(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the Plenary Session on Saturday. Dr. Samir Taneja gave the State-of-the-Art Lecture titled: Focal Therapy in Prostate Cancer: Prime Time or Not Time?
Dr. Taneja began by discussing why focal therapy has emerged as a treatment paradigm. He explained that focal therapy has largely arisen from the perceived inadequacies of current treatment options, including concerns about the marginal improvements in mortality seen with screening (ERSPC/PLCO), the risks of overtreatment highlighted in trials like PIVOT and ProtecT, and the significant impact of current treatments on quality of life.1,2 There remains a persistent desire to treat men to mitigate the risks of disease progression and mortality, particularly given poor compliance with active surveillance, patient anxiety, and the recognized potential for lethality in some cases. Additionally, the emergence of tools that allow for better characterization of tumor risk, extent, size, and location has further propelled the development of focal therapy as a viable approach.
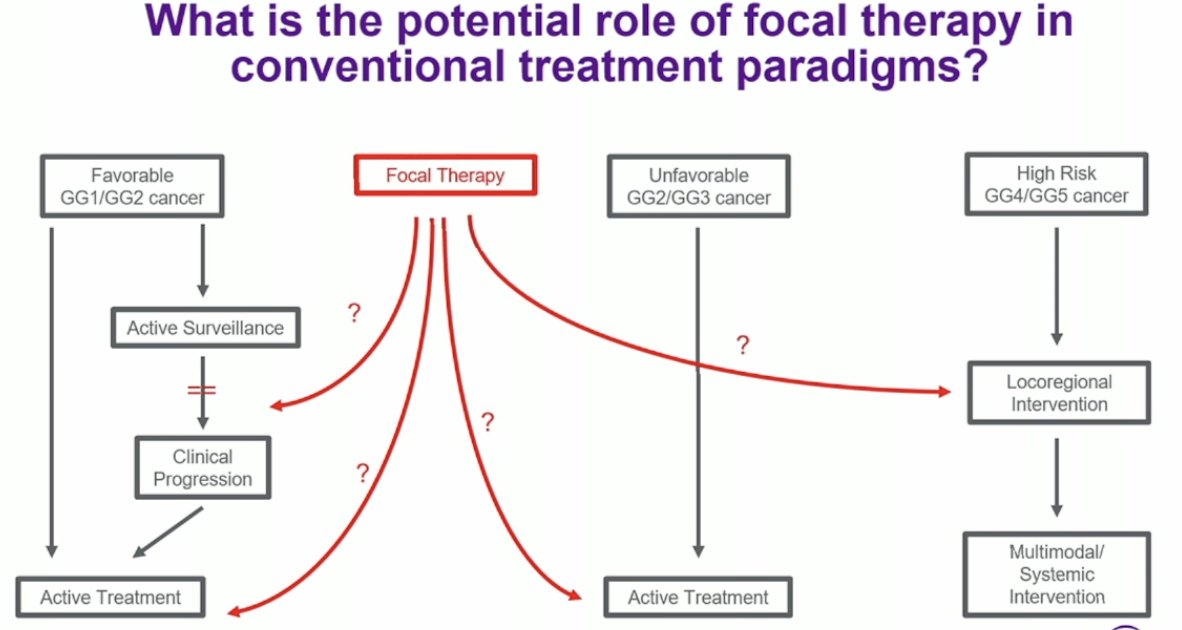
The potential role of focal therapy could be envisioned across various treatment paradigms, either as an alternative to active surveillance or as an active treatment option, particularly for intermediate-risk patients and even for select high-risk patients undergoing locoregional intervention, as illustrated below.
When considering who is the right patient for focal therapy, disease risk remains a subject of debate; however, intermediate-risk patients appear to be the "sweet spot." These patients typically have a longer lead time to metastatic disease, a lower risk of mortality, and if focal therapy fails, salvage treatment remains feasible within a 5–to 10-year window, with disease likely to remain localized. Moreover, many of these patients would otherwise go on to require radical therapy if managed with surveillance alone. Ideally, significant disease should be MRI-visible and show spatial alignment between imaging and biopsy findings. Tumor location within the prostate is also important: anterior tumors, even if large, are often ideal for safe ablation, while posterior tumors should be smaller and located away from the distal apex to minimize treatment risks.
Who Cannot Have Focal Therapy?
