(UroToday.com) The American Urological Association (AUA) 2025 Annual Meeting, held in Las Vegas, NV, was host to an advanced prostate cancer podium session. Dr. Manish Patel presented the results of an exploratory analysis evaluating BMS-986365 (CC-94676), a dual androgen receptor ligand-directed degrader and antagonist, for heavily pre-treated patients with metastatic castration-resistant prostate cancer (mCRPC).
Androgen receptor pathway inhibitors (ARPIs) have been demonstrated to prolong overall survival in patients with mCRPC.1,2 However, ARPIs remain non-curative, and overcoming ARPI-resistant mCRPC has emerged as a key clinical challenge.
The majority of mCRPC likely remains androgen receptor (AR)-dependent, even if resistant to ARPIs.1,2 Potential mechanisms of AR reactivation include mutations in the AR ligand binding domains (LBDs)3 and over-expression of the wild-type (WT) receptor.4
A challenge in the development of AR degraders is identifying high-affinity AR binders that lack intrinsic agonism, which limits drug efficacy in the absence of complete receptor elimination. In this report, Dr. Patel presented data on BMS-986365 in patients with mCRPC, previously published in Annals of Oncology,5 as well as additional exploratory efficacy analyses by baseline patient characteristics.
BMS-986365 is an orally bioavailable, first-in-class, heterobifunctional molecule with a dual mechanism of action that degrades and competitively inhibits the AR. It contains an AR binding moiety that binds and antagonizes the AR LBD with low agonism potential, leading to competitive AR inhibition. It also contains a cereblon (CRBN)-binding moiety that facilitates targeted ubiquitination and subsequent proteosome system-mediated irreversible AR degradation. This agent has demonstrated pre-clinical and clinical activity in ARPI-resistant mCRPC models with WT AR and LBD mutations.6,7

In this phase I multicenter trial, mCRPC patients with disease progression on ≥1 APRI and taxane chemotherapy (or ineligible/declined) were enrolled. The study included a dose escalation (Part A) and expansion (Part B) of BMS-986365 up to 900 mg twice daily. The primary study objectives were to assess safety and tolerability, including defining the maximum tolerated dose (MTD) and/or recommended phase II dose. The key secondary endpoints were to evaluate efficacy outcomes, including:
- Decline in prostate-specific antigen ≥50% (PSA50)
- Radiographic progression-free survival (rPFS)
- Duration of response (DoR)
- Objective soft tissue response
- Pharmacokinetic characterization
The study design is illustrated below.
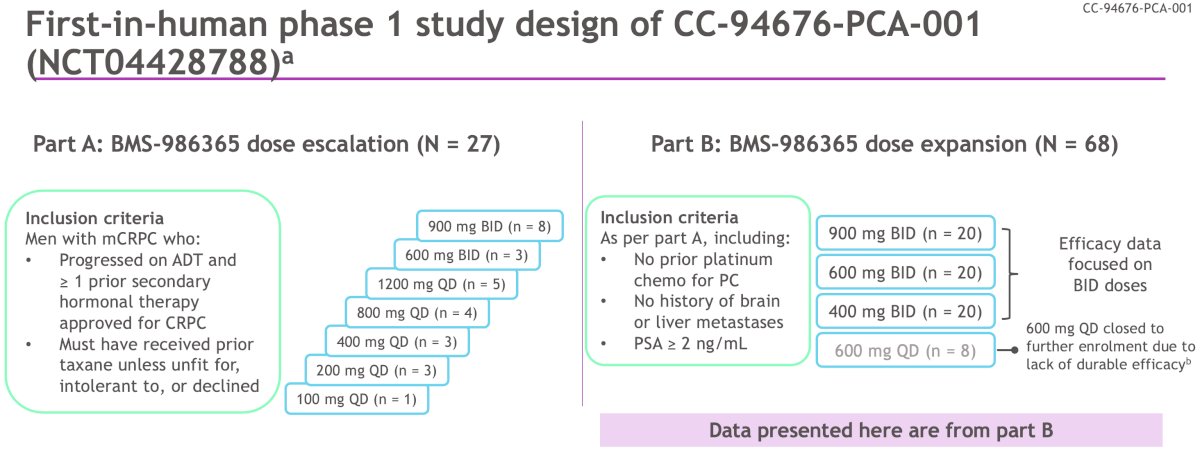
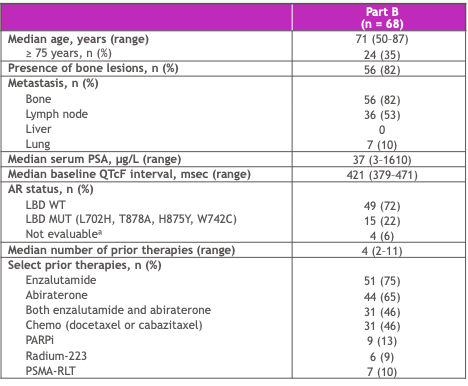
Data presented by Dr. Patel were from Part B, with a median study follow-up of 14.8 months (range: 9.6–24.3). Sixty-eight patients were included in Part B. The median age was 71 years. 82% of the patients had bone metastases, 10% had pulmonary metastases, and none had liver metastases. The median serum PSA was 37 ng/ml. AR LBD mutations were present in 22% of patients (72% AR LBD WT). The median number of prior therapies received was 4 (range: 2–11). Prior therapies received are summarized below.
