(UroToday.com) Tuesday morning’s plenary session featured an excellent crossfire debate on the management of urethral stricture disease. The session compared three sets of global guidelines: the American Urological Association (AUA), European Association of Urology (EAU), and Urological Society of India (USI). Dr. Kenneth Angermeier from the Cleveland Clinic moderated the session, which included panelists Ms. Tamsin Greenwell (EAU), Dr. Pankaj Joshi (USI), and Dr. Hunter Wessells (AUA). Each speaker presented their perspectives on the guidelines, followed by rebuttal arguments, offering insights into the complexities of urethral stricture management.
AUA guidelines contain 250 references with 81 updates and contain three levels of evidence (A indicating high certainty, B indicating moderate certainty, and C indicating low certainty). Recommendations are divided into three categories being strong, moderate, and conditional, based on both clinical principles and expert opinion. EAU contains 588 references with varying levels of evidence, labelled as either strong or weak. USI contains 55 references with Level of Evidence based on CBEM guidelines, ranging on a scale from 1-4. Recommendations are divided into three categories being strong, moderate, or weak, and are guided by clinical principles and expert opinion.
Dr. Angermeier opened the session by introducing the key topic: the comparison of global guidelines for urethral stricture management. He briefly outlined the structure of the debate, highlighting the main areas of focus for each panelist and the methodologies behind the guidelines they would discuss. Dr. Angermeier emphasized that while these guidelines are based on strong evidence, variations across regions reflect differences in healthcare systems, patient populations, and surgical expertise.
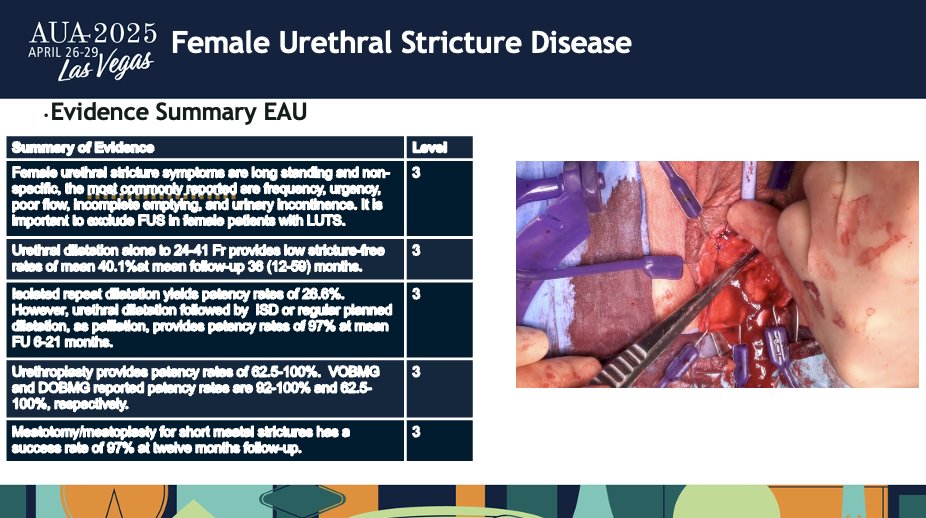
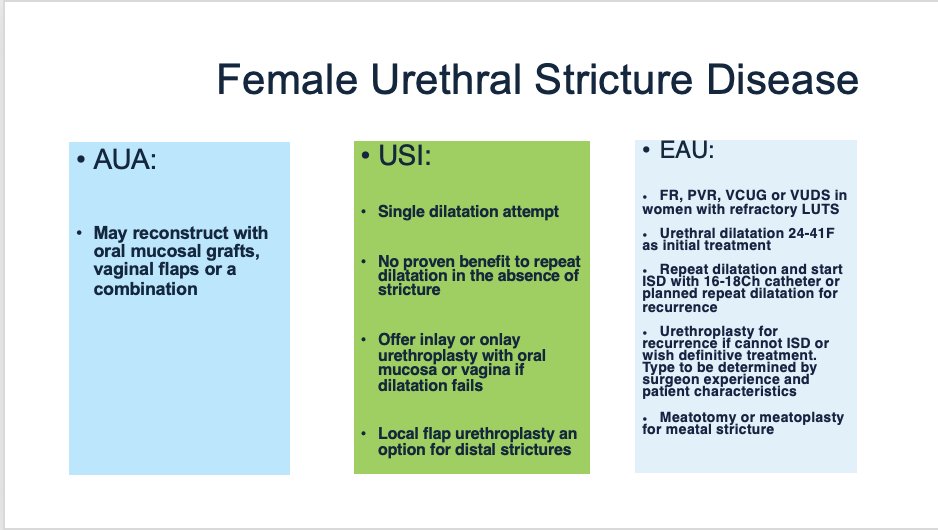
Next, Ms. Tamsin Greenwell took the podium to discuss the EAU guidelines for urethral stricture management. She began by presenting an overview of female urethral stricture disease, which is often caused by idiopathic factors, trauma, or iatrogenic injuries. The EAU guidelines recommend a stepwise approach to treatment, starting with urethral dilatation (24-41 French), followed by direct visual internal urethrotomy (DVIU) for recurrent cases. If these initial treatments fail, EAU guidelines suggest urethroplasty with oral mucosal grafts (BMG) or labial flaps for long-term resolution.