Dr. Taneja discussed the patient populations who should not undergo focal therapy. Men with locally advanced disease, including seminal vesicle invasion or gross extracapsular extension, are not ideal candidates, particularly when no metastatic disease is present. Patients with multifocal clinically significant prostate cancer (csPCa), especially when spatially unrelated or involving a large number of foci, also pose challenges, as treatment must balance the ablative volume with overall gland size. A high local disease burden may preclude adequate clearance, and extreme apical disease adds further difficulty. The use of focal therapy in men with high-risk disease remains more controversial, given concerns about metastatic progression, the possibility of occult metastases at baseline, and a higher risk of local failure. Young men may also not be ideal candidates, as the long-term durability of focal therapy remains unproven, and salvage prostatectomy after focal therapy may lead to reduced functional outcomes. Dr. Taneja noted that the ProtecT trial demonstrated a survival benefit for surgery in reducing prostate cancer mortality, further emphasizing the need for careful patient selection.3
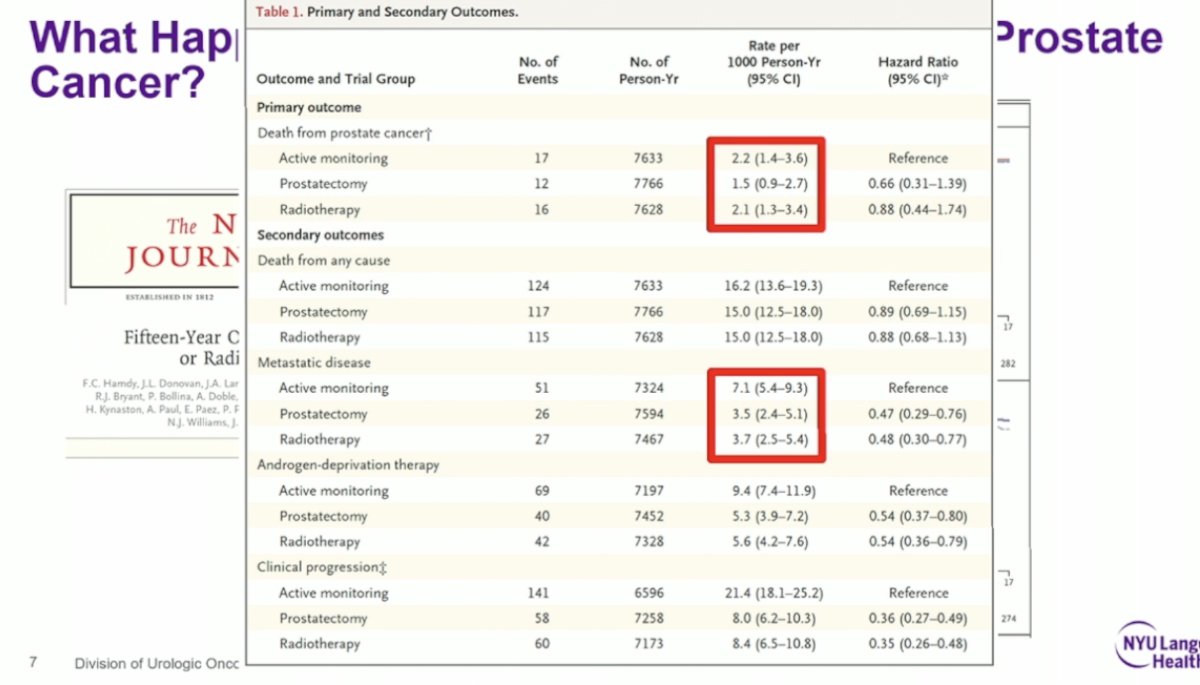
We learned a great deal from the ProtecT study, which enrolled a cohort of men with favorable-risk prostate cancer. At 15 years, both the risk of mortality and metastatic progression were remarkably low, regardless of the initial management strategy, as illustrated below. One of the key lessons from ProtecT is that men with favorable-risk prostate cancer rarely die from the disease within 15 years, whether they undergo active monitoring, surgery, or radiotherapy. As Freddie Hamdy paraphrased, for the average man diagnosed with favorable-risk prostate cancer, "the worst thing that may happen in his lifetime is radical therapy." This highlights the importance of avoiding overtreatment in a population unlikely to die from prostate cancer.3
Dr. Taneja then discussed what we currently know about focal therapy. There are many available tools for tissue ablation, most of which achieve good locoregional control in the short term. The side effect profile of focal therapy is favorable, with rare complications, less short-term impact on potency and continence compared to surgery, and less long-term impact on potency, urinary function, and bowel function compared to radiation. Short- and medium-term locoregional control rates are relatively high, and metastatic recurrences following focal therapy are rare. Importantly, re-treatment is highly feasible and effective in cases of local recurrence, whether through repeat ablation or conversion to radical therapy.
Dr. Taneja highlighted that we may be using the wrong definition of success for focal therapy if we focus solely on long-term outcomes like metastasis-free survival (MFS), cancer-specific survival (CSS), and overall survival (OS). These outcomes take many years to mature and may not fully capture the clinical impact of focal therapy. He suggested that other outcomes might provide a better assessment of success, including recurrence-free survival (any cancer), clinically significant cancer-free survival (any pattern 4 disease), progression-free survival (worsening cancer), re-treatment-free survival (any subsequent treatment) and radical treatment-free survival. Additionally, preserving quality of life remains a critical endpoint when evaluating focal therapy.
