(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, Nevada, was host to the Plenary Session on Saturday 26th of April. Drs. Lara Rodriguez Sanchez, Samir Taneja, Hashim Ahmed, Himanshu Nagar, Edward Schaeffer in a Crossfire: Controversies in Urology debate: discussed if Focal Therapy is a Suitable Option for all Cases with Intermediate-Risk Prostate Cancer.
Dr. Taneja began his presentation by highlighting the AUA Guidelines on the management of localized prostate cancer. He emphasized that clinicians should inform patients with intermediate-risk prostate cancer who are considering whole-gland or focal ablation that there is currently a lack of high-quality data comparing ablation outcomes to those of radiation therapy, surgery, and active surveillance. Furthermore, clinicians should not recommend whole-gland or focal ablation for patients with high-risk prostate cancer outside of a clinical trial setting.
He then moved on to present a clinical case involving a 72-year-old man who presented in early 2018 with an elevated PSA of 12.01 ng/mL. His SHIM score was 17, and his IPSS score was 8. His past medical history was notable for atrial fibrillation, for which he was on apixaban, and hypothyroidism; he had no history of prior surgery. MRI revealed a prostate volume of 37 grams with a 2.1 cm region of suspicion located in the left anterior transition zone, categorized as PI-RADS 3. There was no evidence of extraprostatic extension, seminal vesicle invasion, or lymphadenopathy. Biopsy results confirmed a Gleason score of 3+4 (Grade Group 2) prostate cancer.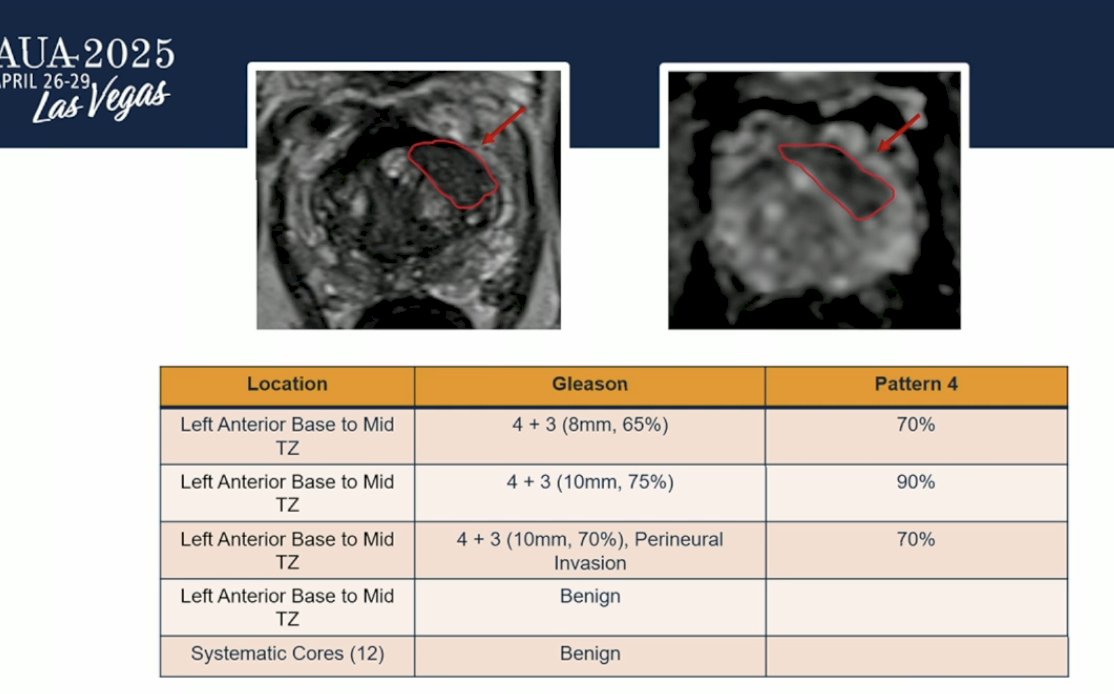
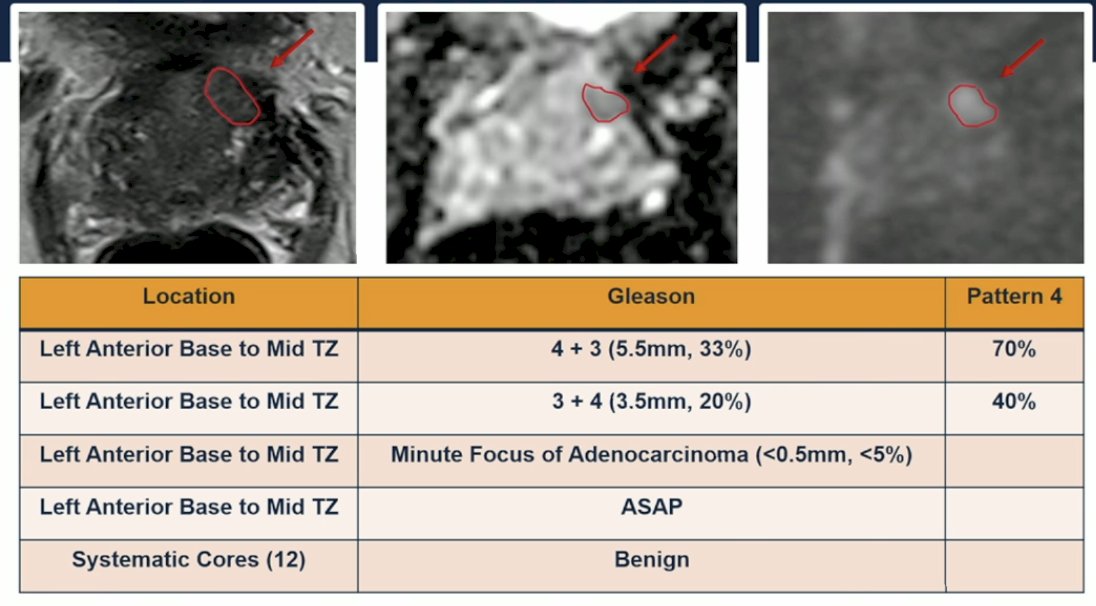
The patient underwent focal cryoablation in 2018. Over the following years, PSA levels remained stable, although in early 2024, there was a slight PSA increase. Despite this, MRI imaging and follow-up biopsies showed no evidence of suspicion or recurrence at that time. However, in November 2024, a new abnormality was identified on MRI: a 9 × 7 mm lesion located in the left anterior base of the transition zone, suspicious for recurrence. Importantly, there was no evidence of extraprostatic extension or lymphadenopathy. The biopsy results and MRI images corresponding to this new finding are shown below.
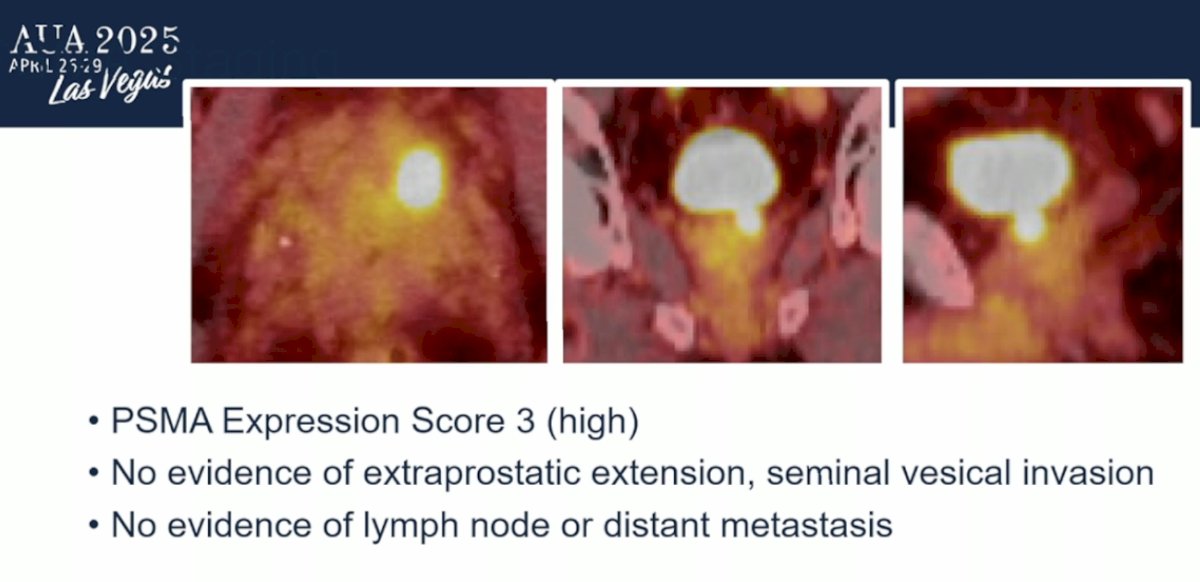
Further evaluation with PSMA PET imaging revealed a PSMA expression score of 3, indicating high uptake at the site of concern. Importantly, there was no evidence of extraprostatic extension, seminal vesicle invasion, lymph node involvement, or distant metastasis.
