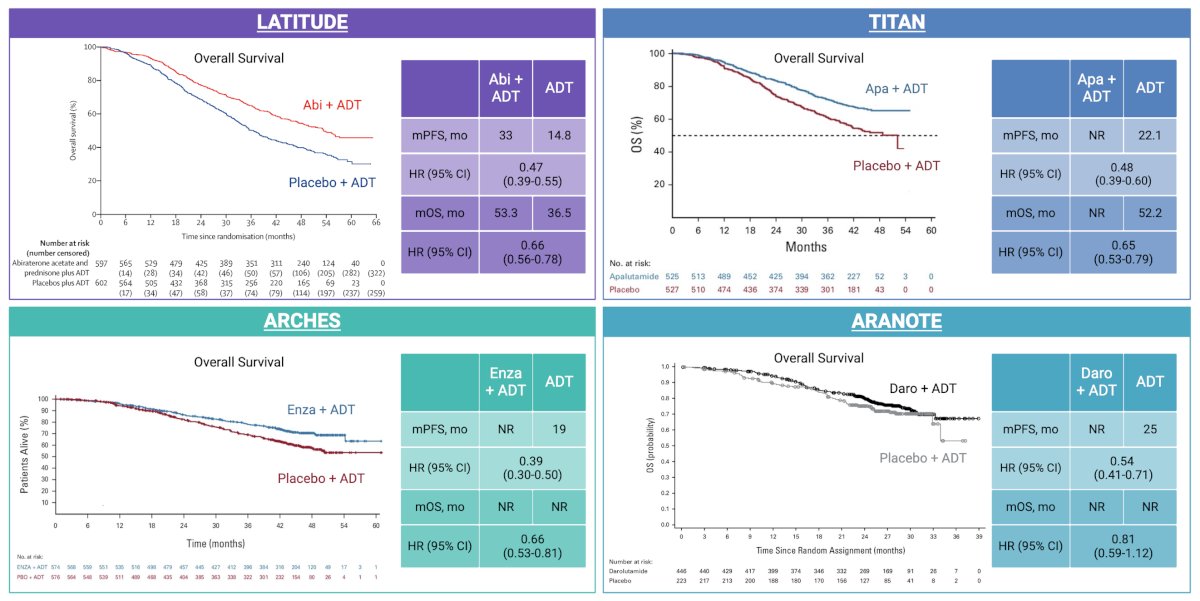
Dr. Hahn noted that, in this setting, the minimum standard of care therapy is ADT + an androgen receptor pathway inhibitor (ARPI). There are numerous trials that have demonstrated significant survival benefits with the addition of an ARPI to ADT in the metastatic hormone-sensitive setting, with Dr. Hahn highlighting the following trials:
- LATITUDE: ADT + abiraterone (median overall survival [OS]: 53.3 versus 36.5 months; HR: 0.66, 95% CI: 0.56–0.78)1,2
- TITAN: ADT + apalutamide (median OS: Not reached versus 52.2 months; HR: 0.65, 95% CI: 0.53–0.79)3,4
- ARCHES: ADT+ enzalutamide (median OS: Not reached in both arms; HR: 0.66, 95% CI: 0.53–0.81)5,6
- ARANOTE: ADT + darolutamide
- Significant progression-free survival (PFS) benefit (HR: 0.54, 95% CI: 0.41–0.71)
- No significant OS benefit to date (HR: 0.81; 95% CI: 0.59–1.12)
Given that there are numerous doublet therapy intensification options for patients with mHSPC, how can we select the appropriate regimen for this patient? One important consideration is the unique toxicity profiles of the different ARPIs, summarized in the table below:
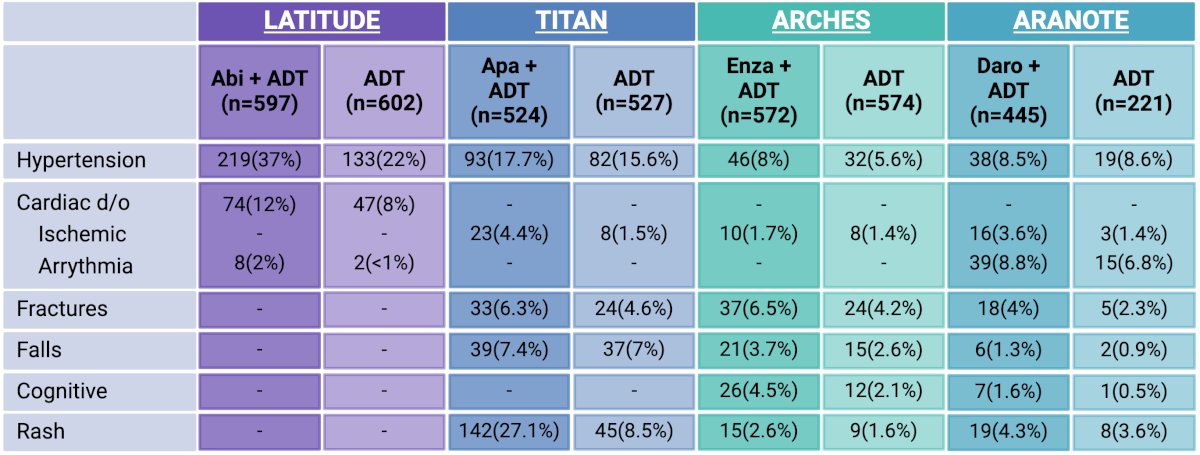
Abiraterone is associated with high rates of hypertension (37% versus 22% with ADT alone). Rashes are a notable potential adverse effect of apalutamide (27% versus 8.5%). All agents are associated with variably increased rates of cardiovascular events, fractures, and falls.
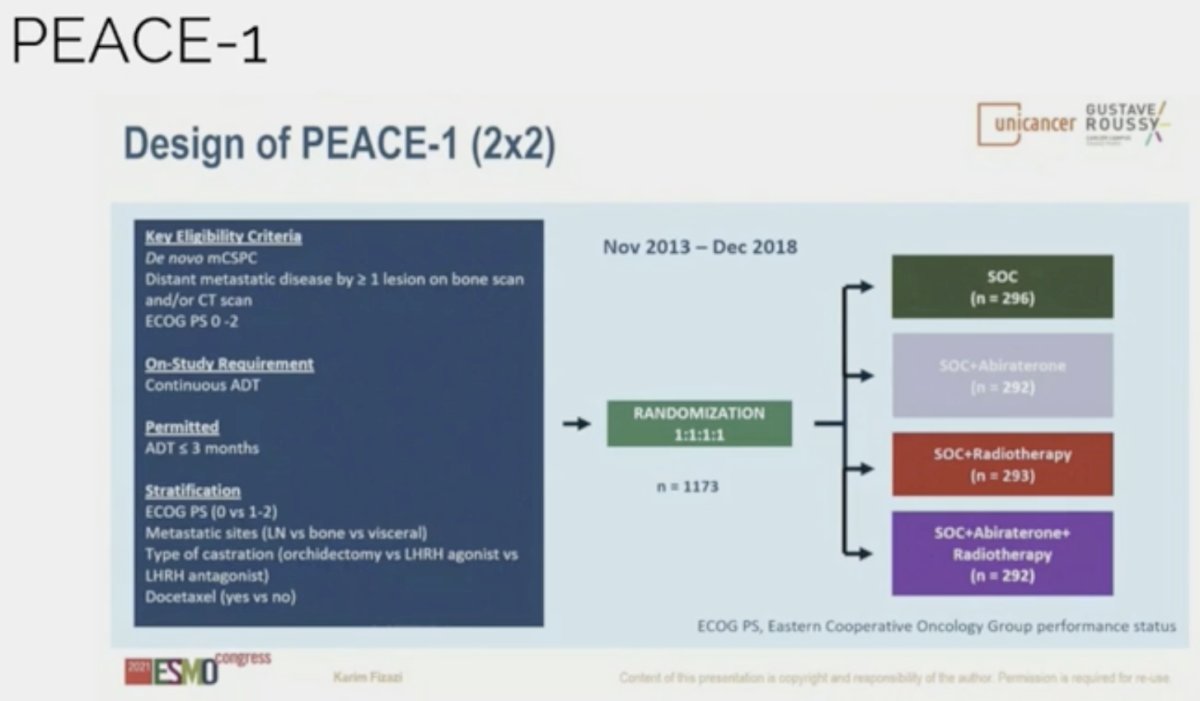
In addition to ARPI doublet therapy, another option for select patients, particularly those with high-volume, de novo disease, is triplet therapy with ADT + an ARPI (abiraterone or darolutamide) + docetaxel, based on results of the PEACE-1 and ARASENS trials.8,9
PEACE-1 is a randomized phase III trial that employed a 2x2 design to assess, separately and combined, the impact of the addition of abiraterone acetate/prednisone and radiation to standard of care (SOC) therapy in men with de novo mHSPC. The control arm in this study evolved to reflect the contemporary SOC. When the study began enrolling patients, the SOC for first-line mHSPC was ADT alone. With publication of data from the STAMEDE and CHAARTED, SOC was updated to include ADT plus docetaxel 75 mg/m2 every 3 weeks for 6 cycles.