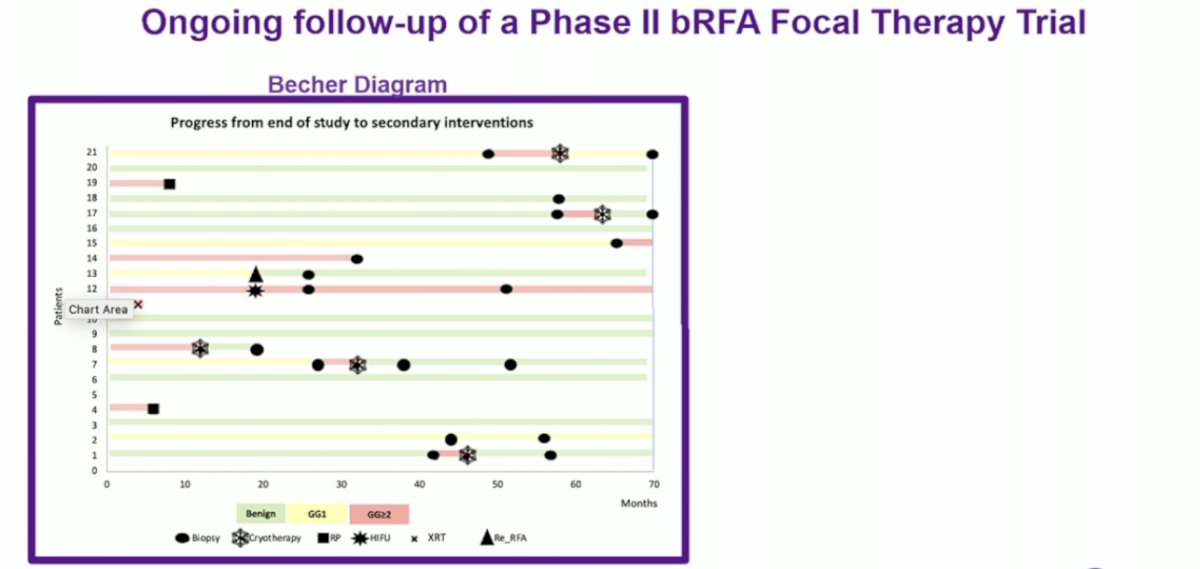
Dr. Taneja presented data from the ongoing follow-up of a Phase II focal therapy trial using bipolar radiofrequency ablation (bRFA). With a median follow-up of 79 months (IQR 67–82), disease-free survival (DFS) was 38%, while clinically significant DFS reached 57%. When including patients who underwent repeat ablation, DFS and clinically significant DFS improved to 57% and 71%, respectively. Freedom from secondary treatment was 52%, and freedom from radical therapy was 81%. Importantly, metastasis-free survival, cancer-specific survival, and overall survival were all 100%. These outcomes highlight that while recurrence is not uncommon, two-thirds of patients remain free of clinically significant recurrence over the long term.4
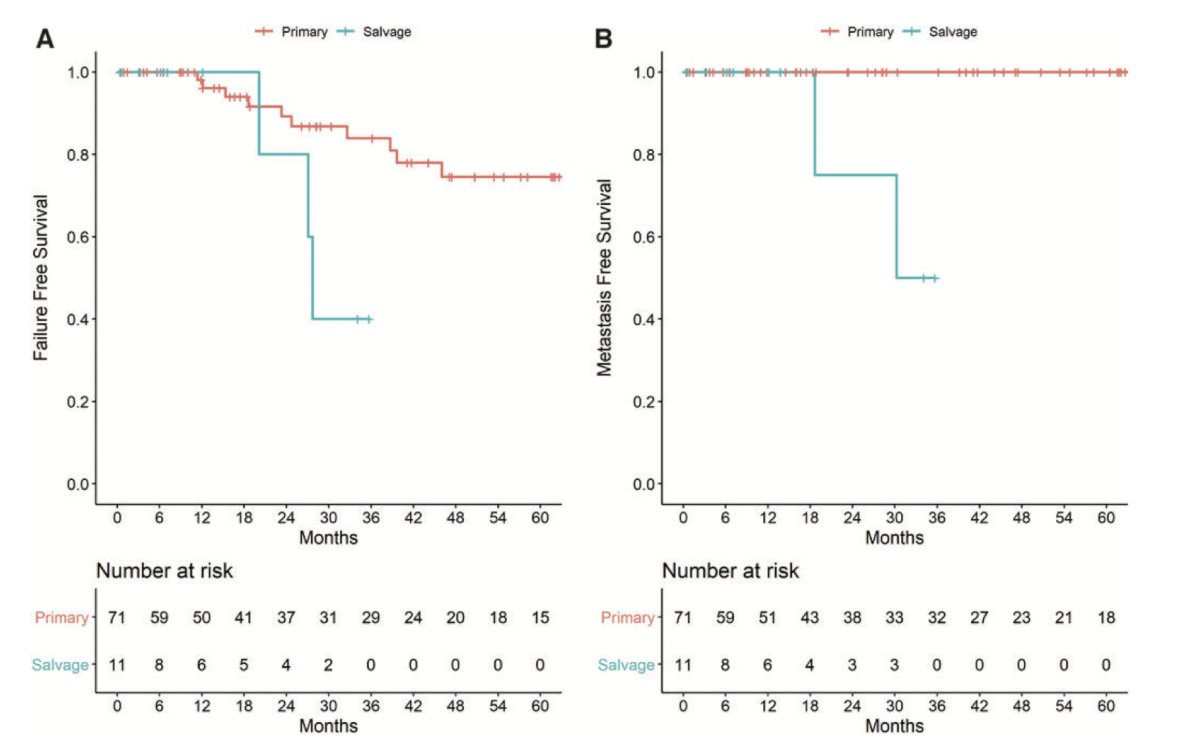
Furthermore, Dr. Taneja discussed a short-term follow-up study of partial gland cryoablation, where failure-free survival was defined as the absence of infield recurrence, out-of-field recurrence, need for whole-gland or systemic therapy, and death. In the primary therapy group, failure-free survival rates at 1, 2, 3, 4, and 5 years were 98%, 89%, 84%, 75%, and 75%, respectively. In the salvage therapy group, the rates at 1, 2, and 3 years were 100%, 80%, and 40%, respectively.5