Dr. Taneja then engaged the audience by posing several important questions about the case. He asked whether this patient would still be considered an appropriate candidate for focal therapy at this stage. He challenged the audience to consider whether the initial favorable outcomes years of disease control with preserved quality of life should be viewed as treatment success. He also questioned whether a delayed local recurrence, several years after the initial focal therapy, should truly be considered a treatment failure.?
Dr. Edward Schaeffer began his presentation by emphasizing that focal therapy is not suitable for all patients with intermediate-risk prostate cancer. For some, focal therapy may represent too much treatment; for others, it may be just right; and for certain patients, it may not be enough. He outlined key factors that must be considered when assessing the suitability and need for treatment in patients with intermediate-risk disease. These include the volume of disease, its biological aggressiveness, the specific type of intermediate-risk prostate cancer, and the patient's overall life expectancy.
Dr. Schaeffer noted that an increasing proportion of prostate cancer cases are now classified as intermediate risk, largely due to advances in diagnostic testing that have refined which patients undergo biopsy. He referenced key data from the PRECISION trial, the PROTECT study, and the OPTIMUM study, all of which highlight these evolving patterns.1,2
He emphasized the phenomenon of grade migration, noting that diagnostic criteria have shifted significantly over time. Following the 2014 ISUP consensus, there has been increased attention to the diagnosis of Gleason pattern 4, particularly with greater recognition of cribriform glands and poorly formed glands. As a result, there has been a significant reduction, approximately 80% in the number of Grade Group 1 cases identified on prostate biopsy. This reclassification reflects a stricter interpretation of biopsy findings, contributing to the growing number of patients categorized as intermediate risk.
Dr. Schaeffer discussed the implications of the increasing migration toward intermediate-risk prostate cancer. He proposed that, just as there has been a migration in diagnosis, perhaps a migration in management strategies is also warranted. Specifically, he suggested that the outstanding historical outcomes observed in men with low-volume, Grade Group 1 prostate cancer may now also apply to certain cases of contemporarily diagnosed low-volume Grade Group 2 disease.
Identifying which cases fall into this favorable category is crucial. The ISUP 2014 recommendations offer valuable guidance in this regard, emphasizing the importance of a precise description of the type and amount of Gleason pattern 4 seen on biopsy. Particular attention should be paid to the presence of cribriform architecture and intraductal carcinoma, as well as the exact measurement in millimeters of pattern 4 cancer identified. This detailed pathological characterization can help clinicians better stratify risk and tailor management approaches appropriate.
Dr. Schaeffer continued by addressing what is known about the amount of pattern 4 disease in Grade Group 2 (GG2) biopsies. He highlighted that low linear amounts of pattern 4 cancer on biopsy are associated with outcomes similar to those seen in pure pattern 3 (Grade Group 1) cancers. In particular, studies have shown that when only 2 mm of pattern 4 is present, there is only about a 2% difference in the risk of biochemical recurrence (BCR) between low-grade and intermediate-grade disease.
These findings suggest that for select patients with minimal pattern 4 involvement, immediate treatment may not be necessary. Instead, active surveillance could be a reasonable and safe approach, similar to strategies used for patients with low-risk prostate cancer.
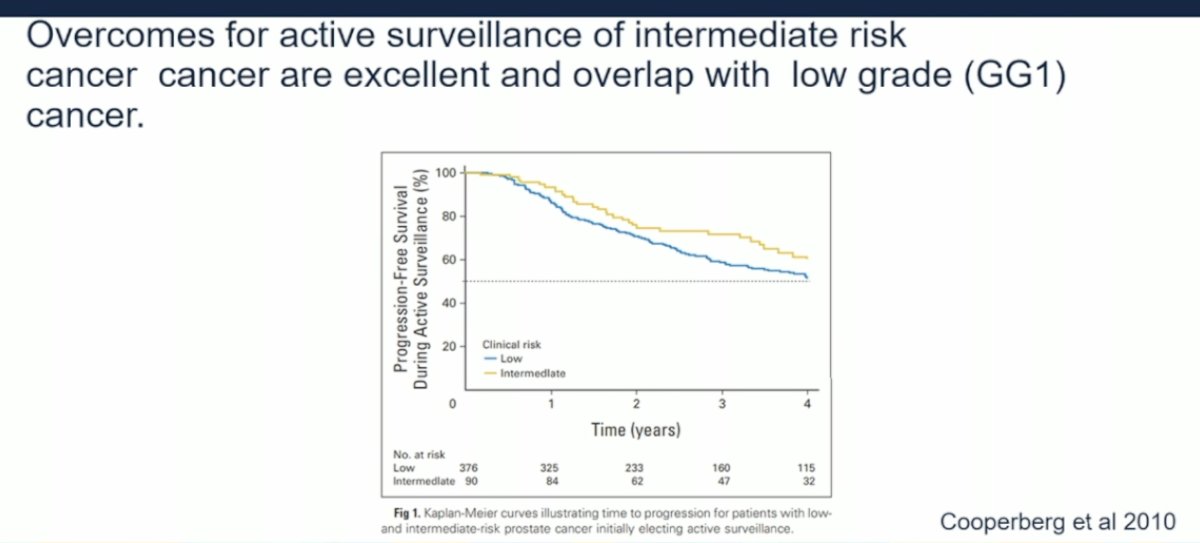
Dr. Schaeffer acknowledged that pioneers like Dr. Matt Cooperberg and Dr. Peter Carroll were among the first to advocate for active surveillance (AS) in carefully selected patients with intermediate-risk prostate cancer. Their work demonstrated that outcomes for active surveillance in intermediate-risk disease are excellent and, in many cases, overlap with the outcomes traditionally seen in low-risk (Grade Group 1) prostate cancer. As shown below.
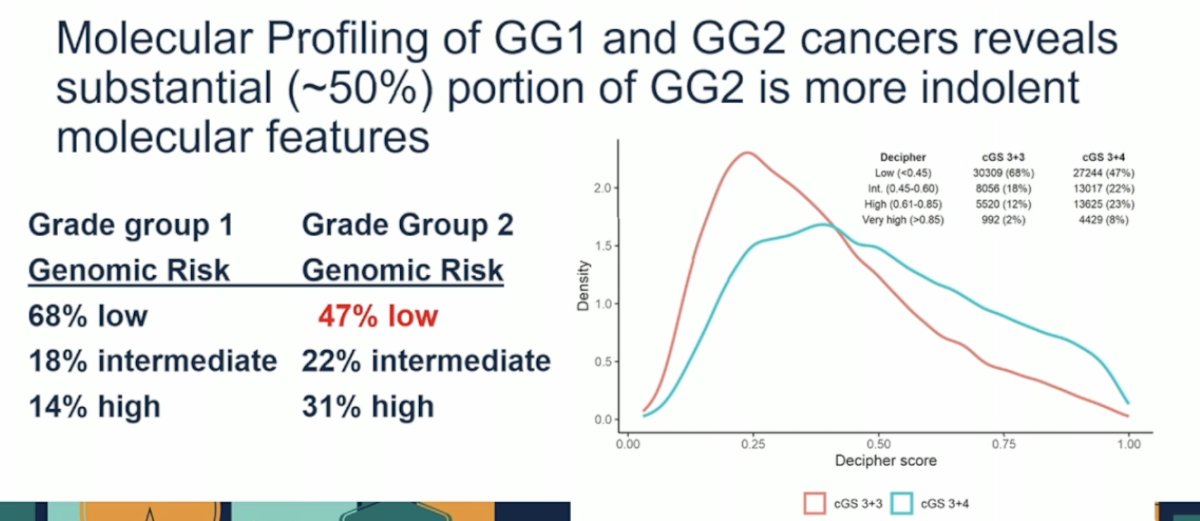
Dr. Schaeffer explained that more granular patient selection can be achieved by assessing the presence or absence of intraductal carcinoma (IDC) and cribriform (Crib) patterns, as their absence suggests a less aggressive pattern 4 phenotype. He also noted that molecular profiling studies show that about 50% of GG2 cancers share indolent features similar to GG1, supporting surveillance in selected patients.
The type of intermediate-risk prostate cancer is often determined by PSA, DRE, and Gleason score. Notably, it is now recognized that intermediate-risk disease defined by PSA alone has favorable outcomes with surveillance. In fact, metastasis-free survival at 15 years was identical 94% for men with GG1 prostate cancer whether their PSA was <10 ng/mL or between 10–20 ng/mL.
