(UroToday.com) Dr. Banna Hussain presented important new data from the Michigan Urological Surgery Improvement Collaborative (MUSIC), shedding light on the real-world implementation and outcomes of active surveillance (AS) for clinical stage T1b renal masses (T1bRM, 4.1–7.0 cm). Although nephrectomy remains standard of care, this large-scale, multicenter effort evaluated how non-surgical management is being utilized and associated outcomes that are being observed in patients across the state of Michigan.
The study analyzed 1,134 patients diagnosed with T1bRM between May 2017 and June 2024. Patients were stratified by initial management at 90 days post-diagnosis: 837 (74%) received immediate treatment, while 297 (26%) were started on AS. The analysis aimed to identify predictors of AS utilization, assess survival and metastasis rates, and track delayed interventions (DI).
Multivariable modeling revealed that patients with higher Charlson comorbidity indices (≥2), non-solid masses (e.g., Bosniak III/IV cysts), indeterminate imaging, or benign biopsy results were significantly more likely to undergo AS. Particularly striking was the 22-fold increase in likelihood of AS in patients with benign pathology on renal mass biopsy (OR 22.2, p < 0.001).
Cohort characteristics revealed that AS patients were older (median 73 vs. 64 years), had smaller tumors, higher comorbidity burdens, and lower preoperative glomerular filtration rates (GFR).
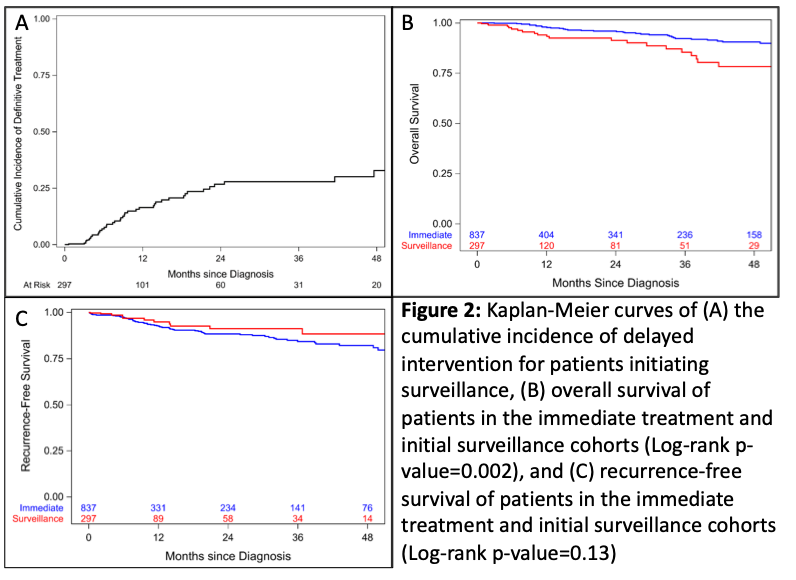
The cumulative incidence of delayed intervention reached 27% at two years, as estimated by Kaplan-Meier analysis. Of the 297 patients who initially chose AS, 21 died during surveillance, including 2 deaths attributed to kidney cancer. Additionally, 5 patients developed confirmed metastatic RCC (Figure 1). Importantly, overall survival remained high: 98% at one year and 92% at three years post-AS initiation.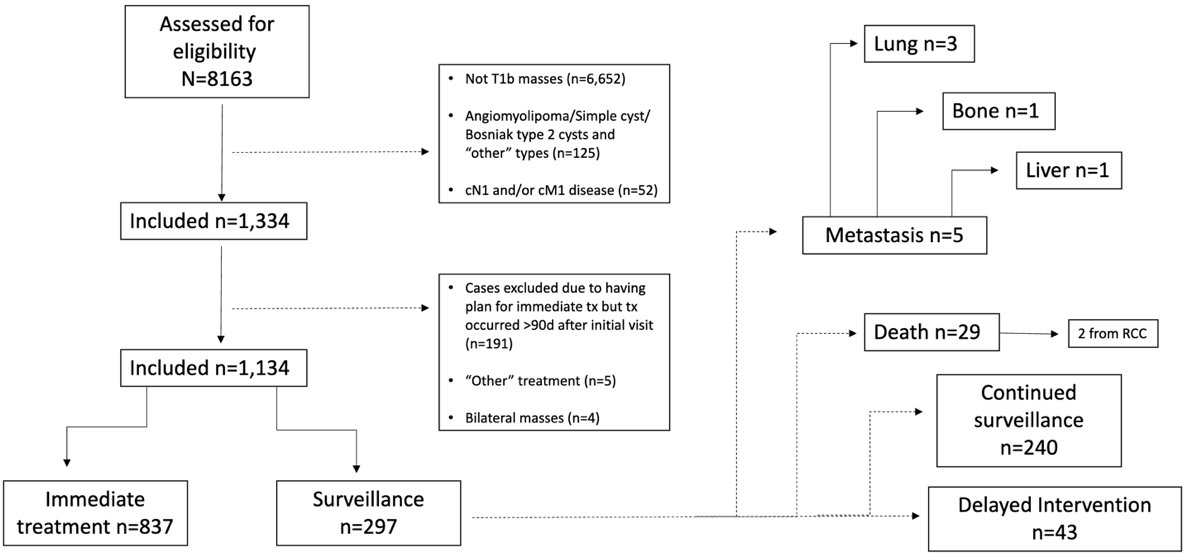
Figure 1: Flow diagram depicting fate of patients on AS during 5 years of follow-up
When compared to immediate surgical intervention, AS was not associated with increased all-cause mortality (HR 1.23, p = 0.5). Age emerged as the only significant independent predictor of mortality (HR 1.06, p<0.001).