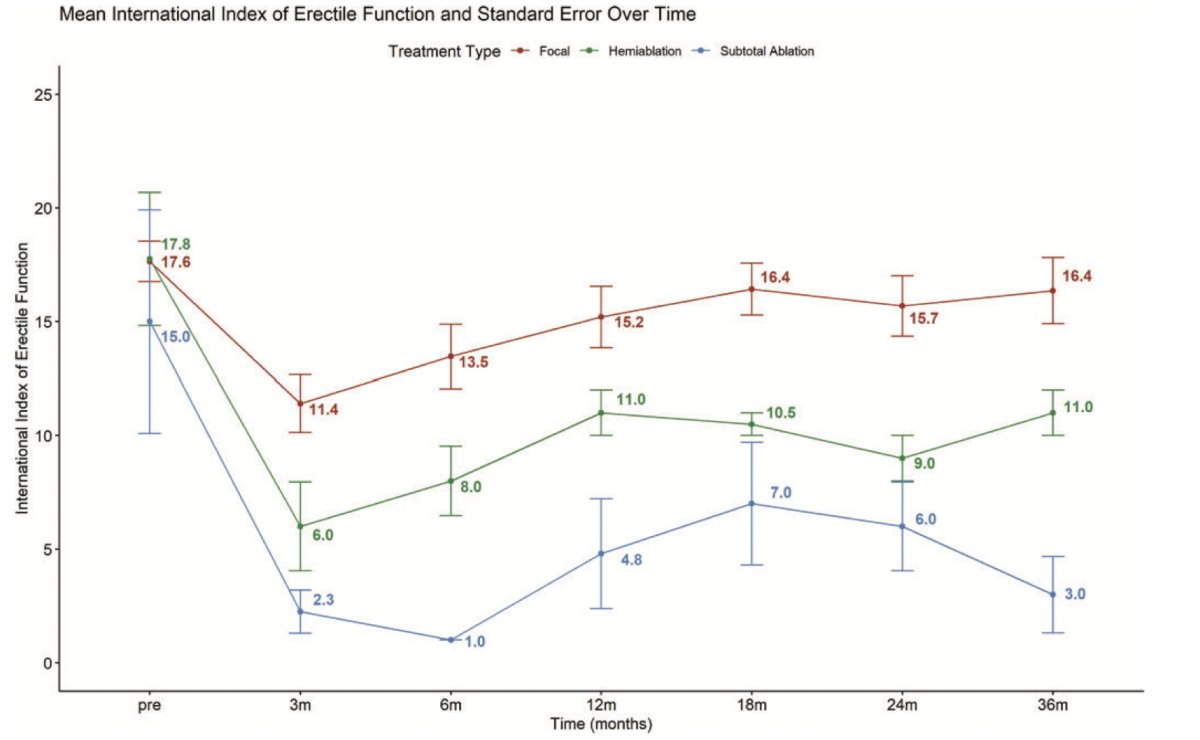
Moreover, quality of life outcomes following partial gland cryoablation are encouraging. Erectile function tends to decline initially but recovers in most men over time, while urinary function not only recovers but often improves, as shown in the data below.
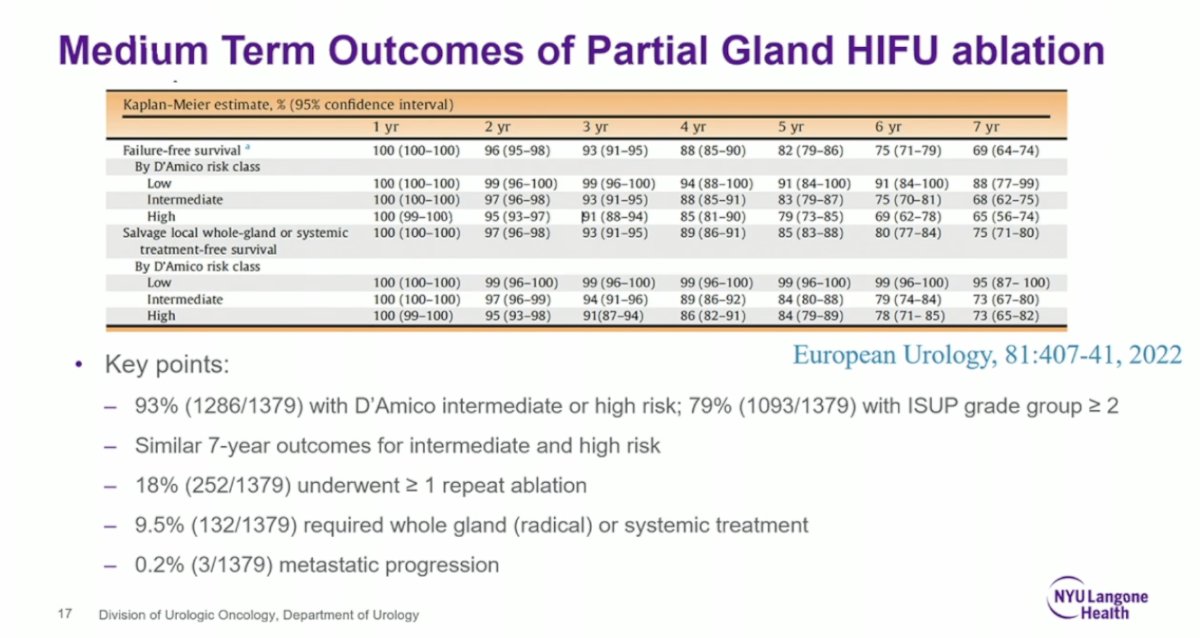
Similarly, in men treated with high-intensity focused ultrasound (HIFU), 7-year outcomes have been encouraging. The FFS rate was 69%, and metastatic progression remained rare. Among the cohort, 93% (1286/1379) had D'Amico intermediate- or high-risk disease, and 79% (1093/1379) had ISUP grade group ≥2 cancers. Outcomes at 7 years were similar for both intermediate- and high-risk groups. During follow-up, 18% (252/1379) of patients underwent at least one repeat ablation, 9.5% (132/1379) eventually required whole-gland (radical) or systemic treatment, and only 0.2% (3/1379) developed metastatic disease.6
Skepticism around focal therapy in prostate cancer remains high. Critics often point out that MRI does not detect all cancer foci, that prostate cancer is inherently multifocal, and question why focal treatment would be pursued instead of definitive whole-gland therapy when a cure might be possible. Some also argue that any recurrence should be considered a failure.