Life expectancy is also a critical factor when considering focal therapy. For patients with limited life expectancy, focal therapy may represent overtreatment. Although current guidelines recommend deferring treatment in this population, there is an increasing trend toward treating even men with intermediate-risk prostate cancer, despite the limited expected benefit.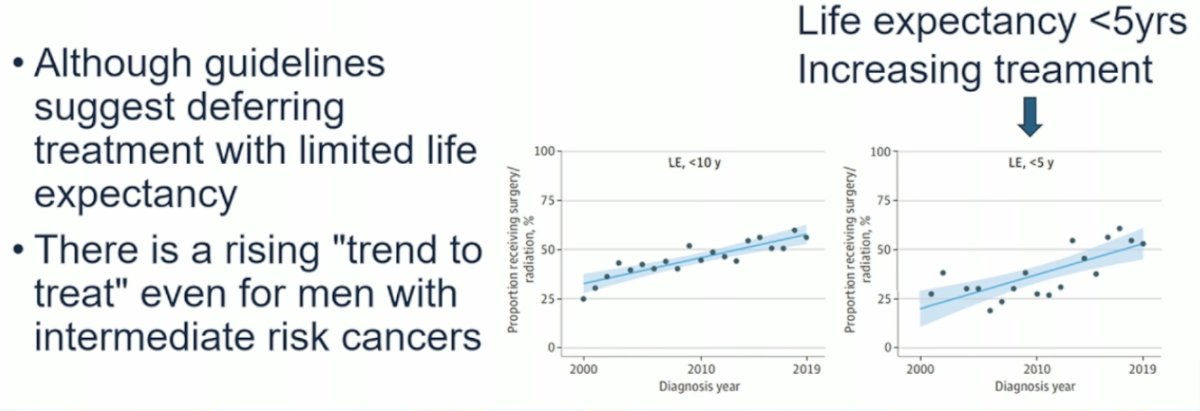
Dr. Schaeffer concluded with the following key points:
- Treatment should be deployed when a cure is truly needed.
- Features suggesting active treatment can be deferred, and focal therapy may not be appropriate:
- Minimal pattern 4 disease (measured by length or percentage)
- Absence of adverse histologic features (cribriform or intraductal carcinoma)
- Low genomic risk profiles
- Intermediate-risk disease defined by PSA elevation only
- Limited patient life expectancy
Dr. Rodriguez began her discussion by highlighting a recent systematic review and meta-analysis of prospective studies published just a few months ago. She noted that the use of focal therapy (FT) has doubled in recent years. The analysis demonstrated that FT offers meaningful effectiveness in ablating prostate cancer and eradicating clinically significant lesions, particularly in carefully selected patients with predominantly intermediate-risk prostate cancer.3
Dr. Rodriguez then addressed the definition of intermediate-risk prostate cancer, noting that it is not equivalent to Gleason score 7 as it was traditionally thought of prior to the 2014 ISUP update. Under the current system, intermediate-risk disease includes patients with Grade Group 2 or 3, clinical stage T2b to T2c, or a PSA level between 10 and 20 ng/mL. She emphasized that many patients treated with focal therapy for so-called "low-risk" disease before 2014 would now, under the updated ISUP classification, be categorized as Grade Group 2 or 3, reflecting a more refined understanding of disease risk.
The FALCON consensus, provides updated guidance for the use of FT in prostate cancer. Notably, the FALCON consensus recommends that FT should be offered to patients with localized ISUP grade 2 prostate cancer (with more than 10% pattern 4) and to patients with localized ISUP grade 3 prostate cancer.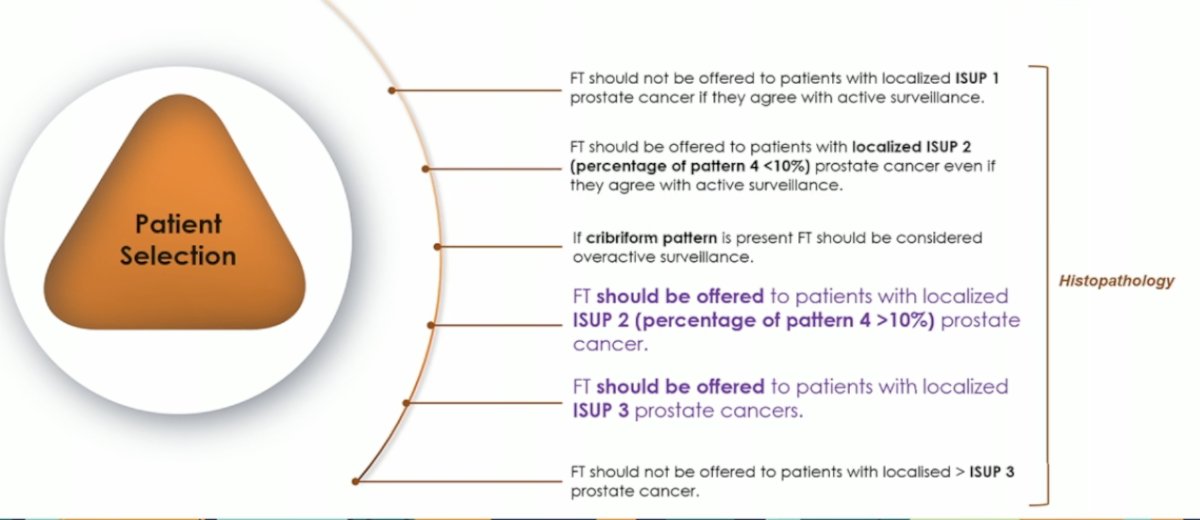
Furthermore, Clinical staging has significantly improved with the use of MRI, which is not surprising. In a study of 1,683 patients undergoing both DRE and MRI, with 552 undergoing RARP, mpMRI more accurately identified stage ≥3a prostate cancer compared to DRE (67% vs 58%). This advanced imaging techniques could help to better select candidates for FT.4
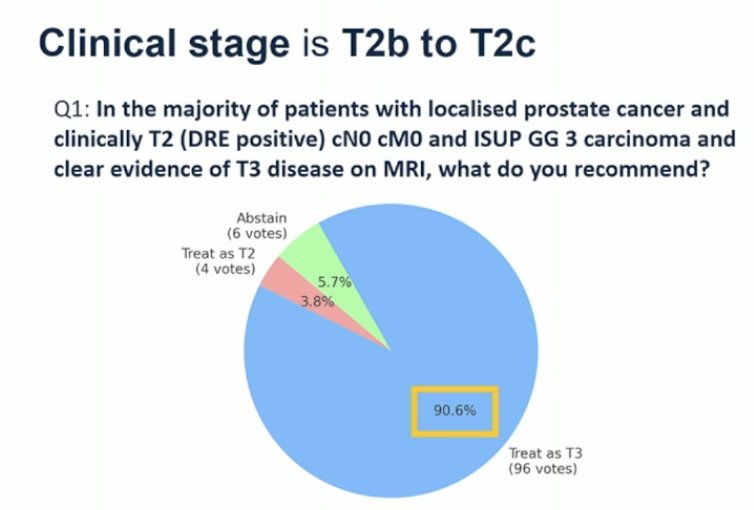
The panel of experts at the APCCC last year, recommend that if a patient has localized prostate cancer with clinical stage T2b–T2c based on DRE, no clinical evidence of nodal (cN0) or distant metastases (cM0), ISUP Grade Group 3 disease, and clear evidence of T3 disease on MRI, the patient should be treated as T3, as shown below. This reflects how MRI is now being used more often than DRE for clinical staging.
Many patients classified as intermediate-risk by PSA alone may actually fall into the low-risk category when PSA density (PSAD) is taken into account, making them candidates for focal therapy. PSA levels between 10 and 20 ng/mL are characteristic of intermediate-risk prostate cancer; however, beyond the absolute PSA value, PSAD significantly improves diagnostic accuracy and may serve as an independent predictor of oncologic outcomes after treatment. According to the AUA guidelines, PSAD is recognized as an important component of clinical assessment.
