(UroToday.com) Sunday afternoon’s plenary session continued with an insightful talk by Dr. José Carlos Truzzi from the Federal University of Sao Paulo. Dr. Truzzi began the session with a brief history of the general understanding of male voiding dysfunction. What was once understood as “prostatism” is nowadays better understood as lower urinary tract symptoms, or “LUTS” through a paradigm shift that occurred over the 1990s. “LUTS”, a term that emerged around 1994 after questioning of “prostatism”, ensured an understanding of nonspecificity in etiology of voiding dysfunction, and not defined as or by one disease.
Dr. Truzzi mentioned, however, that benign prostatic hyperplasia, or “BPH”, patients, symptoms, and management are cited and mentioned heavily in current literature in the context of male voiding dysfunction and lower urinary tract symptoms. Dr. Truzzi reminds us that although patients may have a histological proof of BPH does not guarantee that patients will become or are symptomatic. Even though 50% of men in their 50s and 90% of men in their 80s have histological BPH, this fact alone loses relevance when a patient develops LUTS. Only half of these men who have BPH will have significant prostate enlargement, and only about a quarter of them will experience true obstruction.
On the other hand, patients with small prostates can also have symptoms. The cause-effect relationship, according to Dr. Truzzi, is not straightforward: “Today, we know that the urothelium, neurotransmitters, interstitial cells, and the detrusor muscle play a much bigger role”. Other conditions commonly coexist with BPH, such as detrusor overactivity and detrusor underactivity, which account for up to 60% of LUTS cases.
Urinary symptoms increase with age for both men and women. Classic BPH symptoms are typically defined through a weak stream, dribbling, frequency, incomplete emptying, and nocturia. Dr. Truzzi quoted a video-study containing 3000 men over 40 years of age with moderate to severe International Prostate Symptom Score (IPSS) and poor response to alpha-blockers, only half had bladder outlet obstruction.
“But what about the rest?”
Around 30% had bladder dysfunction, including 28-41% with detrusor hypocontractility, and 5% with detrusor overactivity without bladder outlet obstruction (BOO). Even among those with large prostates, defined as greater than 60 cc in volume, 20% had associated detrusor underactivity.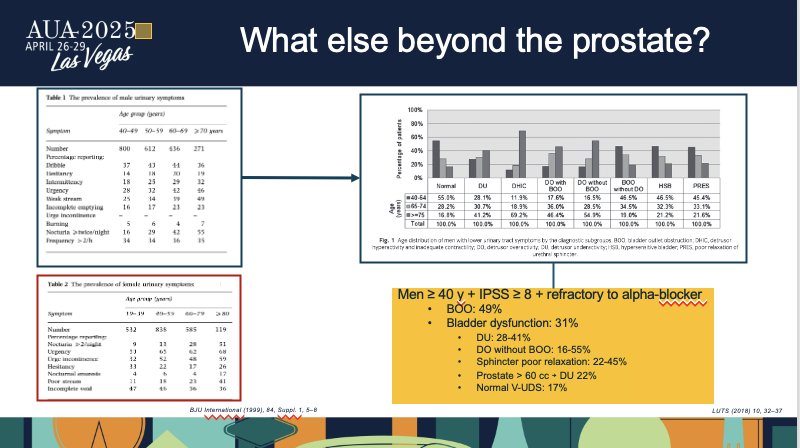
Dr. Truzzi followed up this data with a posing question for the audience: “What else is happening beyond the prostate?”
Although there are many conditions that urologists come across in their daily practice, he reminds us that the three most common ones are detrusor overactivity and overactive bladder (OAB), detrusor underactivity, and nocturnal polyuria.
The term OAB first gained attention in 1997. It took over a decade to arrive at today’s definition of urgency, frequency, and nocturia in the presence or absence of incontinence. OAB is common, affecting around 20% of the worldwide population. However, Dr. Truzzi reminds us that OAB is not the same as detrusor overactivity, and the two must not be confused. Although one can expect to see detrusor overactivity in patients with OAB symptoms, that is not always what urologists find. However, in the context of LUTS and BPH, they can be considered together.
