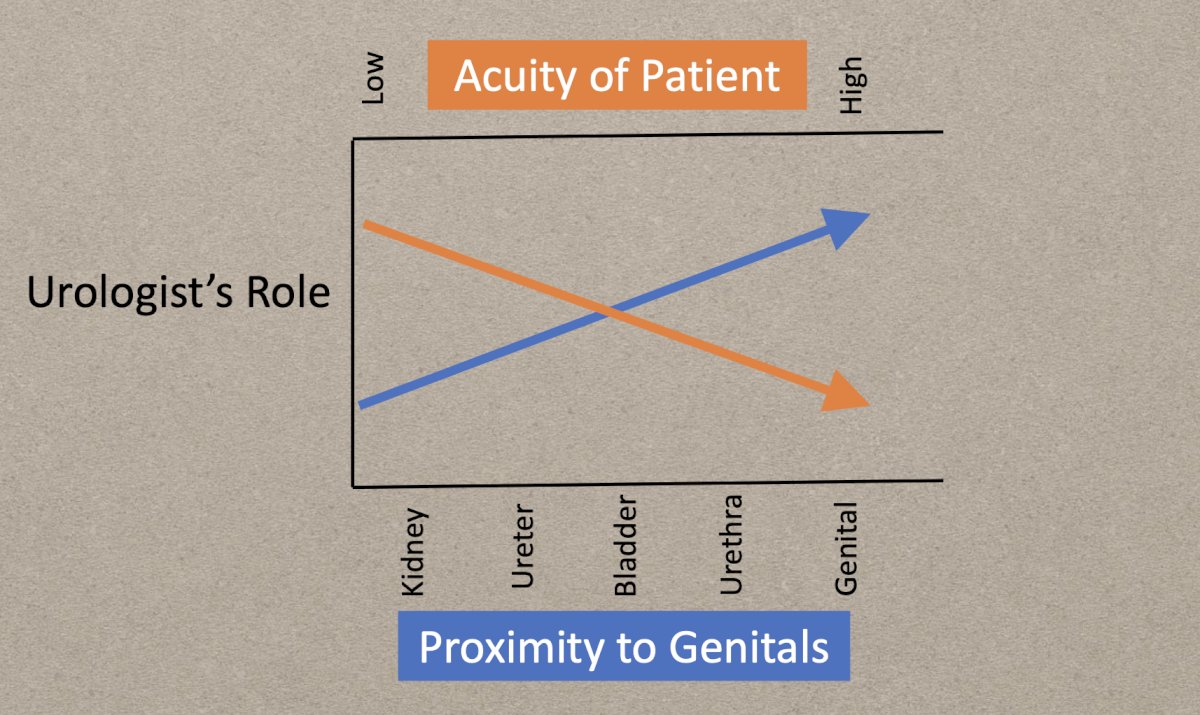
(UroToday.com) Dr. Sean Elliott, Professor of Urology at the University of Minnesota, delivered a comprehensive and informative presentation addressing the evolving role of urologists in genitourinary trauma management. After stating his financial disclosures (Laborie, study investigator and consultant; Boston Scientific, consultant), he began this plenary by explicitly saying this would not be a review of guidelines, but rather, it is a discussion of where the urologist falls in trauma care. Their role, as he uniquely conceptualized, can be thought of as directly proportional to the proximity of injury to the genitals and inversely proportional to the acuity of the patient. Simply put, urologists lead care in genital and urethral trauma, where precision is crucial and conditions are often stable. As injury sites become more proximal (bladder, ureter, kidney) and patient acuity rises, urologists take on more consultative or collaborative roles—often in conjunction with acute care surgeons. For example, he gave common scenarios of patients who present with gunshot wounds to the genital area, where the urologist would primarily direct management, versus the cases of severe bleeding due to renal trauma, where the trauma surgeon would assume primary responsibility and remove the kidney.
When discussing bladder trauma, Dr. Elliott emphasized that urologists must advocate for repair in complex extraperitoneal bladder injuries. While guidelines recommend observation or drainage for most extraperitoneal injuries, repair becomes necessary in cases involving bone fragments, concomitant rectal or vaginal injury, bladder neck injury, delayed healing, or persistent hematuria. Notably, data from the National Trauma Data Bank (NTDB) show that nearly 50% of extraperitoneal injuries underwent repair between 2002–2006—highlighting that clinical judgment frequently supports intervention.