Moreover, in focal therapy, PSAD plays a critical role. In a study of 632 patients with clinically significant prostate cancer (CSPCa) treated with cryotherapy, multivariable analysis showed that only PSAD remained statistically significant in predicting disease-free progression, whereas PSA alone did not.5
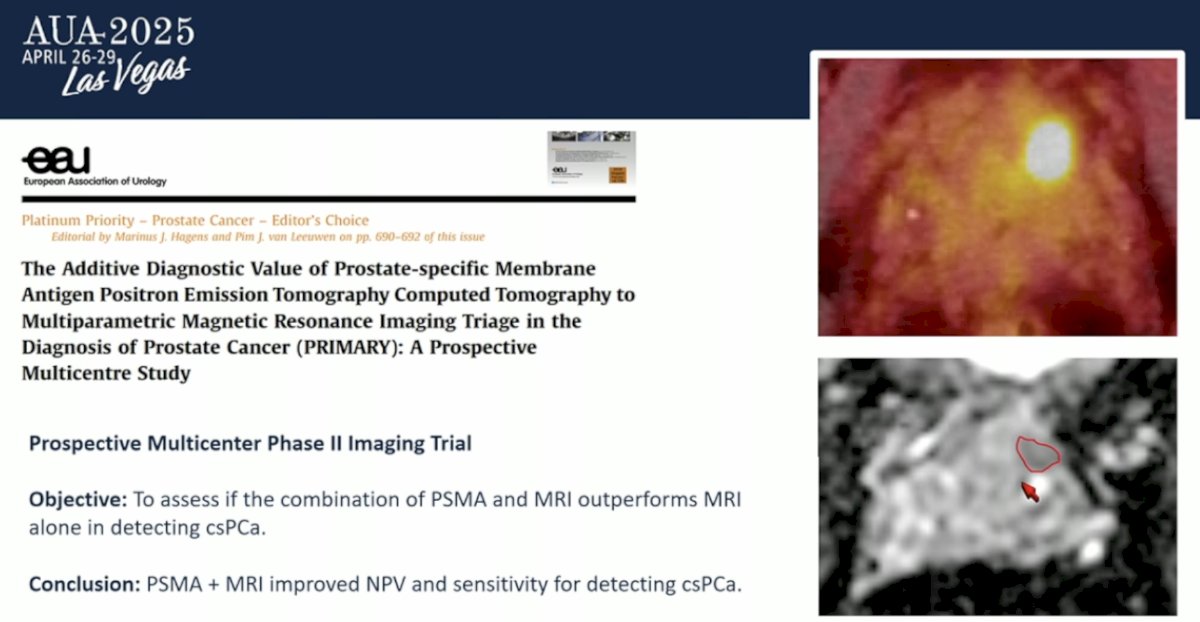
The field is moving forward with the introduction of PSMA PET imaging. Thanks to the PRIMARY prospective study, a multicenter Phase II imaging trial—the combination of PSMA PET and MRI was shown to outperform MRI alone in detecting clinically significant prostate cancer (csPCa). The study concluded that PSMA PET plus MRI improved both the negative predictive value and sensitivity for detecting csPCa. Beyond local staging, PSMA PET also allows us to identify patients with metastatic disease outside the pelvis.6
In a retrospective study of 396 men diagnosed with unfavorable intermediate-risk prostate cancer, PSMA PET/CT was used as the primary staging method. It detected metastatic disease in 9.3% of patients (37 of 396), including distant metastases in 4% and locoregional nodal metastases in 7.3%.
Dr. Rodriguez concluded her presentation with the following key takeaways:
- Recent advances in MRI, pathology, and PSMA PET have significantly shifted how we classify prostate cancer risk.
- As diagnostic tools continue to improve, our ability to accurately select candidates for focal therapy—and expand selection criteria—has also improved.
- In 2025, even patients with unfavorable intermediate-risk prostate cancer may be considered appropriate candidates for focal therapy under certain conditions.
Dr. Nagar began by highlighting the "Goldilocks Principle" and applying it to intermediate-risk prostate cancer and focal therapy, illustrating how treatment could be “too cold,” “too hot,” or “just right.”
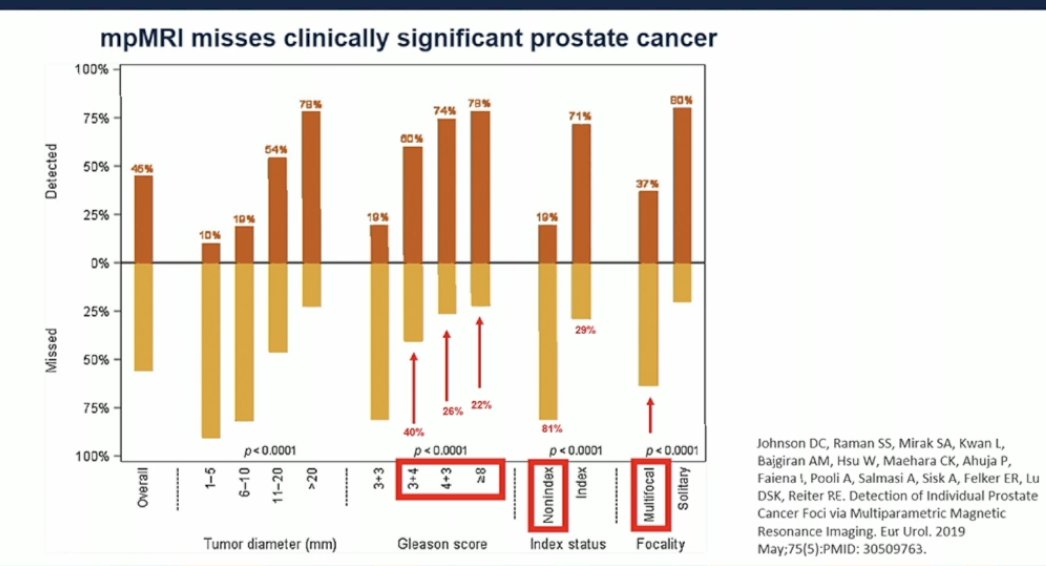
The applicability of focal therapy depends on the "clinical significance" of the prostate cancer, including factors such as multifocality, tumor volume, and biological aggressiveness. Data suggest that suboptimal patient selection remains a challenge. Often, we observe that mpMRI misses clinically significant prostate cancer when compared to radical prostatectomy surgical pathology, leading to disease upgrading at the time of surgery.
However, we may be able to overcome this pitfall by offering targeted biopsies. In a study assessing the impact of MRI targeting on pathologic upgrading and downgrading at prostatectomy, MRI-targeted biopsy resulted in lower rates of upgrading compared to systematic biopsy alone (27% vs. 42%).7
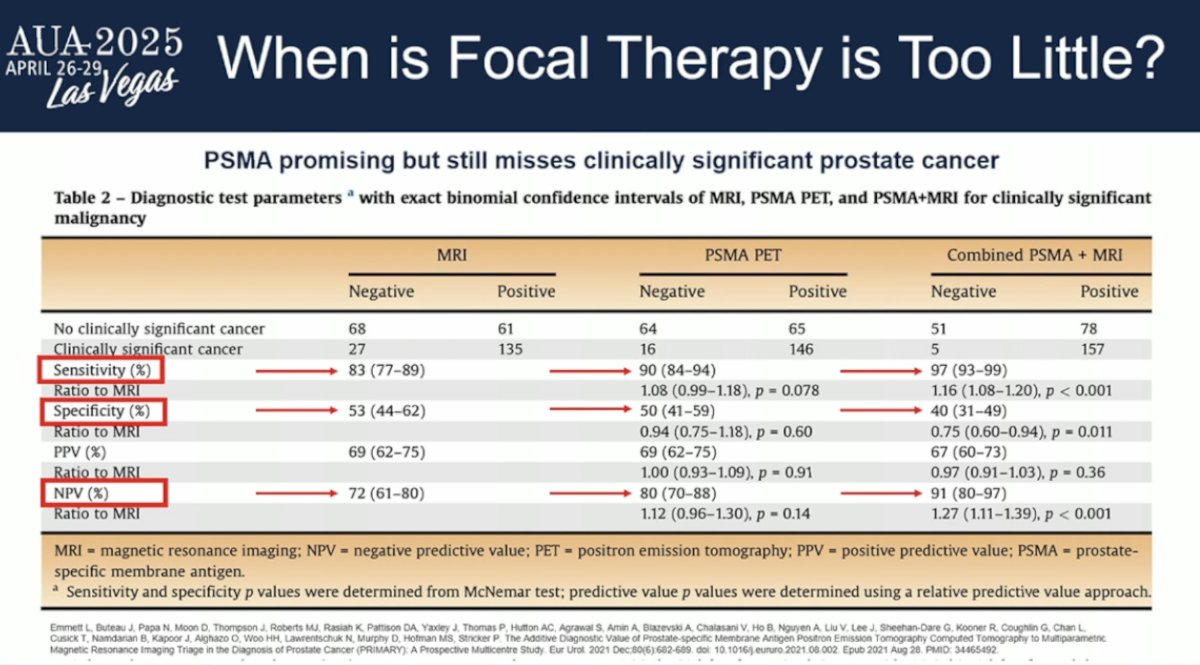
While PSMA PET is promising, it still misses some cases of clinically significant prostate cancer and is not yet perfect for identifying all patients who would benefit from focal therapy. In studies, the sensitivity of PSMA PET for detecting CSPC was 90%; however, the specificity was only 50%.
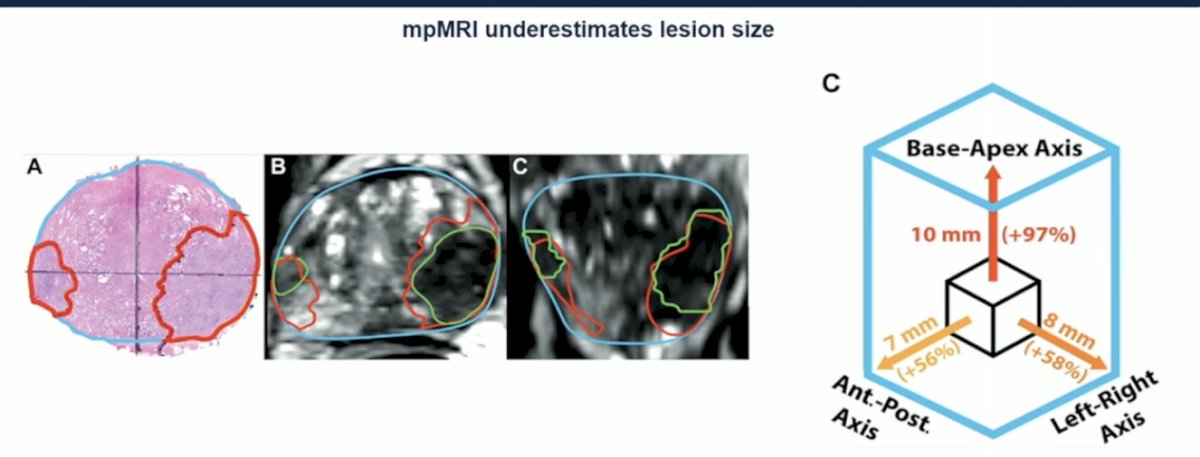
Moreover, MRI tends to underestimate the size of the target lesion, raising concerns about missing part of the treatment area and questioning what margin should be applied during focal therapy. From an imaging standpoint, we are still not fully there in accurately identifying ideal candidates for focal therapy.