To address these criticisms and properly evaluate focal therapy, several critical concepts must be accepted. First, the therapeutic goal of focal therapy is distinct from that of conventional treatments: while there is a high likelihood of residual cancer foci of uncertain significance, the primary goal is the prevention of metastasis and cancer-related mortality. Focal therapy should be considered a disease management strategy rather than a curative one. Second, re-treatment must be seen as both acceptable and feasible, integrated as part of the overall management plan. Third, there are currently no long-term comparative outcomes, and no consensus exists yet on definitions of success. Finally, candidate selection and follow-up strategies continue to evolve as our understanding of focal therapy improves.
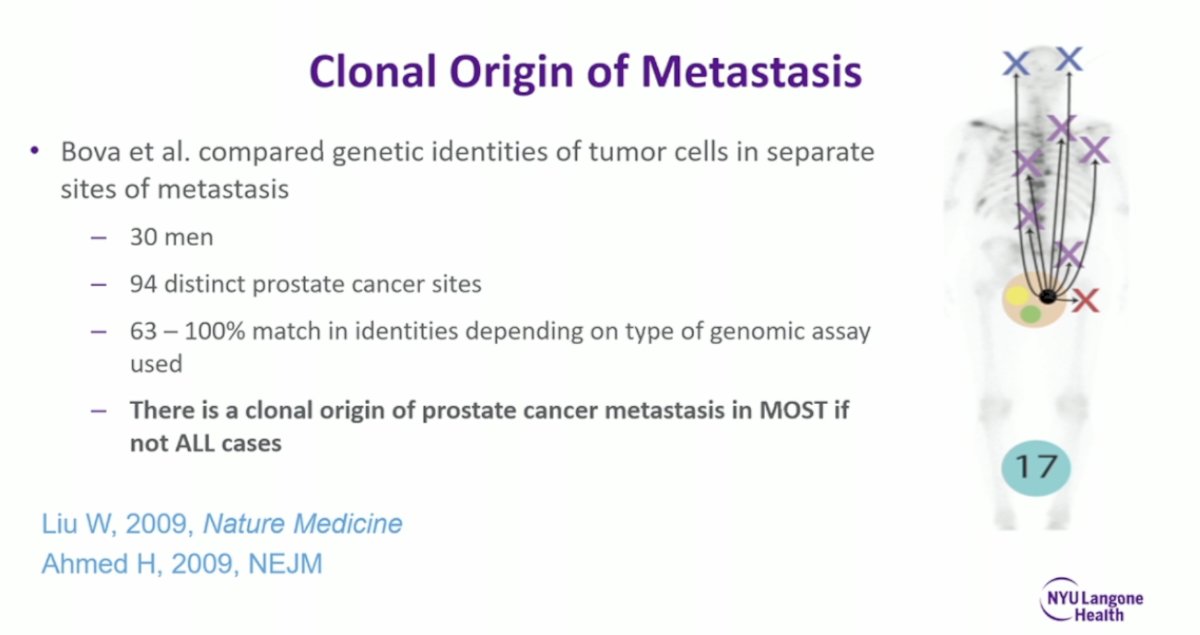
Much of the rationale for focal therapy stems from the understanding that most metastatic progression in prostate cancer arises from a clonal origin within the prostate. Bova et al. compared the genetic identities of tumor cells across separate metastatic sites in 30 men, analyzing 94 distinct prostate cancer samples. They found a 63–100% match in tumor identities, depending on the type of genomic assay used. These findings suggest that in most, if not all, cases, prostate cancer metastases originate from a single clonal source within the prostate.
The character of non-index lesions in prostate cancer further supports the rationale for focal therapy. Ohori et al.introduced the concept of the index lesion, showing that it contains approximately 80% of the total tumor volume and carries the dominant Gleason score in 92% of cases, while non-index lesions rarely contribute to extracapsular extension (1%). Similarly, Villers et al, reported that secondary lesions were smaller than 0.5 cc in 80% of cases. Collectively, these findings suggest that treatment directed at the index lesion could leave 79% of men with only residual, clinically insignificant disease.