In cases of ureteral trauma, penetrating injuries typically arise from gunshot wounds and are often accompanied by significant concurrent injuries to vascular and gastrointestinal structures. These are most often surgically treated with exploratory laparotomy. Dr. Elliott reviewed data showing that nearly half of these patients experience small bowel or colon injuries, with 38% involving major vascular trauma, commonly to the iliac vein. Management strategies include immediate repair when stable, delayed repair, or initial stenting depending on the patient’s condition. For blunt ureteral injuries, most patients undergo stenting or nephrostomy, with open reconstruction reserved for those already undergoing laparotomy for other indications.
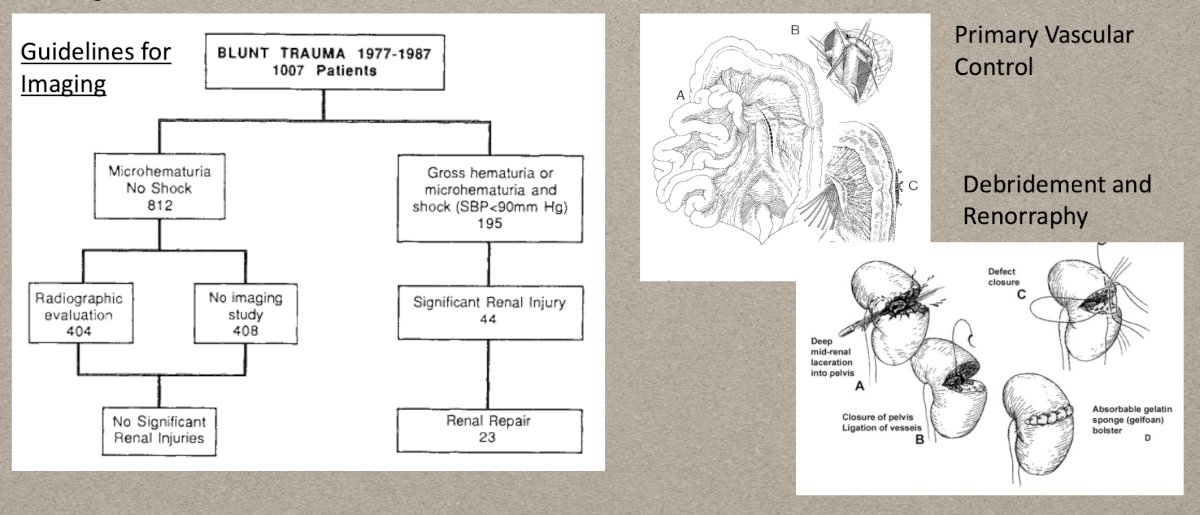
Renal trauma management has seen perhaps the most significant transformation over the last four decades. Dr. Elliott provided a historical narrative, noting that before the adoption of CT imaging in the 1980s, many renal injuries were discovered at laparotomy and often resulted in nephrectomy. The introduction of imaging, vascular control techniques, and renorrhaphy improved outcomes and allowed greater renal preservation.
By the 1990s, the development of the Organ Injury Scale (OIS) and broader acceptance of non-operative management (NOM) led to declining nephrectomy rates. The OIS was a product of the partnership between urologists and American College of Surgeons. Additionally, it was more advanced imaging techniques that led to the advent of the OIS as improved radiographic assessment of organ status allowed for more careful injury staging. Then, in the 2000s, there was an increasing trend of acute care surgeon involvement in cases of renal trauma. Their presence has been undeniably impactful, leading to better adherence to trauma protocols. Consequently, this has resulted in fewer complications such as ARDS, DVT, AKI, and sepsis. However, the most relevant effect may be the ability for urologists to now take on non-operative management strategies, mostly for cases of blunt trauma. Injuries to the kidney can parallel those to the liver and spleen, which have all now transitioned to a similar treatment paradigm of observation prior to potential embolization. Between 2002 and 2012, nephrectomy rates for high-grade renal trauma dropped significantly, from 19% to 4% for penetrating injuries and from 8% to 2% for blunt injuries. Increased use of selective angioembolization rather than surgery was a key driver of this shift.