Genomic testing has revealed that intermediate- and high-risk prostate cancers often share overlapping biological profiles. This highlights the wide biological spectrum within these risk groups. As shown below, the variability in genomic features underscores the complexity of accurately predicting disease behavior based solely on traditional clinical parameters.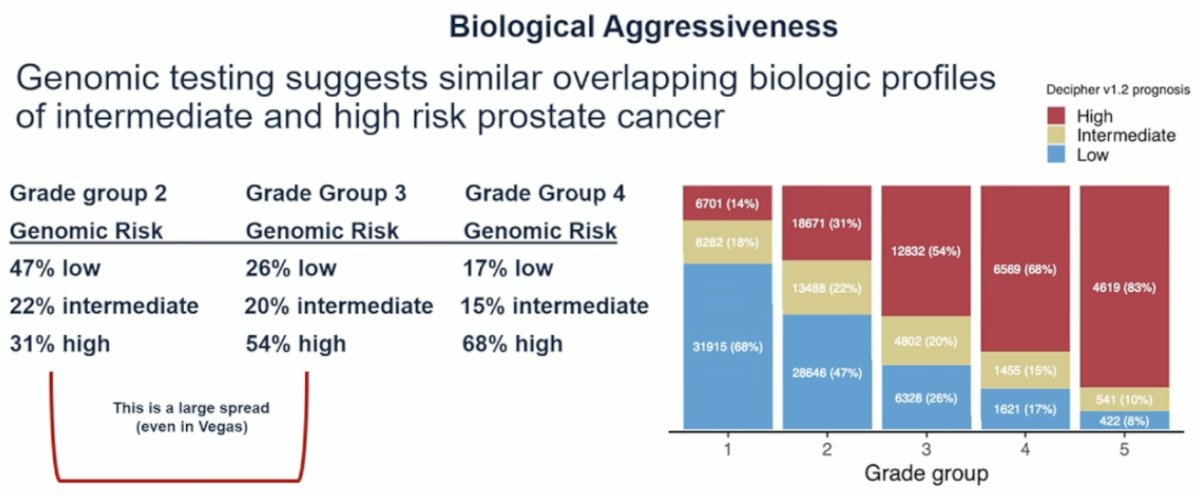
Dr. Nagar highlighted the issue of suboptimal patient selection in focal therapy, referencing a meta-analysis where 19 of 50 included studies focused predominantly on intermediate-risk patients (n = 2800). In the overall cohort, the estimated 12- and 24-month csPCa recurrence-free survival (RFS) rates were 86% (95% CI: 82–89%) and 81% (95% CI: 74–86%), respectively. Within the intermediate-risk subgroup, the 12-month csPCa RFS rate was lower at 79% (95% CI: 74–83%). Dr. Nagar noted that the median follow-up of 21 months and the reliance on surrogate endpoints were major limitations of the available data.8
Moreover, in a systematic review and meta-analysis, biochemical progression was reported in 15 of 49 cohorts (30.6%). Among these, 80% used the Phoenix criteria, 13.3% used the ASTRO criteria, and 6.7% applied a nadir + 0.5 ng/mL definition. The average biochemical progression rate per year was 9.3% (95% CI: 7.0–12.3; I² = 63%; p < 0.01). The rate of any cancer-positive biopsy following focal therapy was 44.6% (95% CI: 38.7–50.6%). The treatment failure rate—including radical treatment, whole-gland ablation, hormonal therapy, or transition to watchful waiting was 14.1% per year.
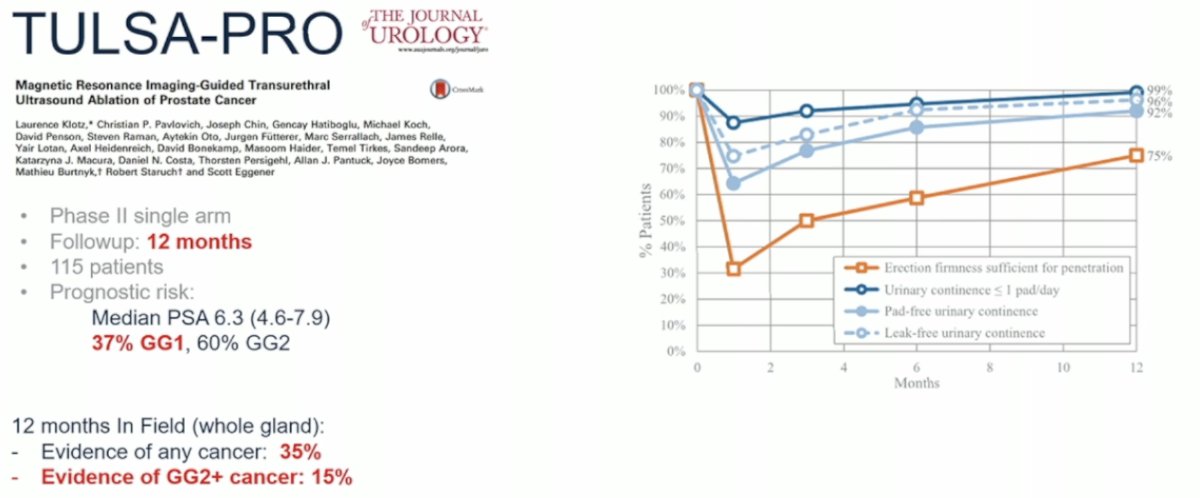
Dr. Nagar briefly discussed the TULSA-PRO trial, a Phase II single-arm study with a 12-month follow-up. A total of 115 patients were enrolled, with a median PSA of 6.3 ng/mL; 37% had Grade Group 1 disease and 60% had Grade Group 2 disease. At 12 months, within the in-field treatment area, evidence of any cancer was found in 35% of patients, and evidence of Grade Group 2 or higher cancer was found in 15%. However, while urinary continence and erectile function initially declined following treatment, both recovered to near-baseline levels by one year.9
In terms of MRI-guided high-intensity focused ultrasound (HIFU), one of the landmark studies is a Phase II single-arm trial with a 24-month follow-up. Of 194 patients assessed, 101 were treated, primarily with intermediate-risk disease; the median PSA was 5.7 ng/mL (range 4.2–7.5), and 78% had Grade Group 2 disease. At 24 months, within the targeted area, evidence of any cancer was found in 20% of patients, and evidence of Grade Group 2 or higher cancer was found in 9%, with 55.6% of these being Grade Group 3 or higher. When assessing the entire prostate, evidence of any cancer was found in 60% of patients and evidence of Grade Group 2 or higher cancer in 40%. Notably, 40% of patients developed erectile dysfunction by two years.10
Dr. Nagar concluded that if we apply the Goldilocks Principle, we are still "too cold" when it comes to focal therapy in this disease space. While focal therapy works in approximately 60% of cases, it is not yet consistently reliable across all patients with intermediate risk prostate cancer.