In the Part A dose escalation cohort, the MTD was not reached. One drug-limiting toxicity of asymptomatic prolonged QTc interval was observed at a dose of 900 mg BID.
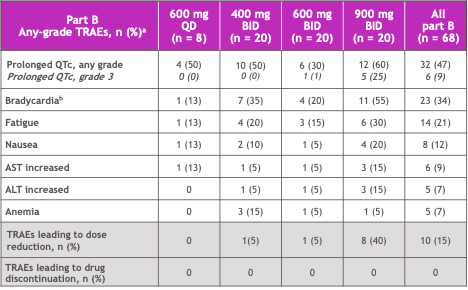
In the Part B dose expansion cohort, there were no grade 4–5 treatment-related adverse events (TRAEs). Grade 3 TRAEs occurred in 8 (12%) patients:
- 6 (9%) were asymptomatic prolonged QTc
- All grade 3 QTc events occurred within the first two cycles
Serious TRAEs occurred in 3 (4%) patients, all at 900 mg BID. Overall, TRAEs were manageable with dose modifications, and BMS-986365 was well-tolerated with a manageable safety profile.
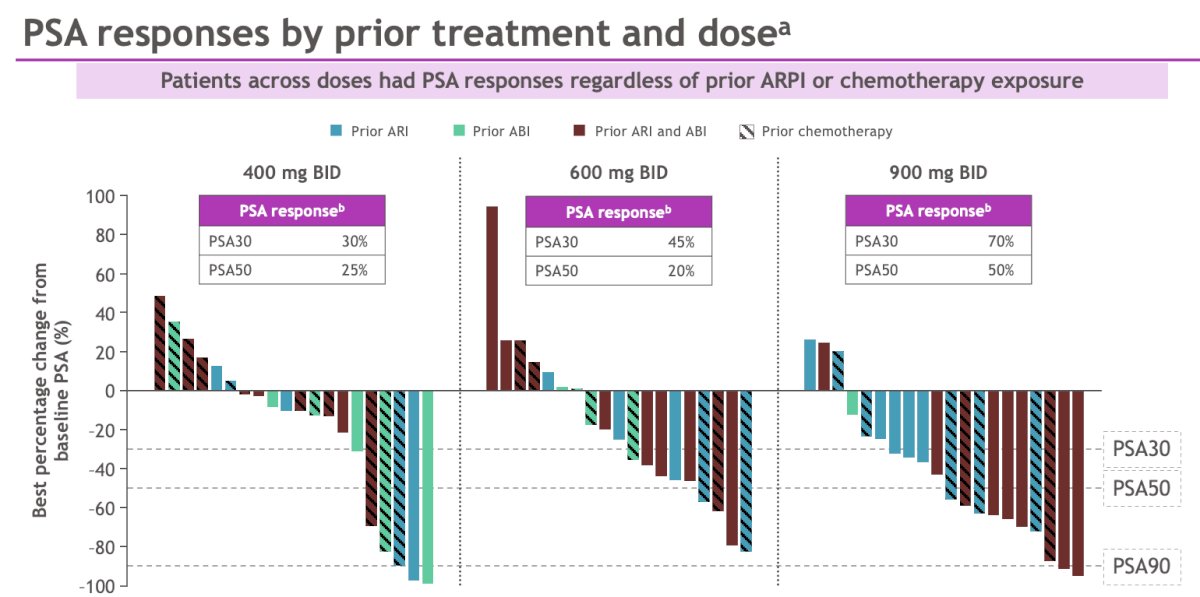
Patients across doses had PSA responses regardless of prior ARPI or chemotherapy exposure. The highest PSA30 and PSA50 responses were observed in the 900 mg BID-treated patients (70% and 50%, respectively).