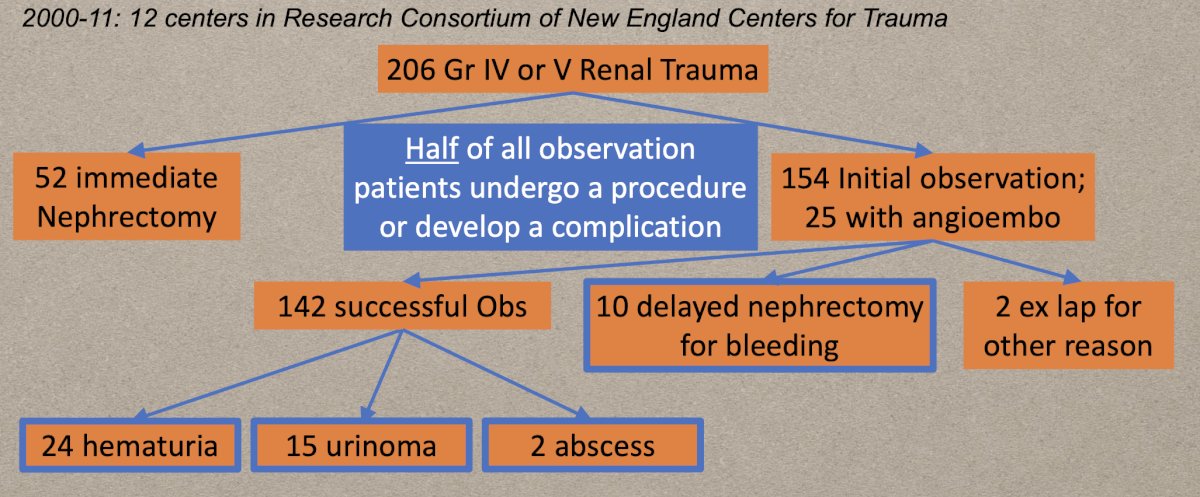
While non-operative management has become the standard approach for most renal injuries, Dr. Elliott cautioned that it demands active surveillance. Citing a paper by Van der Welden et al. in 2013, approximately half of patients initially observed for high-grade renal trauma eventually require some form of intervention, whether for hematuria, urinoma, infection, or delayed bleeding. He highlighted that missed opportunities for early intervention, such as inadequate imaging, can lead to complex late complications. Anecdotally, he referenced one patient he cared for who had a severe renal trauma, a gunshot wound that was managed at an outside hospital with surgical repair of their vena cava and right renal vein. The patient eventually developed a retroperitoneal abscess anterior to the kidney that drained for several months before coming to Dr. Elliot.
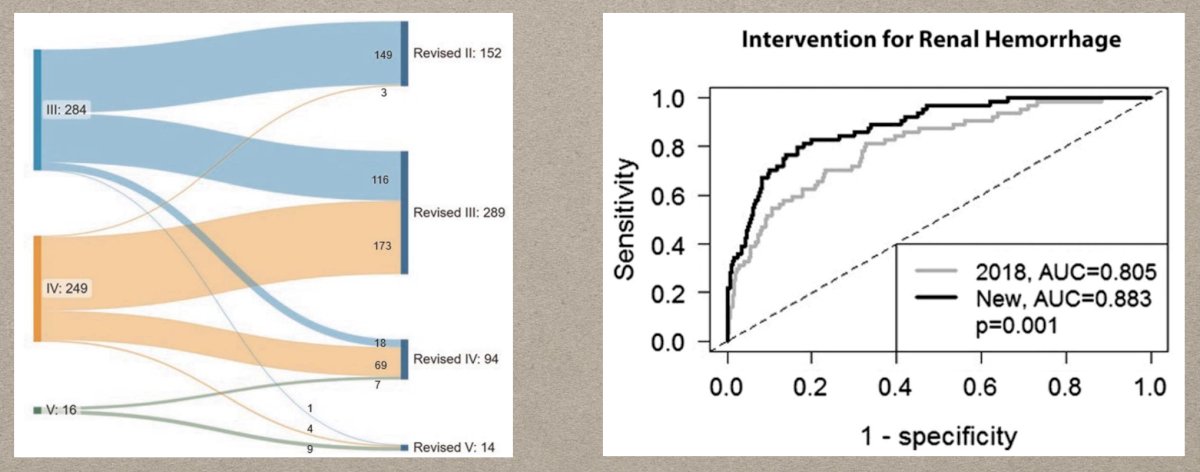
Urologists continue to lead the research and improve treatment. To illustrate this point, Dr. Elliott referenced the updates to the OIS for bleeding control, which better delineate the need for hemostatic intervention. In 2025, the management of renal trauma has evolved to a highly collaborative model. Initial triage and stabilization are typically performed by acute care surgeons, especially in community trauma centers. However, urologists remain indispensable for nuanced genitourinary management: performing delayed stenting, guiding management of bladder and urethral injuries, and ensuring complications are promptly recognized and treated.
Dr. Elliott concluded by emphasizing that urologists should continue to partner with acute care surgeons, leveraging their strengths in systemic stabilization while providing specialized expertise for GU-specific trauma. In doing so, urologists maintain a critical leadership role in ensuring optimal outcomes for patients with complex injuries.
Presented by: Sean Elliot, MD, MS, Director of Reconstructive Urology, Department of Urology, University of Minnesota, Minneapolis, MN, USA.
Written by: Yezan Hadidi, BS, Department of Urology, University of California Irvine. @yezanhadidi on X during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025