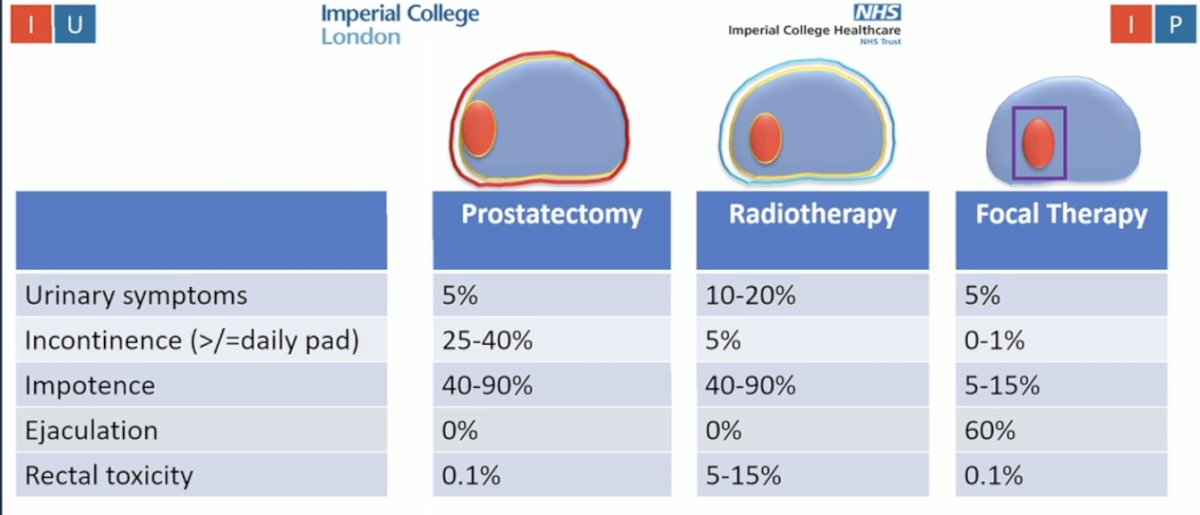
Focal Therapy a suitable option for all cases of Intermediate risk prostate cancer: YesDr. Ahmed discussed how we invest significant energy, time, effort, and resources into identifying the index lesion, only to often discard that precision by treating the entire prostate. He emphasized that functional outcomes are overwhelmingly better with focal therapy, noting a 5- to 10-fold improvement in urinary symptoms and rates of impotence, as illustrated below.
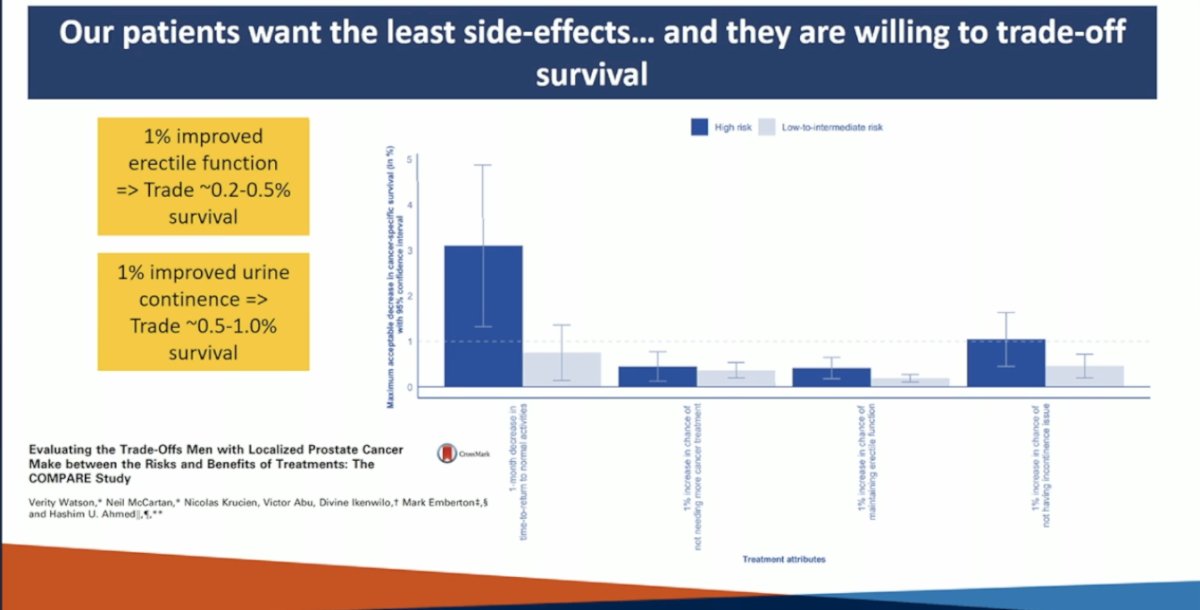
It is no secret that our patients want the least possible side effects and they are willing to trade off some degree of survival for improvements in quality of life. Data suggest that patients would trade approximately 0.2–0.5% survival for a 1% improvement in erectile function, and about 0.5–1.0% survival for a 1% improvement in urinary continence. However, the key message is that with focal therapy, they may not need to make that trade-off.
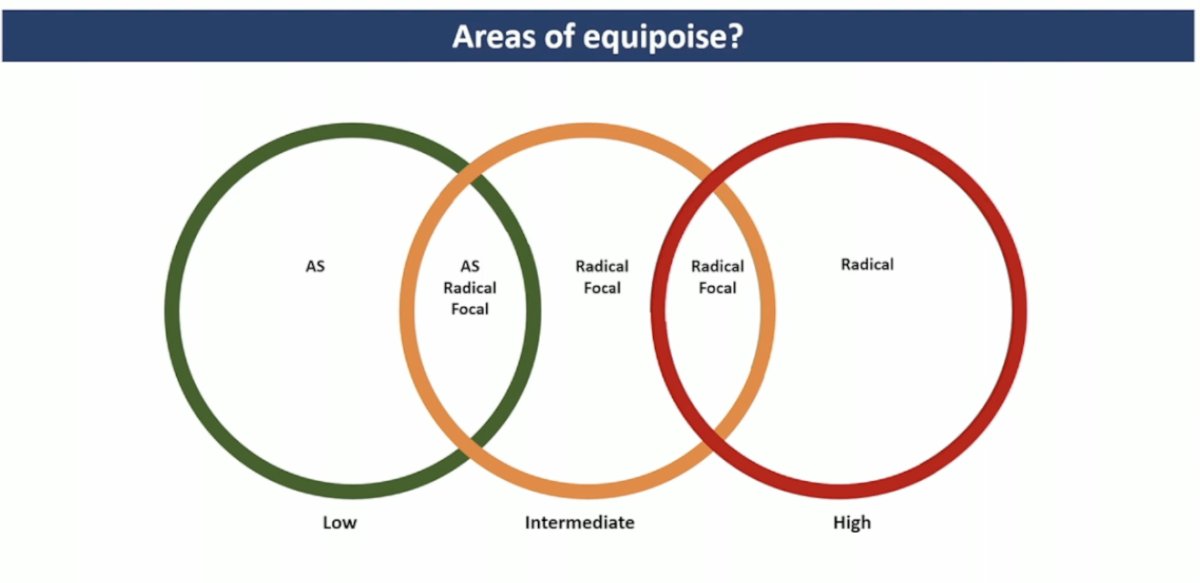
In intermediate-risk prostate cancer, there is the greatest area of equipoise, with significant overlap among treatment options ranging from active surveillance to focal therapy and radical treatment.
Focal therapy is being held to a higher standard than radical therapy has been over the past few decades. It is important to understand that focal therapy is not an alternative to active surveillance in low-risk prostate cancer. Dr. Ahmed highlighted the importance of developing and maintaining dedicated registries across different focal therapy modalities to better understand outcomes and guide patient selection.