A clinical benefit was evident in mCRPC patients regardless of AR LBD status, with numerically higher PSA30 and PSA50 responses in those with mutant LBDs.
Median rPFS was consistent across LBD WT and MUT mCRPC.
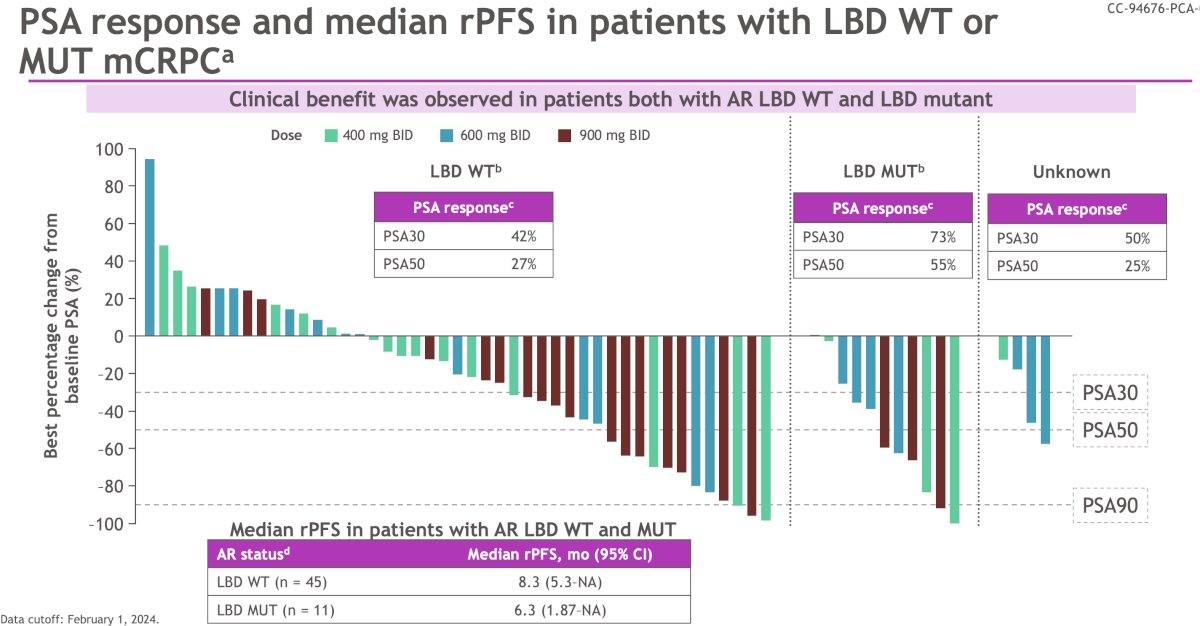
Among the patients in part B treated with twice daily regimens, the overall median rPFS (n=60) was 6.3 months (95% CI: 5.3–10.5) and highest in the 900 mg BID group, with a median of 8.3 months. Overall, 42% (n = 25) of patients were free of radiographic progression or death at 6 months. Post-hoc analyses of rPFS stratified by age, prior chemotherapy use, and opioid use at baseline were performed. When stratified by age (≤70 versus >70 years), no significant differences were observed.