However, this rationale is not always perfect, and questions remain about the true significance of the disease that may be left behind after focal therapy. Whole-mount correlative studies from radical prostatectomy specimens have shown that MRI detects 86% of solitary lesions and 77% of index lesions. Among non-index tumors, 14% (33/239) were ≥7 mm, with 18 of these missed by MRI, and 5% (12/239) were Gleason 4+3 or higher, with 6 missed by imaging. Missed tumors were typically smaller than those detected, and their spatial relationship to the index lesion was often unclear. It is important to note, however, that the relevance of these findings is uncertain, as these patients likely would not have been ideal candidates for focal therapy in the first place.7
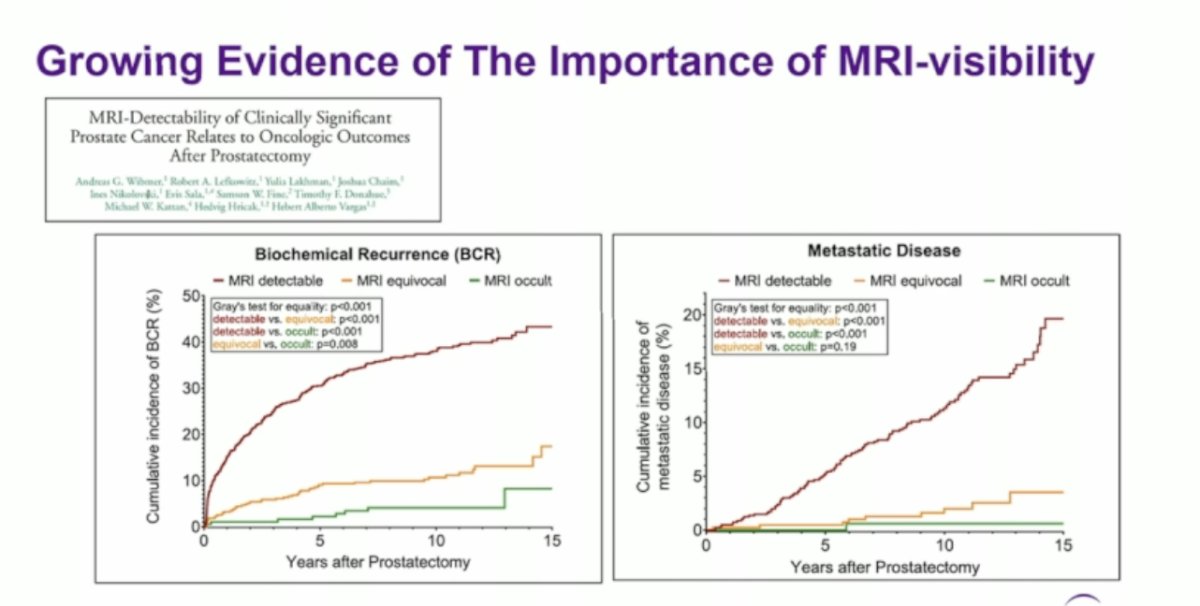
There is growing evidence supporting the importance of MRI visibility in prostate cancer. In a retrospective analysis of 1,449 patients with csPC who underwent preoperative MRI followed by radical prostatectomy, tumors were categorized based on their MRI visibility. Patients who experienced biochemical recurrence (BCR) and metastatic disease had a higher incidence of MRI-detectable tumors.8
One of the recognized pitfalls of MRI in prostate cancer is that it does not reveal all of the disease. However, it remains a very good guide. MRI typically shows only a portion of the tumor and a surrounding halo has been found to have csPC, as illustrated below.
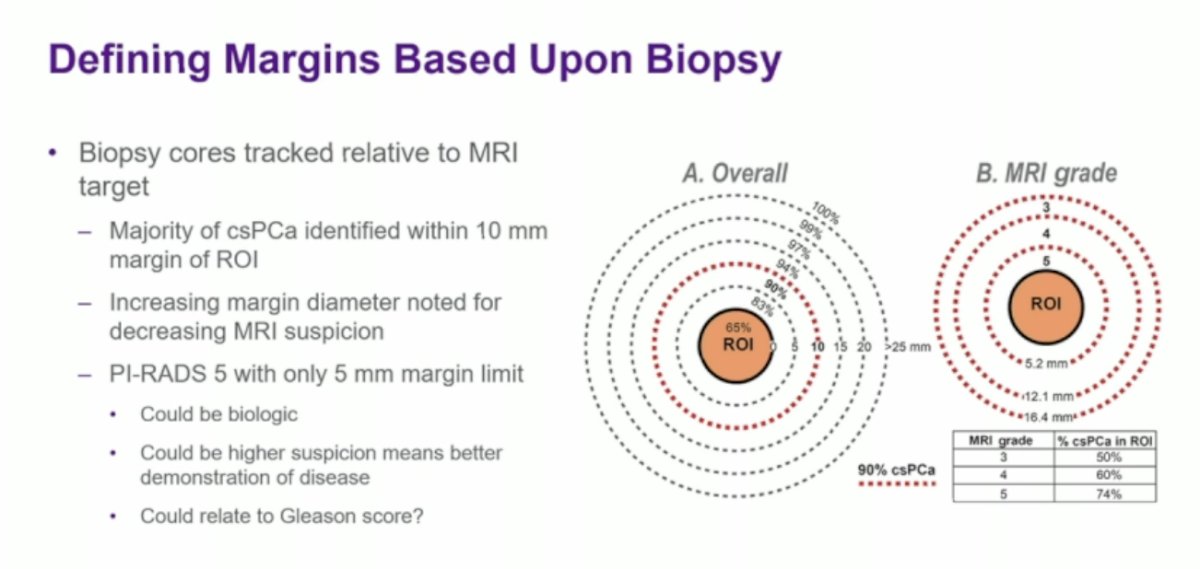
To better guide focal therapy, margins must be defined based on biopsy data, with biopsy cores tracked relative to the MRI target. Studies have shown that the majority of csPC are identified within a 10 mm margin around the region of interest (ROI). Interestingly, the required margin tends to increase as MRI suspicion decreases; for example, PI-RADS 5 lesions often require only a 5 mm margin. This could be due to biological differences, better visualization of higher-risk disease, or a correlation with higher Gleason scores. Dr. Taneja noted that a 9 mm margin would likely be sufficient, referencing data from the UCLA group that supports this approach.