In the U.K., a very pragmatic approach has been adopted for patient selection for focal therapy. Clinically, candidates include those with a PSA ≤20 ng/mL, radiological staging of T3aN0M0, and a lesion confined to no more than one quadrant on MRI. From a histological standpoint, patients with Gleason 7 disease (either 3+4 or 4+3) are eligible, and maximal Gleason 4+4 disease on targeted biopsies may be permitted provided the primary lesion is Gleason 7. There is no cancer length limit for Gleason 7 lesions. For patients with Gleason 3+3=6 disease, eligibility requires a core length of ≥6 mm associated with an MRI-visible lesion scored 3, 4, or 5, while untreated non-visible disease (MRI scores 1, 2, or 3) may be left under surveillance. Additionally, up to 5 mm of Gleason 3+3 disease or up to 2 mm of Gleason 3+4 with <10% pattern 4 is permitted, with these patients being placed on active surveillance.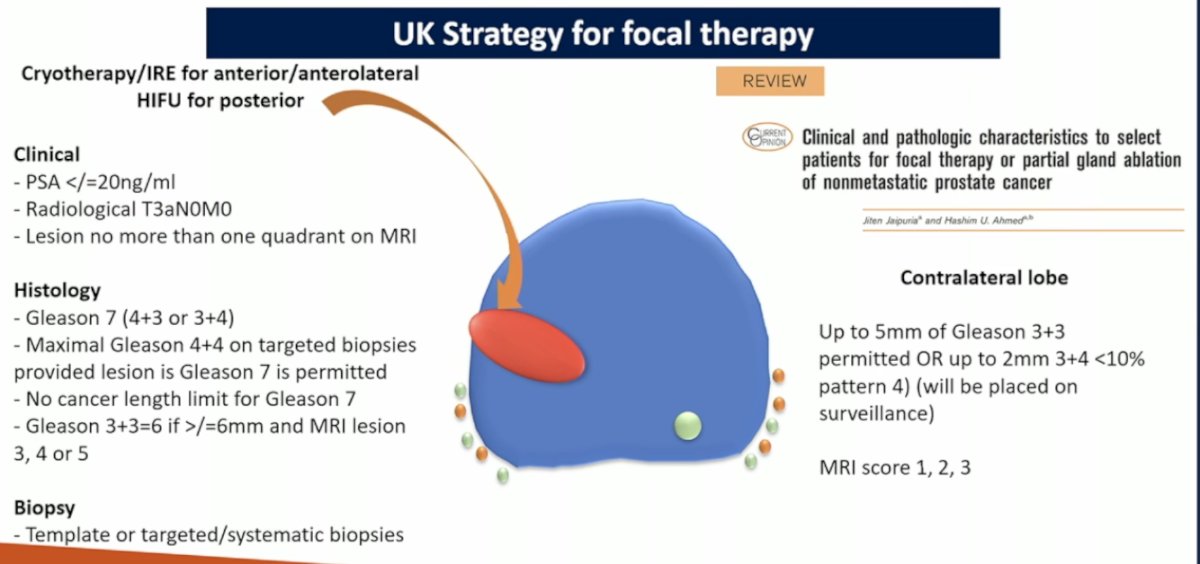
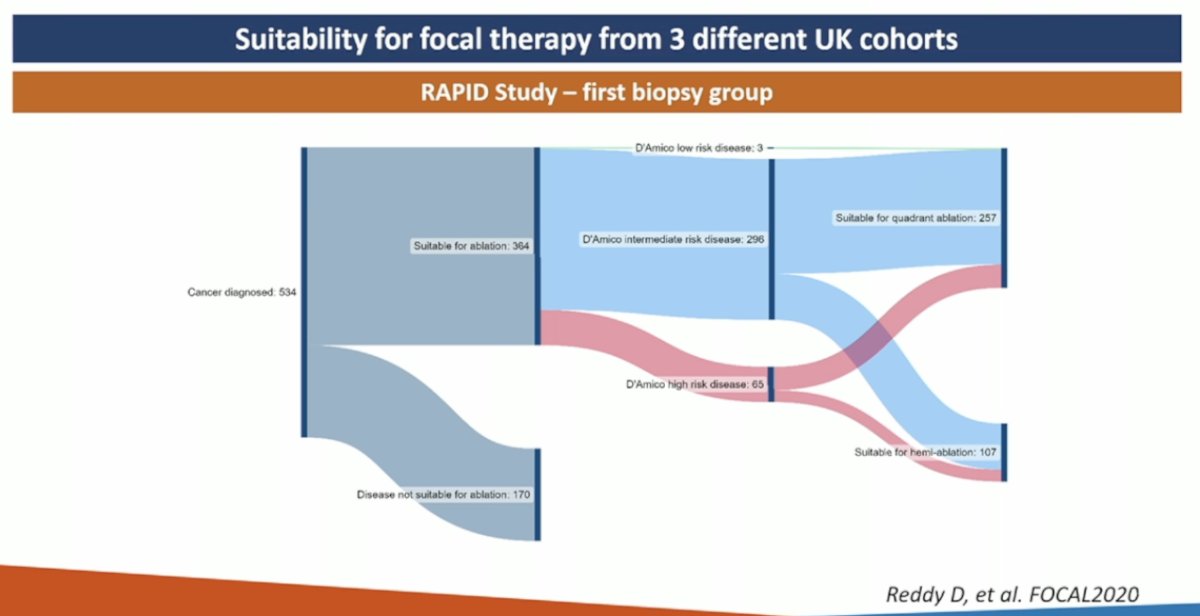
The suitability for focal therapy was assessed across three different U.K. diagnostic and screening trials in the RAPID study. Approximately 40–70% of newly diagnosed men with localized prostate cancer were found to be suitable for focal therapy based on the current Focal Therapy UK criteria.
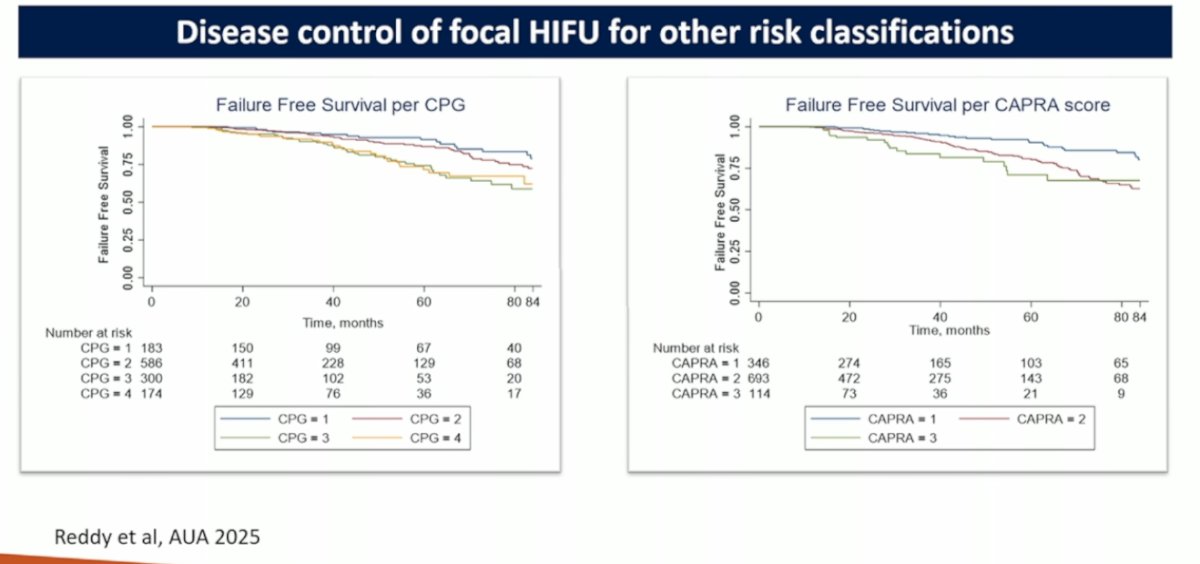
Cancer control after focal therapy is generally good enough, Longer-term outcomes are now available from modalities such as transrectal ultrasound-guided HIFU (graphic below), cryotherapy, and irreversible electroporation (IRE). If individuals using these modalities are not achieving comparable outcomes, it suggests they are not applying the technique correctly. Importantly, outcomes from one modality are not directly translatable to another. There are no shortcuts for newer focal therapy approaches; instead, they should learn from the lessons and mistakes made over the past two decades.
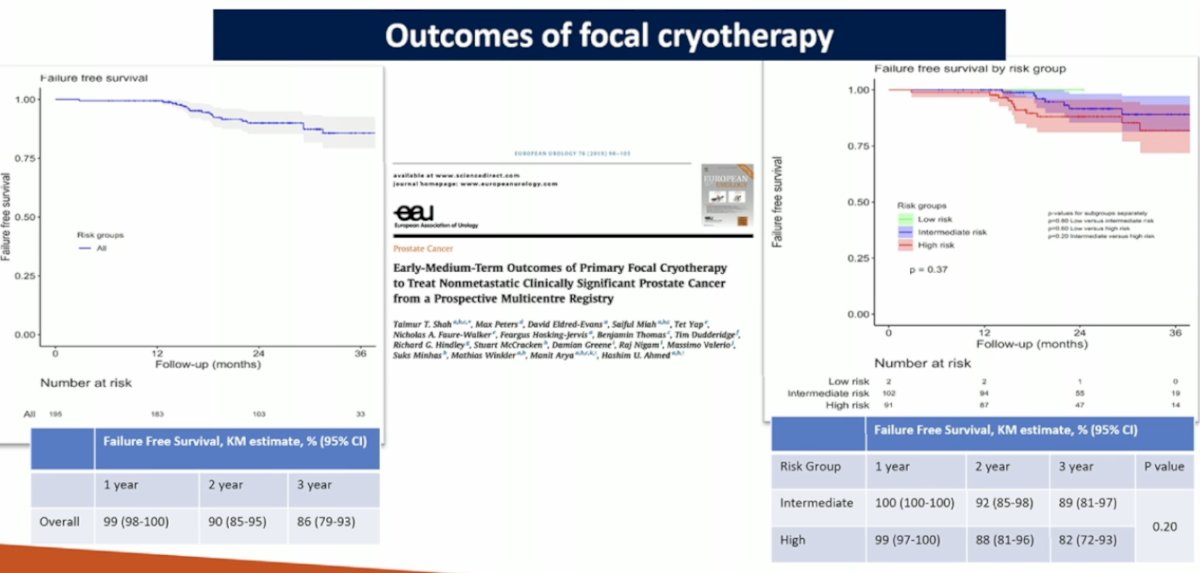
Cryotherapy and IRE have demonstrated excellent outcomes, with overall failure-free survival (FFS) rates of 90% at 2 years and 86% at 3 years.