Detrusor overactivity may or may not be related to prostate enlargement. About 60% of men with BPH experience this condition. However, the degree of obstruction does not always correlate with their degree of hyperplasia. Many factors, such as urodynamic patterns, age, cystometric capacity, and combination of such parameters, all in conjunction with how much prostate tissue has been removed after prostate reduction therapies and procedures, have all been proposed to predict whether or detrusor overactivity will persist or not in the postoperative period.

Next, Dr. Truzzi dives into underactive bladder and detrusor underactivity. In men over 40 years of age, both these conditions are highly prevalent and may act as contributors to LUTS. They can have neurogenic, muscular, iatrogenic, or even unknown origins. Indeed, they overlap with the prostatic obstructive process. Symptoms of an underactive bladder, such as a weak stream or hesitancy, are often confused with so-called “prostate symptoms”. The same is true for urodynamic findings of detrusor underactivity, where reduced contraction, prolonged and incomplete bladder emptying, can promote such symptoms. “Unfortunately”, Dr. Truzzi mentions, “we do not yet have great tools to identify these patients ahead of time”.
When we consider the association of smaller prostate size and some urodynamics findings like low urinary flow and reduced detrusor contractility, this might point to underactivity and help us to differentiate detrusor underactivity and BOO. The main takeaway is that urologists should always consider both possibilities in our diagnosis and treatment plans for voiding dysfunction.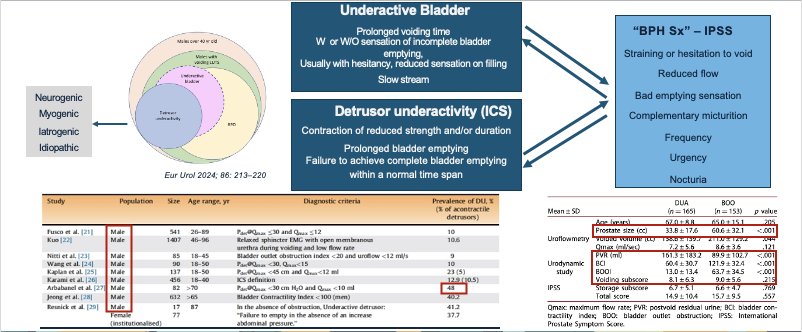
Lastly, Dr. Truzzi touched on nocturia as the third main condition. While it is not the most common symptom, it is one of the most bothersome for patients and significantly negatively impacts their quality of life. Once urologists reduce nocturia, maximal improvement of quality of life occurs. Nocturnal polyuria is found in up to 90% of men with nocturia. Dr. Truzzi mentions that it is relatively easy to diagnose and manage with a simple voiding diary and behavioral changes, such as fluid intake reduction in the evening and nighttime.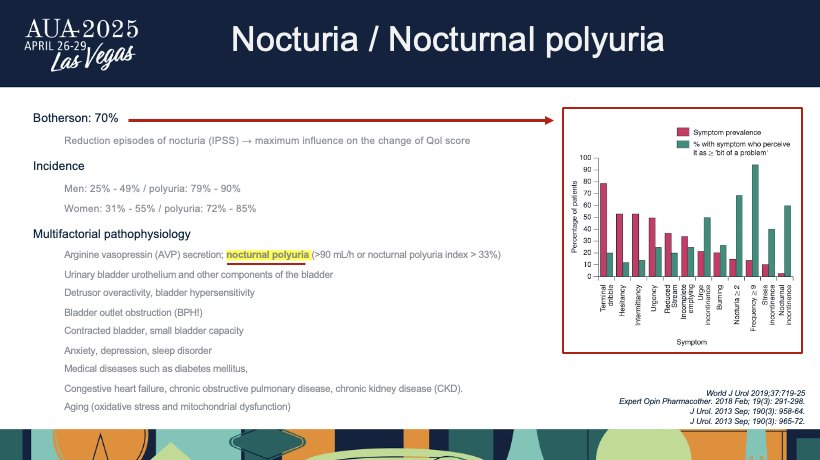