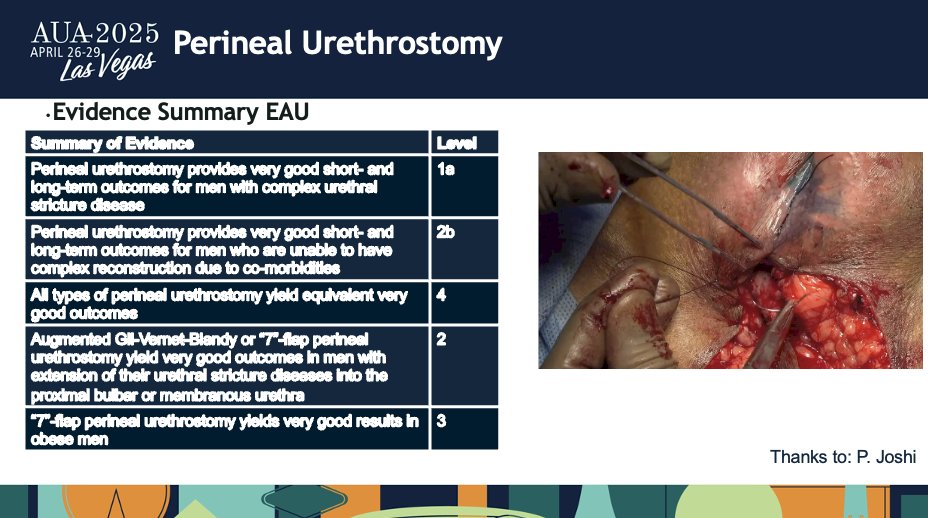
Ms. Greenwell highlighted the EAU's focus on comprehensive diagnostic approaches, such as flow rate measurements and cystourethroscopy, to guide treatment decisions. She also emphasized the use of perineal urethrostomy (PU) as an option for complex anterior strictures, particularly for patients who are unfit for reconstruction.