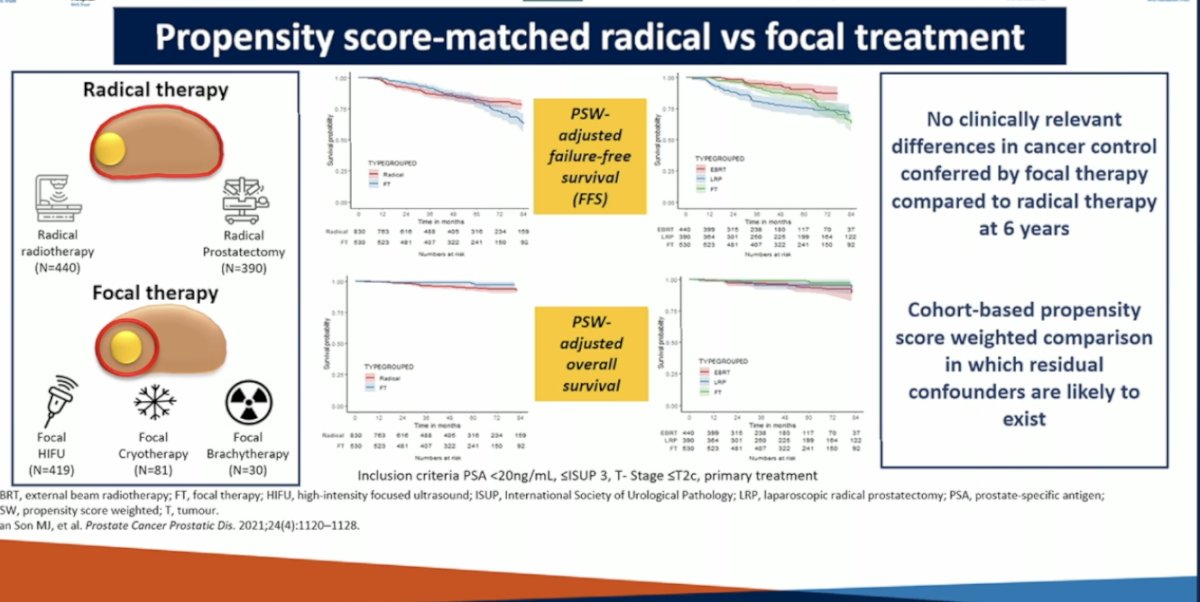
There are non-randomized data, including a propensity score–matched (PSM) study, comparing radical treatment versus focal therapy in patients with PSA <20 ng/mL, ISUP Grade Group 3, and clinical stage ≤T2c undergoing primary treatment. This study found no clinically relevant differences in cancer control between focal therapy and radical therapy at 6 years. However, it was a cohort-based, propensity score–weighted comparison, and the possibility of residual confounders remains likely.
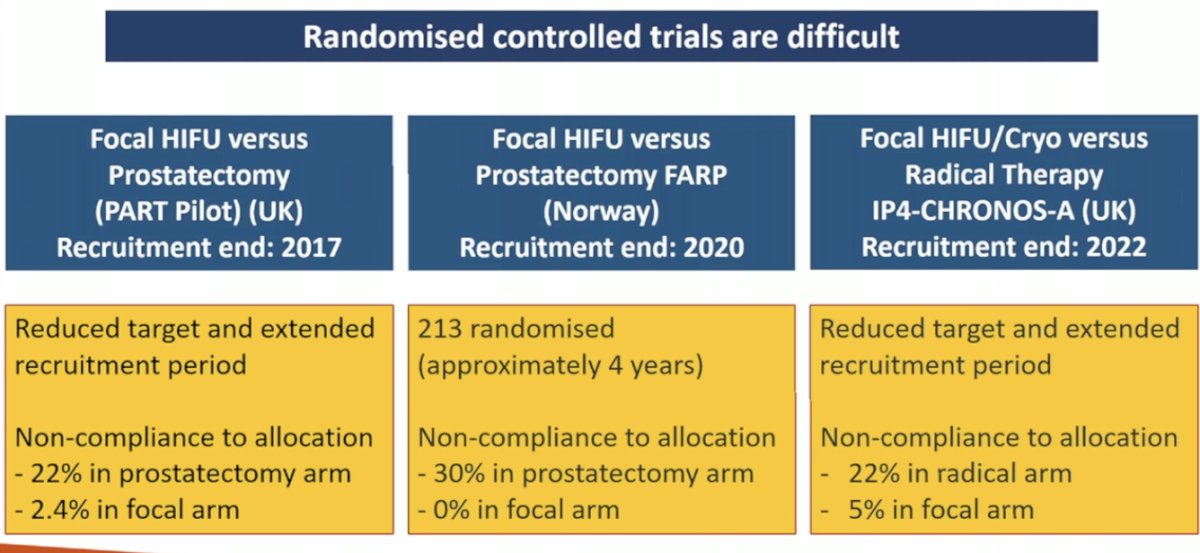
Dr. Ahmed highlighted the challenges of conducting randomized controlled trials in this setting. He discussed three trials comparing focal HIFU or cryotherapy versus radical therapy, all of which were limited by a reduced target population, prolonged recruitment periods, and significant non-compliance with treatment allocation in the radical therapy arms.
Dr. Ahmed concluded his presentation with the following key points:
- Focal therapy represents a natural evolution in surgical oncology, building on the precision diagnosis advances of the past decade.
- Treatment-related side effects are reduced 5- to 10-fold compared to radical therapy.
- Focal therapy has shown iso-effective cancer control compared to radical therapy at 5 to 10 years.
- It should be routinely offered as a standard option for eligible intermediate-risk patients, and select high-risk cases may also be appropriate candidates.
- Samir Taneja, MD, Professor of Urologic Oncology in the Department of Urology at NYU Grossman School of Medicine, Vice Chair of Urology and Director of Urologic Oncology at NYU Langone Health. New York, NY.
- Edward Schaeffer, MD, PhD, Chair of the Department of Urology at Feinberg School of Medicine and Program Director of the Genitourinary Oncology Program at the Robert H. Lurie Comprehensive Cancer Center of Northwestern University. Chicago, IL.
- Lara Rodríguez Sánchez, MD, PhD, Urologic Surgeon Associate Assistant, Institut Mutualiste Montsouris, Ville de Paris, France.
- Hashim Ahmed, MD, Chair of Urology and Head of the Section of Specialty Surgery at Imperial College London, London, UK.
- Himanshu Nagar, MD, MS, Radiation Oncologist at the Memorial Sloan Kettering Cancer Centre, New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
References
- Kasivisvanathan V, Rannikko AS, Borghi M, et al.; PRECISION Study Group Collaborators. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med. 2018;378(19):1767-1777. doi:10.1056/NEJMoa1801993
- Kinnaird A, Luger F, Cash H, et al. Microultrasonography-Guided vs MRI-Guided Biopsy for Prostate Cancer Diagnosis: The OPTIMUM Randomized Clinical Trial. JAMA. 2025 Mar 23:e253579. doi:10.1001/jama.2025.3579
- Ślusarczyk A, Rajwa P, Barnaś A, Ismail H, et al. Outcomes of Focal Therapy for Localized Prostate Cancer: A Systematic Review and Meta-analysis of Prospective Studies. European Urology Oncology. 2025.
- Soeterik, T.F.W., van Melick, H.H.E., Dijksman, L.M., Biesma, D.H., Witjes, J.A., & van Basten, J.A. (2021). Multiparametric Magnetic Resonance Imaging Should Be Preferred Over Digital Rectal Examination for Prostate Cancer Local Staging and Disease Risk Classification. Urology, 147, 205–212.
- Bianco, F.J., Martinez-Salamanca, J.I., Kattan, M.W., et al. (2025). Natural History of Patients Undergoing Transperineal Fusion Biopsies to Transperineal Fusion Cryoablation: 5-Year Outcomes. Journal of Endourology, 39(S2), S3–S12.
- Emmett, L., Buteau, J., Papa, N., et al. (2021). The PRIMARY Score: Using Intraprostatic 68Ga-PSMA PET/CT Patterns to Improve the Diagnostic Accuracy of Clinically Significant Prostate Cancer. Journal of Nuclear Medicine, 62(5), 603–609.
- Weinstein, I.C., Wu, X., Hill, A., Brennan, D., Omil-Lima, D., Basourakos, S., Brant, A., Lewicki, P., Al Hussein Al Awamlh, B., Spratt, D., Bittencourt, L.K., Scherr, D., Zaorsky, N.G., Nagar, H., Hu, J., Barbieri, C., Ponsky, L., Vickers, A.J., & Shoag, J.E. (2023). Impact of Magnetic Resonance Imaging Targeting on Pathologic Upgrading and Downgrading at Prostatectomy: A Systematic Review and Meta-analysis. European Urology Oncology, 6(4), 355–365.
- Ślusarczyk, A., Rajwa, P., et al. (2025). Outcomes of Focal Therapy for Localized Prostate Cancer: A Systematic Review and Meta-analysis of Prospective Studies. European Urology Oncology.
- Klotz, L., Pavlovich, C. P., Chin, J., et al. (2021). Magnetic Resonance Imaging–Guided Transurethral Ultrasound Ablation of Prostate Tissue in Patients with Localized Prostate Cancer: A Prospective Phase I Clinical Trial. The Journal of Urology, 205(3), 769–779.
- Ehdaie, B., Tempany, C. M., Holland, F., et al. (2022). MRI-guided focused ultrasound focal therapy for patients with intermediate-risk prostate cancer: a phase 2b, multicentre study. The Lancet Oncology, 23(7), 844–853.