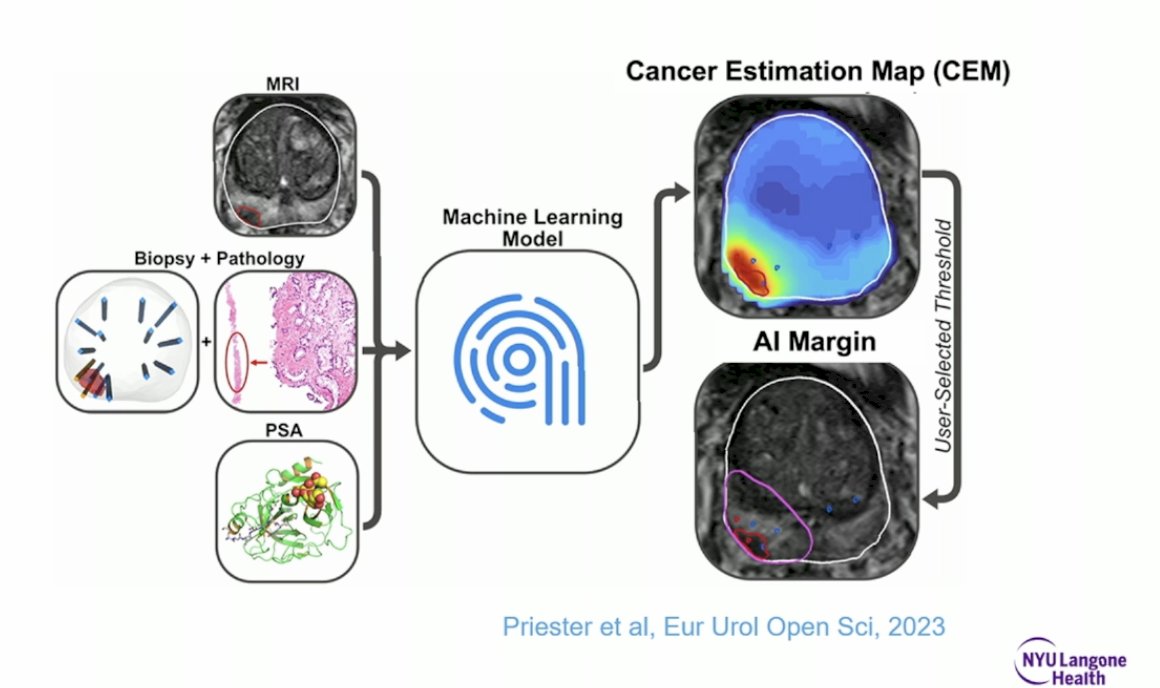
New technologies are emerging that can help refine focal therapy planning. Advanced MRI techniques, combined with artificial intelligence (AI) tools and ultrasound (US) data integration, are enhancing our ability to more accurately define tumor margins, detect clinically significant disease, and guide precise treatment delivery.
The availability of better tools has helped bring focal therapy into prime time. MRI-targeted biopsy platforms, including fusion imaging and spatial recording of biopsy cores, have improved the precision of diagnosis and treatment planning. Mapping tools now allow for more accurate assessment of tumor extent. A growing variety of ablative energy sources has expanded the ability to treat tumors of varying size and location, with most technologies demonstrating similar ablative efficacy. Additionally, the development of new imaging modalities, such as PSMA PET and micro-ultrasound, is further enhancing the ability to define tumor extent and clinical significance.