Kaplan-Meier analysis showed a statistically significant difference in overall survival favoring immediate treatment (log-rank p = 0.002), though recurrence-free survival did not differ significantly between groups (log-rank p = 0.13), supporting the oncologic safety of AS in select patients (Figure 2).
 Dr. Hussain emphasized that MUSIC’s real-world, collaborative data supports active surveillance as a viable and safe option for select patients with T1bRM, especially those with significant comorbidities or imaging/biopsy features suggesting lower malignant potential. This data may shift the paradigm toward more individualized care, especially in patients for whom surgery may pose substantial risk.
Dr. Hussain emphasized that MUSIC’s real-world, collaborative data supports active surveillance as a viable and safe option for select patients with T1bRM, especially those with significant comorbidities or imaging/biopsy features suggesting lower malignant potential. This data may shift the paradigm toward more individualized care, especially in patients for whom surgery may pose substantial risk.
Practice-level analysis revealed significant variability in AS utilization. Among 14 MUSIC practices with at least 10 qualifying cases, surveillance rates ranged from 6.7% to 47% (Chi-square p < 0.001), highlighting institutional differences in adoption. Bubble plot visualization showed case volume differences across practices, with larger circles indicating higher case volume (Figure 3).
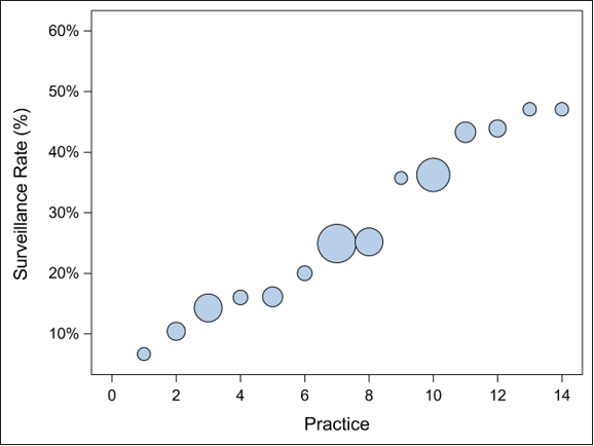
Figure 3: Practice-level variation of the rate of initiation of AS for T1bRM. Each circle represents one of the 14 MUSIC practices (of 24 in the sample) with 10+ cases; the size of each circle correlates with the number of included cases. AS rate differed significantly by practice (p < 0.001 via Chi-square test), ranging from 6.7% to 47%.
Dr. Hussain concluded that surveillance is a safe and feasible option, particularly in older patients, those with smaller tumors, higher comorbidities, and lower GFR. The team hopes to further validate these findings with longer follow-up and more granular oncologic outcomes.
During the post-presentation discussion, a key question from the audience centered on the distinction between true active surveillance (AS) and watchful waiting or observational management. Dr. Hussain acknowledged that this differentiation is indeed important, especially given that earlier studies may have overestimated metastasis rates due to the inclusion of patients under observational management rather than structured AS. Since the submission of the abstract, the authors have updated their terminology to more accurately reflect the cohort as “watchful waiting” rather than strict active surveillance, due to the absence of standardized protocols for planned delayed intervention.
Another attendee inquired about the potential benefit of AS in younger patients with comorbidities. Dr. Hussain responded that while their dataset reflects that older patients tend to benefit more from surveillance, younger patients were not specifically evaluated in this study, and future analyses could explore that subgroup. Finally, a question from Dr. Daneshvar from the moderator table prompted a discussion between Dr. Hussain and Dr. Rodgers (also from Henry Ford) about the role of renal mass biopsy in surveillance planning, highlighting institutional variability and the need to consider biopsy data when stratifying patients and designing future protocols.
Presented by: Banna Hussain, Henry Ford Health, during the 2025 American Urological Association (AUA) Annual Meeting, April 26-29, 2025, Las Vegas, Nevada
Co-Authors: Yuzhi Wang, Brian R. Lane, Sami Wilder, Mohit Butaney, Monica Van Til, Mahin Mirza, Abena Osei, Elnaz Guivatchian, Junzhi Sun, Stephanie Daignault-Newton, Alice Semerjian, Craig G. Rogers, and Amit K. Patel
Moderated by: Michael Daneshvar (University of California, Irvine), John Lam (Kaiser Permanente-Southern California)
Written by: Seyed Amiryaghoub M. Lavasani, B.A., University of California, Irvine, @amirlavasani_ on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.