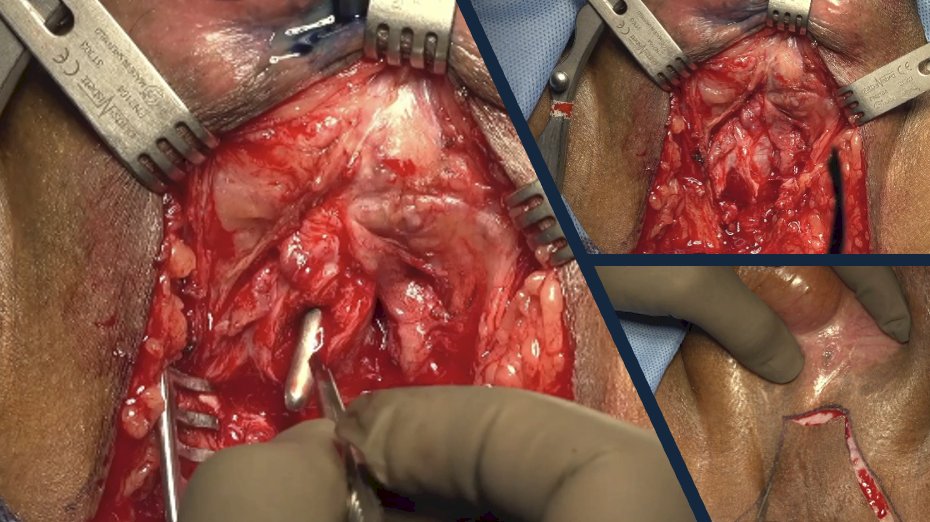
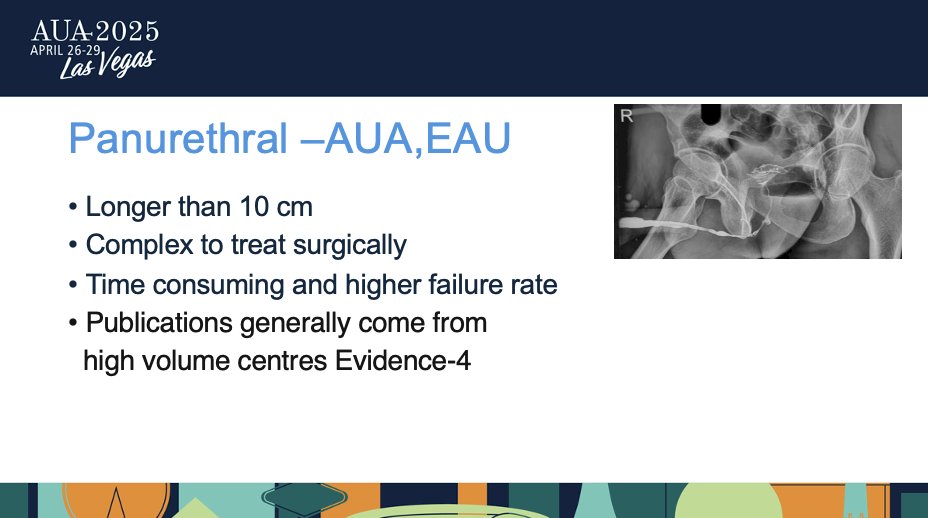
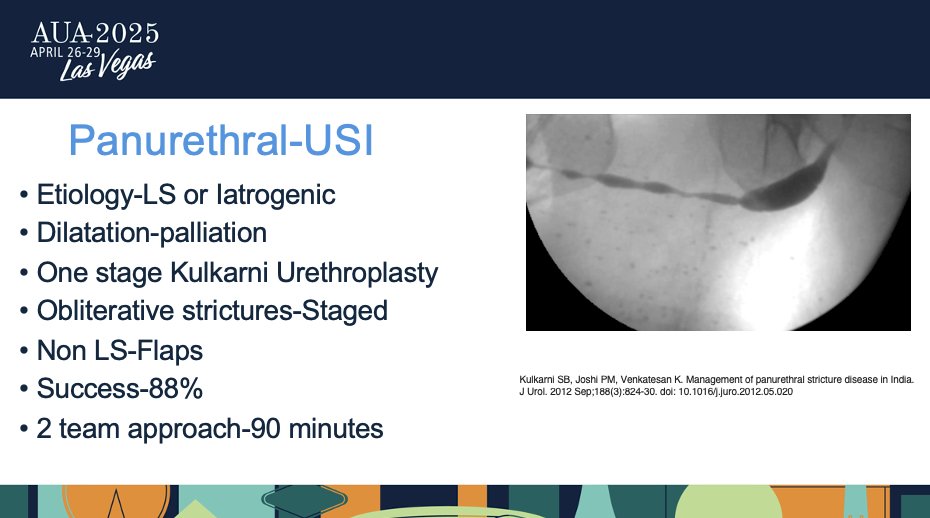
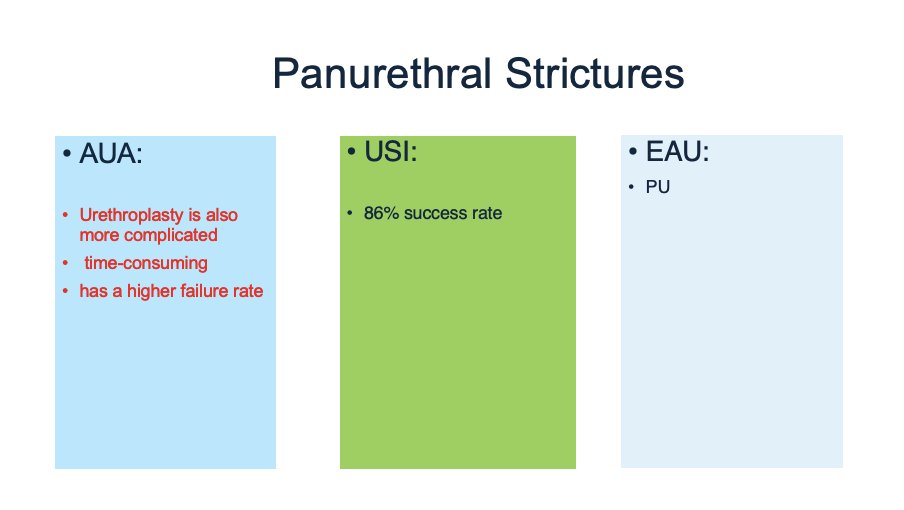
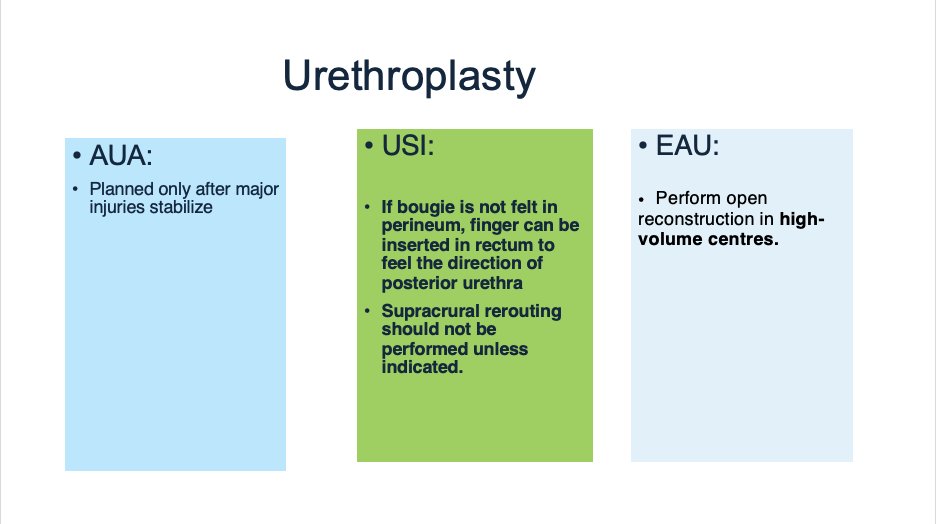
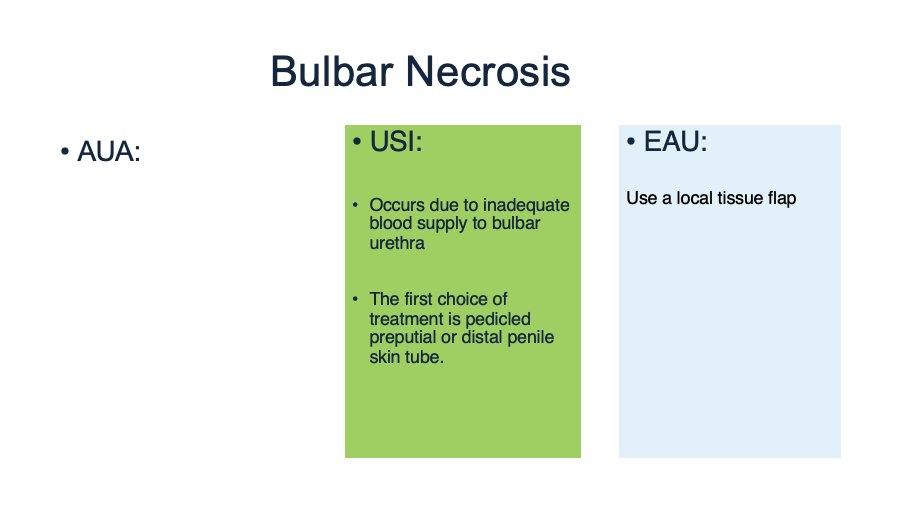
Following Ms. Greenwell, Dr. Pankaj Joshi took the podium to present the USI guidelines. He began by discussing long bulbar strictures, emphasizing that for strictures longer than 2 cm, urethroplasty should be offered as the treatment of choice. Dr. Joshi noted that the USI guidelines favor a single-stage approach for panurethral strictures, with success rates around 88%, particularly when performed in high-volume centers.