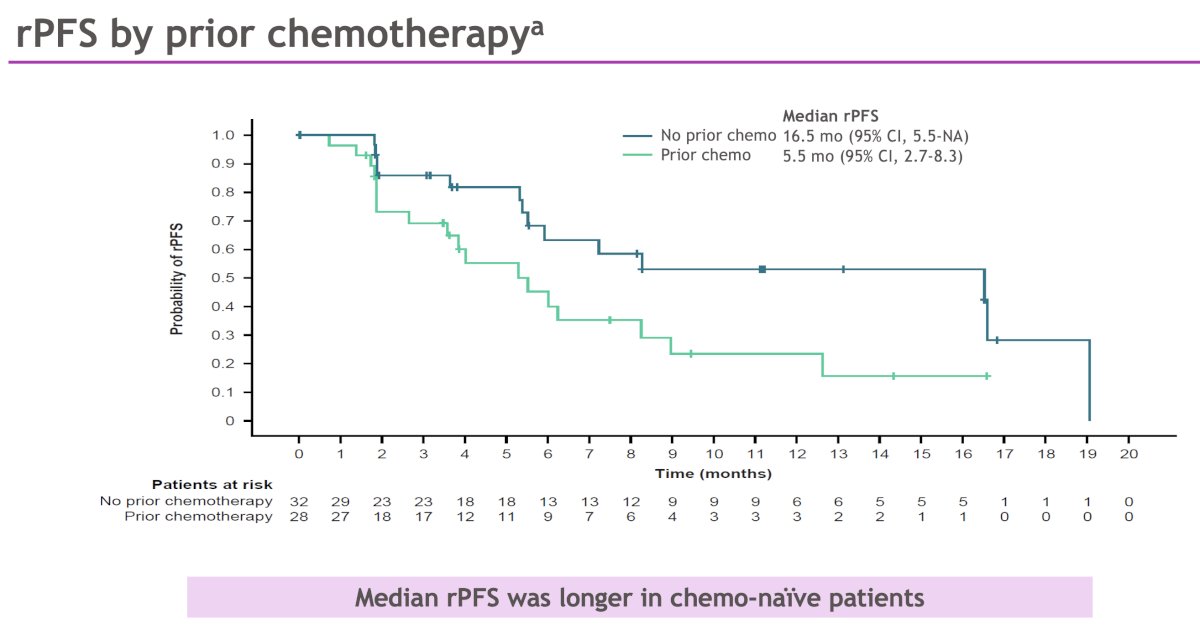
When stratified by prior chemotherapy, the study investigators observed that the median rPFS was longer in chemo-naïve patients (median: 16.5 versus 5.5 months).
Median rPFS was longer for patients not taking opioids at baseline (12.6 versus 5.4 months).

Based on these results, Dr. Patel concluded as follows:
- BMS-986365 is an orally bioavailable, first-in-class dual AR degrader and antagonist with the potential to overcome ARPI resistance in mCRPC, regardless of AR LBD mutational status
- BMS-986365 was well-tolerated with a manageable safety profile
- QTc prolongation was the most common TRAE; grade 3 events occurred during the first 2 cycles (n = 6), and all were asymptomatic and resolved with dose modification
- The MTD was not reached, and dose optimization is ongoing
- BMS-986365 demonstrated anti-tumor activity in heavily pretreated patients with mCRPC, all with prior ARPI exposure (with nearly 50% receiving 2 prior ARPIs)
- Dose-dependent PSA responses were observed with higher PSA30 at higher doses
- A clinical benefit was seen in both patients with AR LBD WT and AR LBD MUT mCRPC
- The median rPFS was longer in chemo-naïve patients compared to chemo-exposed patients, and longer for patients not taking opioids at baseline
- A pivotal phase III study of BMS-986365 in patients with mCRPC is underway (rechARge, NCT06764485)
Presented by: Manish R. Patel, MD, Medical Oncologist/Hematologist Director of Drug Development at Florida Cancer Specialists & Research Institute/Associate Director of Drug Development at Sarah Cannon Research Institute, Sarasota, FL
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: BMS-986365: Targeting AR Degradation and Antagonism in Metastatic Prostate Cancer - Manish Patel
References:
- Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013; 368(2): 138-148.
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014; 371(5): 424-433.
- Antonarakis ES, Zhang N, Saha J, et al. Prevalence and Spectrum of AR Ligand-Binding Domain Mutations Detected in Circulating-Tumor DNA Across Disease States in Men With Metastatic Castration-Resistant Prostate Cancer. JCO Precis Oncol. 2024; e2300330.
- Abida W, Cyrta J, Heller G, et al. Genomic correlates of clinical outcome in advanced prostate cancer. Proc Natl Acad Sci U S A. 2019; 116(23): 11428-11436.
- Rathkopf DE, Patel MR, Choudhury AD, et al. Safety and clinical activity of BMS-986365 (CC-94676), a dual androgen receptor ligand-directed degrader and antagonist, in heavily pretreated patients with metastatic castration-resistant prostate cancer. Ann Oncol. 2025; 36(1): 76-88.
- Xu S, et al. Oral presentation at the American Association for Cancer Research Annual Meeting; April 5–10, 2024; San Diego, CA.
- Rathkopf D, et al. Poster presentation at the ASCO Genitourinary Cancers Symposium; January 25–27, 2024; San Francisco, CA. Abstract 134. Cancer.