Dr. Truzzi goes on to share a prospective multicenter study where patients had two years of follow up in men with nocturia. Of these men, one group received standard pharmacotherapy for BPH. Another group received no treatment at all. Despite similar baseline prostate size of around 50 cc, flow rates, and post-void residuals, 70% still had bothersome nocturia after treatment. Those not on any medication actually had less nocturia than the treated group. Next, Dr. Truzzi asked, “When we’re managing male LUTS, is treating the prostate truly enough?”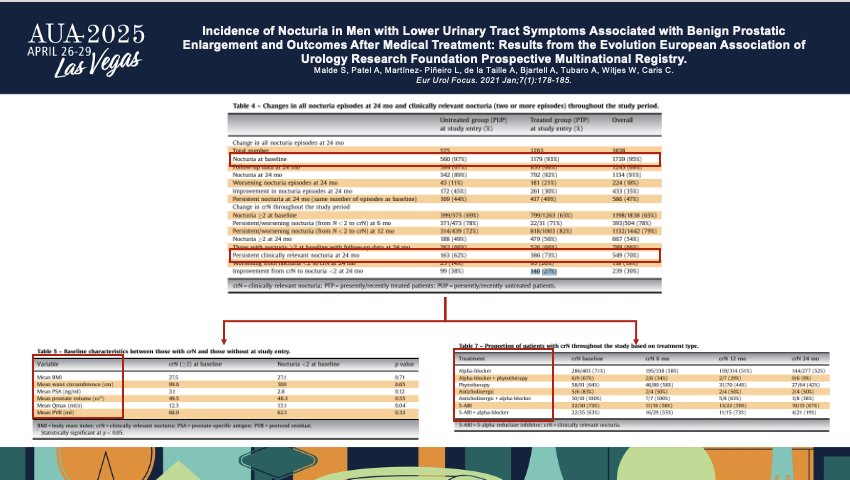
The audience was reminded that, according to AUA guidelines, we should target LUTS attributed to BPH AND give special attention to conditions like detrusor overactivity, underactivity, and nocturia. However what we foind in this recent review over adherence to the AUA guideline was that mong men submitted to idfferent surgical procedures, only 64% had their prostate size measured. Just over 50% had post-void residuals measured, and only one-third had uroflowmetry done. Between 60-80% were treated with alpha-blockers or 5-alpha reductase inhibitors. After surgery, 15-40% continued to have symptoms and remained on the same previous medications used to reduce the prostate volume and improve obstruction.
Dr. Truzzi urges “[that] it is time we asked ourselves: are we correctly treating our patients? Are we not overlooking key dysfunctions that could be causing their symptoms?”. Dr. Truzzi reinforces his point that we must look beyond the prostate. When prostate-targeted treatments fail to resolve symptoms, we must consider more than just a bad effect of the medication, failure of the technique, or the device used. In fact, long-term obstruction causes structural and functional changes to the bladder. In obstructed patients, bladder biopsies reveal increased Type I and Type II collagen, elevated vascular growth factors, higher muscarinic receptor levels, and few receptors involved in contraction.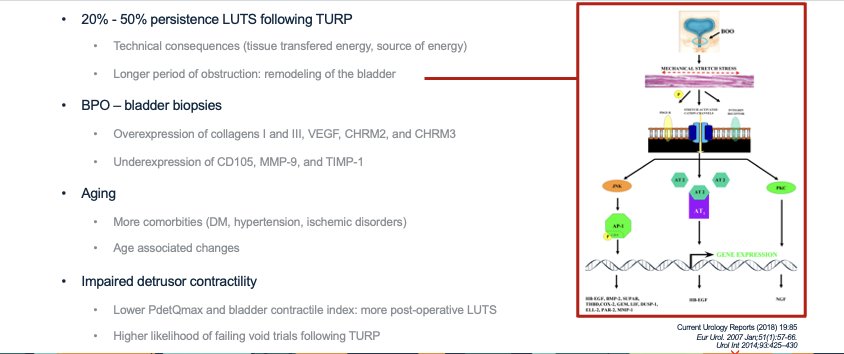
As a final point of reinforcement, Dr. Truzzi reminds us that male LUTS may or may not be caused by prostate obstruction, and that persistent symptoms after treatment don’t always mean a persistent prostate issue.
Presented by: José Carlos Truzzi, MD, MSc, PhD, Director of the Division of Female Urology, Pelvic floor and Urodynamics – Confederación Americana de Urología (CAU), Director Division of Infections – Sociedade Brasileira de Urologia (SBU), Escola Paulista de Medicina – Federal University of São Paulo (Brazil)
Written by: Eman N. Chaudhri, MD, Department of Urology, University of California, Irvine, @EmanChaudhri on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.