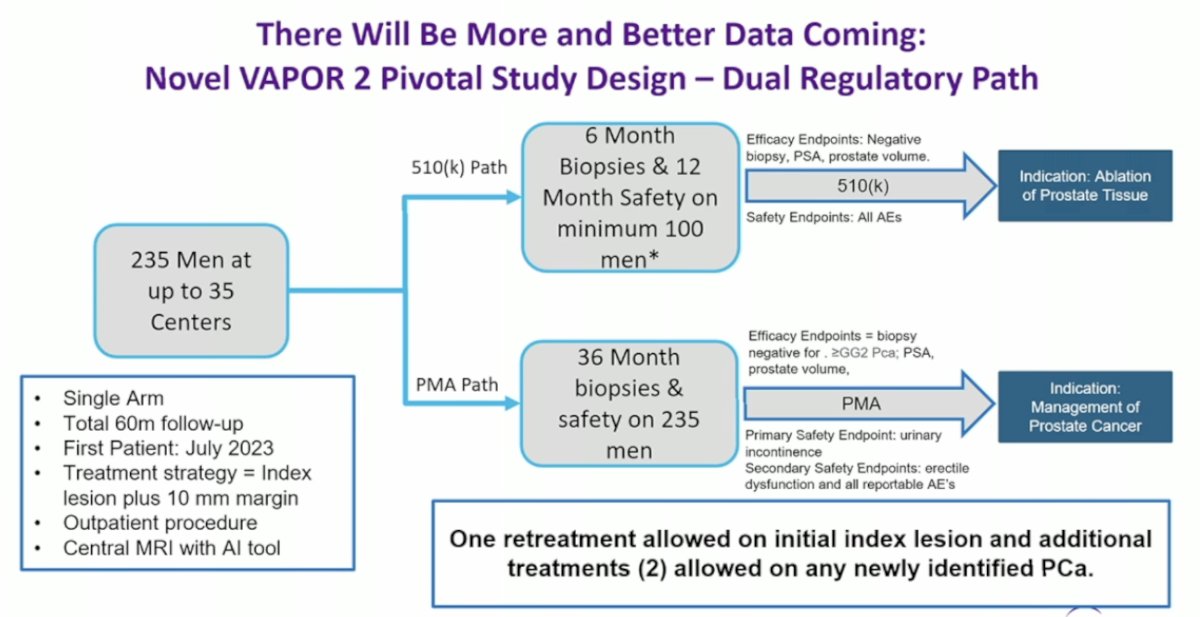
Looking ahead, Dr. Taneja highlighted that more and better data will soon be available. He specifically mentioned the VAPOR 2 pivotal study, which is enrolling 325 men across up to 35 centers. This trial is evaluating focal therapy using water vapor ablation for the treatment of intermediate-risk prostate cancer.
Starting a successful focal therapy program requires a foundation of high-quality work and strong multidisciplinary collaboration. This includes close coordination between urology, radiology, and pathology teams, with expertise in prostate MRI interpretation, MRI-targeted biopsy techniques, and infrastructure for radiology-pathology correlation. Ongoing quality assessment and quality improvement efforts are also essential. In addition, it demands a significant investment of dedicated time to gain proficiency with a chosen ablative energy platform. Strict protocols for patient tracking and follow-up must be in place, along with a clear strategy for managing salvage indications and approaches when needed.
Dr. Taneja concluded his presentation with several key messages. Focal therapy has demonstrated favorable locoregional disease control for up to 5–10 years, with reproducible outcomes that appear independent of energy source or disease risk, and a low rate of metastatic progression. Most recurrences remain salvageable, whether through local retreatment or radical therapy. Compared to conventional therapies, focal therapy offers improved short-term quality of life relative to surgery and potentially better long-term quality of life than radiation. Advances in diagnostic and staging tools have further empowered more precise candidate selection and follow-up strategies. However, long-term comparative outcomes and definitive evidence of mortality benefit are still lacking, although this was similarly true at the inception of other treatment modalities. Practical experience has shaped current approaches, with formal trials following later.
In answering whether focal therapy is ready for prime time, Dr. Taneja concluded that it is, but only if it is done well, with careful candidate selection, meticulous treatment planning, complete and aggressive treatment of the index tumor, rigorous follow-up, and early salvage of any recurrence.
Presented by: Samir Taneja, MD, Professor of Urologic Oncology in the Department of Urology at NYU Grossman School of Medicine, Vice Chair of Urology and Director of Urologic Oncology at NYU Langone Health. New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Wilt TJ, Brawer MK, Jones KM, et al. Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med. 2012;367(3):203-213. DOI:10.1056/NEJMoa1113162
- Schröder FH, Hugosson J, Roobol MJ, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. 2009;360(13):1320-1328. DOI:10.1056/NEJMoa0810084
- Hamdy FC, Donovan JL, Lane JA, et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N Engl J Med. 2023;388(17):1617-1628. doi:10.1056/NEJMoa2214122
- Aydin AM, Gage K, Dhillon J, et al. Prostate Radiofrequency Focal Ablation (ProRAFT) Trial: Early Efficacy of Bipolar Radiofrequency Ablation for Localized Prostate Cancer. J Urol. 2021 Apr;205(4):1098-1099. doi:10.1097/JU.0000000000001567.01. PMID: 3348701
- Tan WP, Chang A, Sze C, Polascik TJ. Oncological and Functional Outcomes of Patients Undergoing Individualized Partial Gland Cryoablation of the Prostate: A Single-Institution Experience. J Endourol. 2021 Sep;35(9):1290-1299. doi: 10.1089/end.2020.0740. Epub 2021 Mar 16. PMID: 33559527; PMCID: PMC8558074.
- Reddy D, Peters M, Shah TT, et al. Cancer Control Outcomes Following Focal Therapy Using High-Intensity Focused Ultrasound in 1379 Men with Nonmetastatic Prostate Cancer: A Multi-institute 15-year Experience. Eur Urol. 2022;81(4):407-413. doi:10.1016/j.eururo.2021.12.013
- Le Nobin J, Orczyk C, Deng FM, et al. Multiparametric Magnetic Resonance Imaging Detection of Clinically Significant Prostate Cancer: Correlation with Whole-Mount Histopathology. Eur Urol. 2015;67(3):569-576. doi:10.1016/j.eururo.2014.08.079
- Wibmer AG, Lefkowitz RA, Lakhman Y, et al. MRI-Detectability of Clinically Significant Prostate Cancer Relates to Oncologic Outcomes After Prostatectomy. Clin Genitourin Cancer. 2022;20(4):319-325. doi:10.1016/j.clgc.2022.04.001