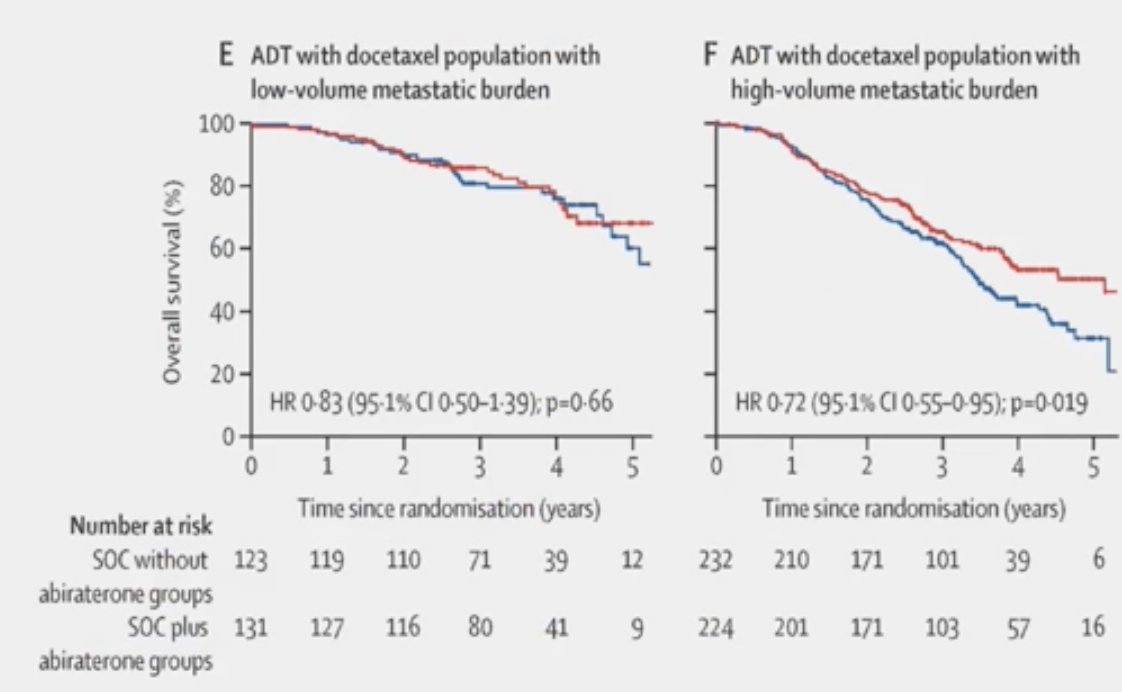
The addition of abiraterone resulted in an 18% improvement in overall survival, with a median overall survival of 4.7 years in the SOC arm and 5.7 years in the SOC plus abiraterone arm (HR 0.82, 95% CI: 0.69–0.98; p=0.03).8
The ARASENS trial is an international, double-blind, phase III study that enrolled patients with mHSPC and ECOG performance status 0 or 1 (NCT02799602). Once accrued, patients were randomized 1:1 to darolutamide 600 mg twice daily or matching placebo in addition to SOC comprising ADT and docetaxel. The primary endpoint was overall survival.