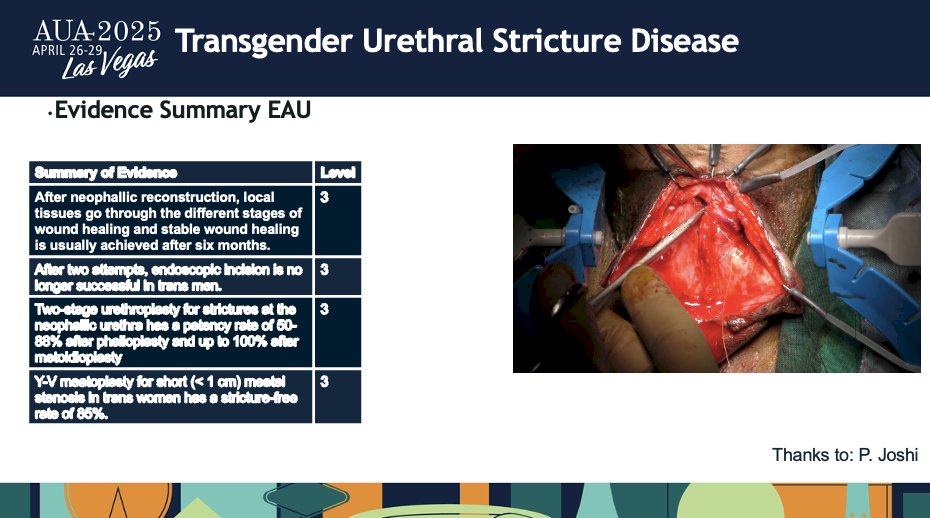
He also focused on transgender urethral stricture disease, explaining that early intervention post-neophalloplasty using dilation or perineostomy is often insufficient, and staged urethroplasty is required for long-term success. In his presentation, Dr. Joshi highlighted the importance of a tailored approach for each patient, taking into consideration factors such as the location of the stricture and patient comorbidities.
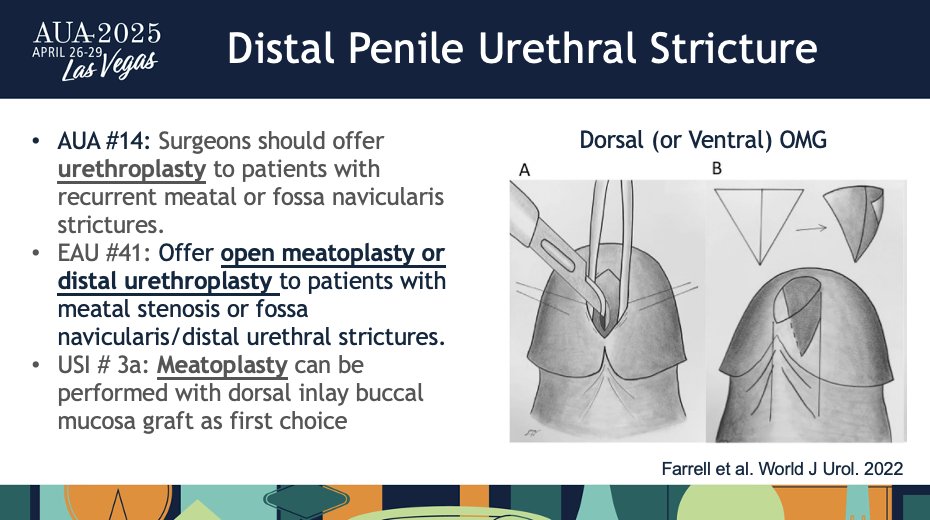
Dr. Hunter Wessells was the final speaker, presenting the AUA guidelines on urethral stricture management. He discussed the treatment of short bulbar strictures, recommending that urethroplasty be offered as the initial treatment for strictures less than 2 cm in length. For recurrent strictures after failed dilation or DVIU, the AUA guidelines advocate for urethroplasty rather than repeated endoscopic procedures, citing success rates of 88-91% for graft and flap approaches in one-stage and multi-stage surgeries.