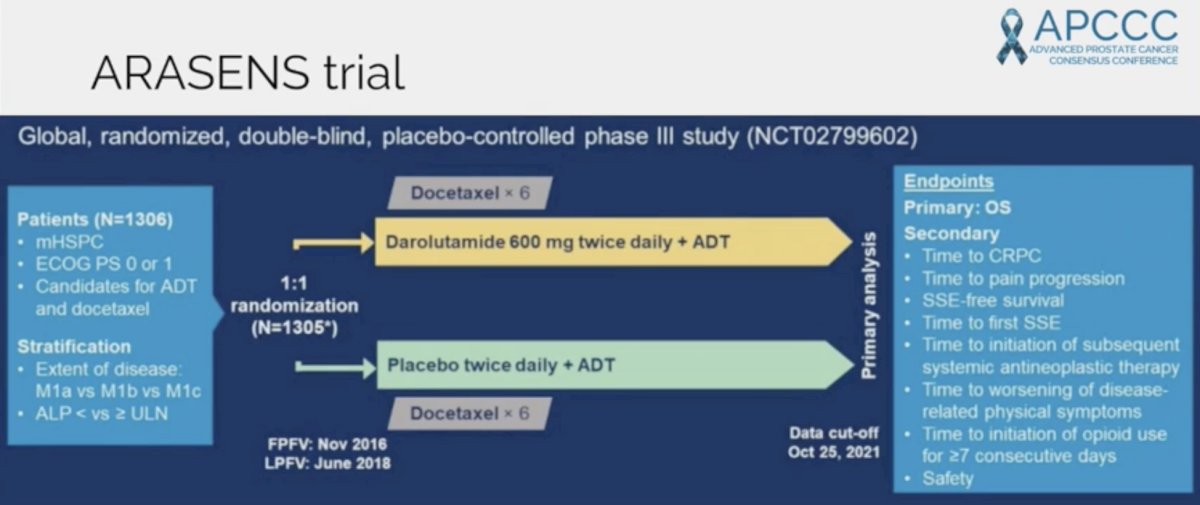
With a primary data cut-off of Oct 25, 2021, the authors observed a significant 32.5% decreased rate of death among patients treated with darolutamide compared to placebo (HR: 0.675, 95% CI 0.568–0.801; p<0.0001). A larger proportion of patients initially randomized to placebo received subsequent life-prolonging systemic antineoplastic therapy (75.6%) than those initially randomized to darolutamide (56.8%), again highlighting the overall survival benefits of early treatment intensification. When stratified by disease presentation (de novo versus recurrent), darolutamide showed consistent overall survival benefits. In patients with de novo metastatic disease, HR for overall survival was 0.71 (95% CI: 0.59–0.85). The magnitude of effect was even more pronounced in those with recurrent metastatic disease (HR: 0.61, 95% CI: 0.35–1.05).9
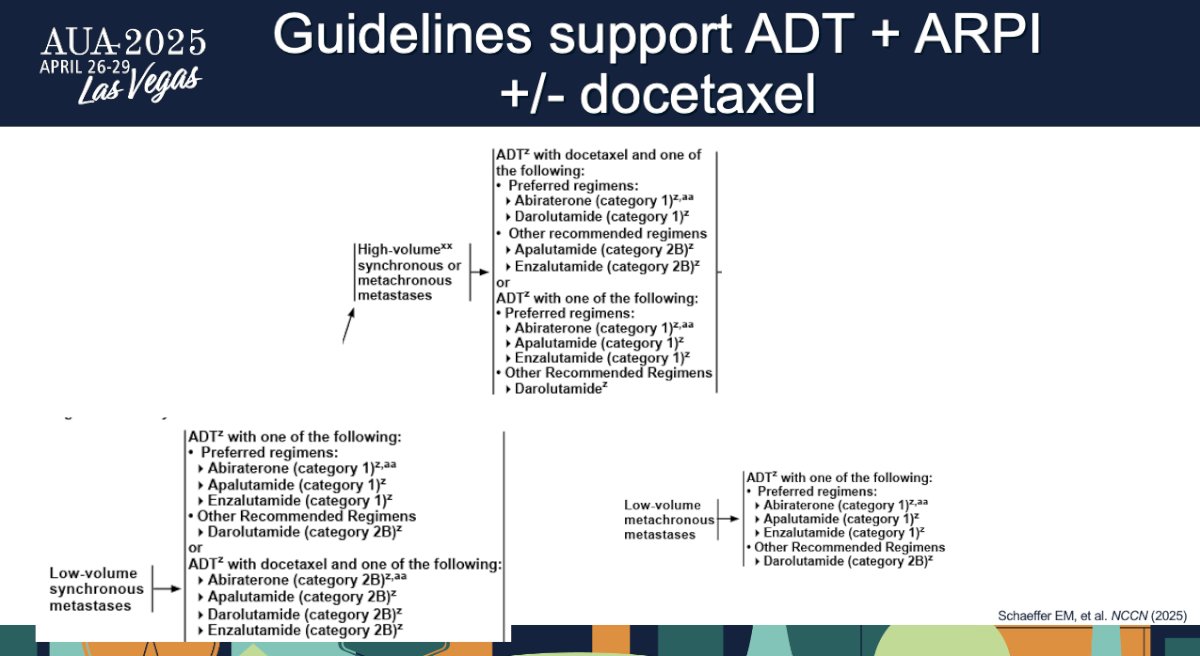
Currently, the NCCN guidelines support the use of triplet therapy regimens for select patients with high-volume metastases as a category 1 recommendation (synchronous or metachronous) and low-volume, synchronous metastases as a category 2B recommendation.
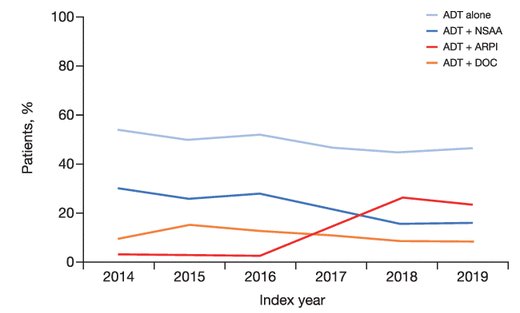
However, despite these recommendations, real-world data suggest that ADT monotherapy use persists in current practice and that the early uptake of ADT + ARPI has been lower than expected. Notable limitations of these studies, however, include missing variables from real-world databases and the fact that most of these studies do not report on uptake in the last 2–3 years.
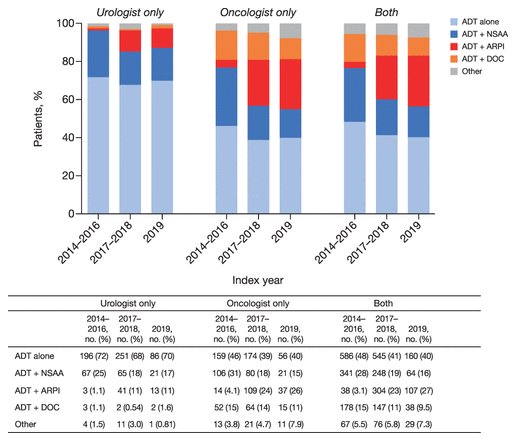
What are some of the reasons/factors that explain the continued use of ADT monotherapy? The most important variable appears to be the specialty of the prescribing physicians. In a real-world study of initial prescription patterns for mHSPC patients between 2014 and 2019, 90% of urologists prescribed ADT + a first-generation non-steroidal anti-androgen (NSAA) versus 64% of oncologists – both proportions alarmingly high.10
Other important variables associated with prescription patterns included:11
- Older age of patients
- Non-White race
- Higher comorbidity burden
- Rural setting
- Community practice
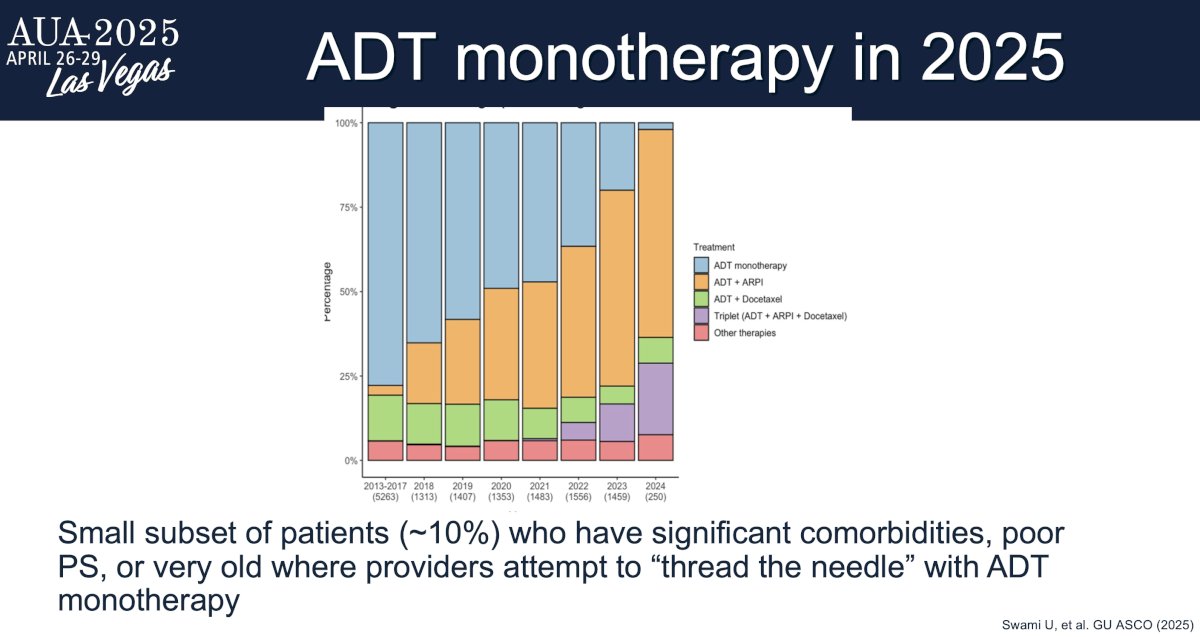
More recent data from the Flatiron US database presented at ASCO GU 2025 by Swami et al. demonstrates that the use of ADT monotherapy has significantly decreased in clinical practice, with only 24% of mHSPC patients being prescribed ADT monotherapy since 2023 and only 10% in 2024.12
In addition to evaluating barriers and facilitators to treatment intensification in the real world, further research is needed to better understand why patients experience differential toxicity with hormone therapy. Dr. Hahn noted that comorbidities, such as diabetes mellitus, likely contribute; however, early evidence suggests that inherited ‘vulnerabilities’ may predispose patients to drug-related toxicities.
Going back to the case presentation, the 84-year-old patient experienced mild fatigue with degarelix, but continued to work as a farmer in the Midwest. He underwent germline DNA next-generation sequencing (NGS) with no pathologic variant identified. On somatic DNA NGS testing, he was found to have loss of PTEN and a TMPRSS2:ERG fusion mutation. He was started on apalutamide doublet intensification. His PSA was undetectable at 6 months follow-up and a radiographic response was noted on conventional imaging. He has remained on therapy with minimal side effects 2.5 years later.
Dr. Hahn concluded as follows:
- ADT + ARPI is the backbone of treatment for men with mHSPC, and there is a role for ADT + ARPI + docetaxel in a subset, defined by clinical and genomic factors
- In the real world, there has been a slow uptake of intensification with an ARPI.
- There is an unmet need to further understand the determinants of harm from hormone therapy and to develop treatment approaches for these patients.
Presented by: Andrew Hahn, MD, Assistant Professor, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:- Fizazi K, Tran N, Fein L, et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2017 ;377(4): 352-60.
- Fizazi K, Tran N, Fein L, et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): Final overall survival analysis of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2019; 20(5): 686-700.
- Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019; 381(1): 13-24.
- OS: Chi KN, Chowdhury S, Bjartell A, et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: Final survival analysis of the randomized, double-blind, phase III TITAN study. J Clin Oncol. 2021; 39(20): 2294-303.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy with Enzalutamide or Placebo in Men with Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol. 2019; 37(32): 2974-86.
- Armstrong AJ, Iguchi T, Azad AA, et al. The efficacy of enzalutamide plus androgen deprivation therapy in oligometastatic hormone-sensitive prostate cancer: A Post hoc analysis of ARCHES. Eur Urol. 2023; 84(2): 229-41.
- Saad F, Vjaters E, Shore N, et al. Darolutamide in combination with androgen-deprivation therapy in patients with metastatic hormone-sensitive prostate cancer from the phase III ARANOTE trial. J Clin Oncol. 2024; 42(36): 4271–81.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022; 399(10336): 1695-707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022; 386(12):1132-42.
- Swami U, Hong A, El-Chaar NN, et al. The role of physician specialty in the underutilization of standard-of-care treatment intensification in patients with metastatic castration-sensitive prostate cancer. J Urol. 2023; 209(6): 1120–31.
- Dodkins J, Nossiter J, Cook A, et al. Does research from clinical trials in metastatic hormone-sensitive prostate cancer treatment translate into access to treatments for patients in the "real world"? A systematic review. Eur Urol Oncol. 2024; 7(1): 14–24.
- Swami U, Jo Y, Ozay Zi, et al. Recent treatment patterns in US-based real-world patients (pts) with metastatic hormone-sensitive prostate cancer (mHSPC). J Clin Oncol. 2025; 43: 5_suppl