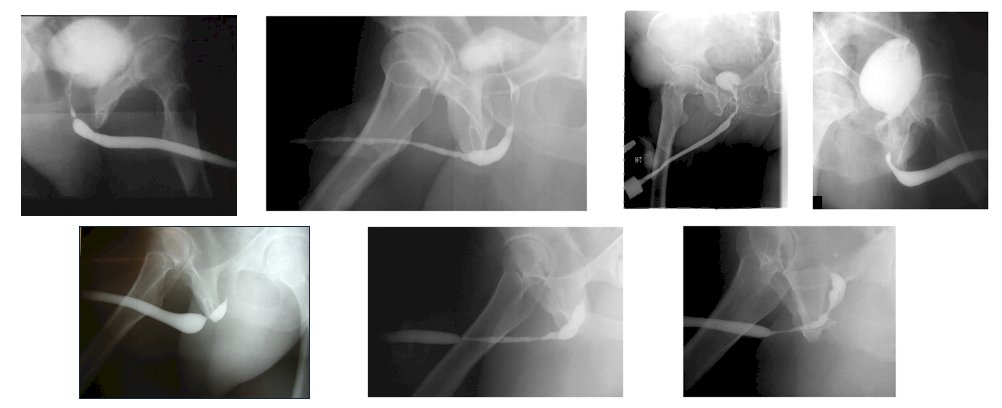
Dr. Wessells also provided insights into the management of panurethral strictures, stating that these complex cases are best handled at high-volume centers where multi-stage procedures can be performed with greater success. He highlighted the importance of using a comprehensive approach that includes imaging studies, such as retrograde urethrogram (RGU) and cystoscopy, to guide treatment decisions.
Each panel debater had a rebuttal prepared for each set of guidelines. Ms. Greenwell took the podium once again to provide her rebuttal first. During her rebuttal, Ms. Greenwell addressed some of the points raised by Dr. Joshi and Dr. Wessells, particularly around the role of perineal urethrostomy. While Dr. Joshi advocated for PU in pan-urethral and radiation-induced strictures, Ms. Greenwell argued that PU should only be considered for specific cases with complex anterior disease, underscoring that surgeon experience plays a critical role in the success of this procedure.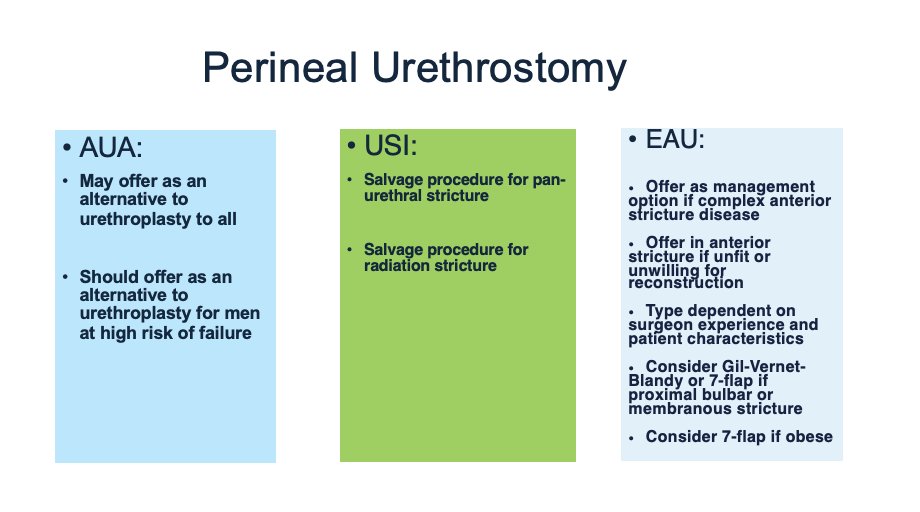

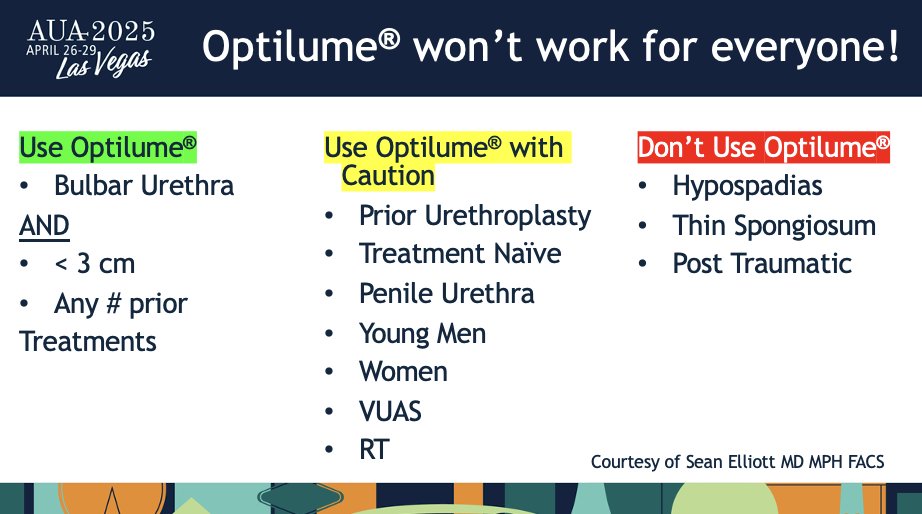
Next, Dr. Joshi took the podium. In his rebuttal, Dr. Joshi responded to Dr. Wessells' endorsement of drug-coated balloon (DCB) therapy for short bulbar strictures. Dr. Joshi pointed out that while DCB offers promising results, particularly in the AUA guidelines, the USI guidelines remain cautious about using DCB in certain patient populations, such as those with post-traumatic strictures or women with hypospadias. He emphasized the need for a more personalized approach, with urethroplasty remaining the gold standard for many patients.
Lastly, Dr. Wessells took the podium to provide his rebuttal. In his rebuttal, Dr. Wessells responded to Dr. Joshi's comments on the use of perineal urethrostomy. While Dr. Joshi recommended PU for panurethral strictures, Dr. Wessells cautioned that PU should be reserved for select cases, particularly those with complex anterior stricture disease or when urethroplasty is not an option. He also addressed the EAU guidelines' reliance on perineal urethrostomy as a management option, suggesting that its use should be more selective, particularly for patients with complex or advanced disease.
Dr. Angermeier took the podium after speakers provided their rebuttals. In his closing remarks, Dr. Angermeier summarized the key takeaways from the session. He noted that while the AUA, EAU, and USI guidelines all offer valuable insights into the management of urethral stricture disease, there are nuanced differences that arise from regional practices and patient populations. He emphasized that urologists should base their treatment decisions on a combination of evidence-based guidelines and their own clinical experience, especially when dealing with complex cases.
Moderated by: Kenneth Angermeier, MD, FACS, Department of Urology, Cleveland Clinic, Cleveland, OH, USA
Expert Panel:- Tamsin Greenwell, Consultant Urologic Surgeon, University College London Hospital, London, England, UK
- Pankaj Joshi, MBBS, Consultant Urologist, UROKUL Hospital, Pune, India
- Hunter Wessells, MD, President of UW Physicians, Professor and Nelson Chiar of Urology, Director of the Genitourinary Trauma and Reconstruction Fellowship, University of Washington, Seattle, WA, USA
Written by: Eman N. Chaudhri, MD, Department of Urology, University of California Irvine, @EmanChaudhri on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025