(UroToday.com) Dr. Alice Pitout and colleagues from Bordeaux and Clermont-Ferrand, France, presented their investigation into the training of a neural network (NN) for the identification of renal parenchyma, for the eventual application into augmented reality (AR) for robotic-assisted partial nephrectomy (RAPN). Currently, their institution has incorporated 3D preoperative models for surgical planning and virtual reality. These have proven to be beneficial, namely in improving patient experience with regard to their understanding of pathology and surgical treatment1. Herein, they are developing an AR software to project and superimpose the 3D models onto the surgical field in real time.
Indeed, AR integration into RAPN remains a complicated process that requires the automated recognition of the renal parenchyma by an NN (Figure 1). Such a model must be trained via a substantial database of surgical images, which further demands a time-consuming effort that may be delegated to non-surgeon annotators. To this end, Dr. Pitout et al. sought to quantitatively assess the reliability of non-physician segmentations in comparison to physician evaluations. Their work was funded by a French national research agency (ANR) grant under the third investment program for the future (PIA).
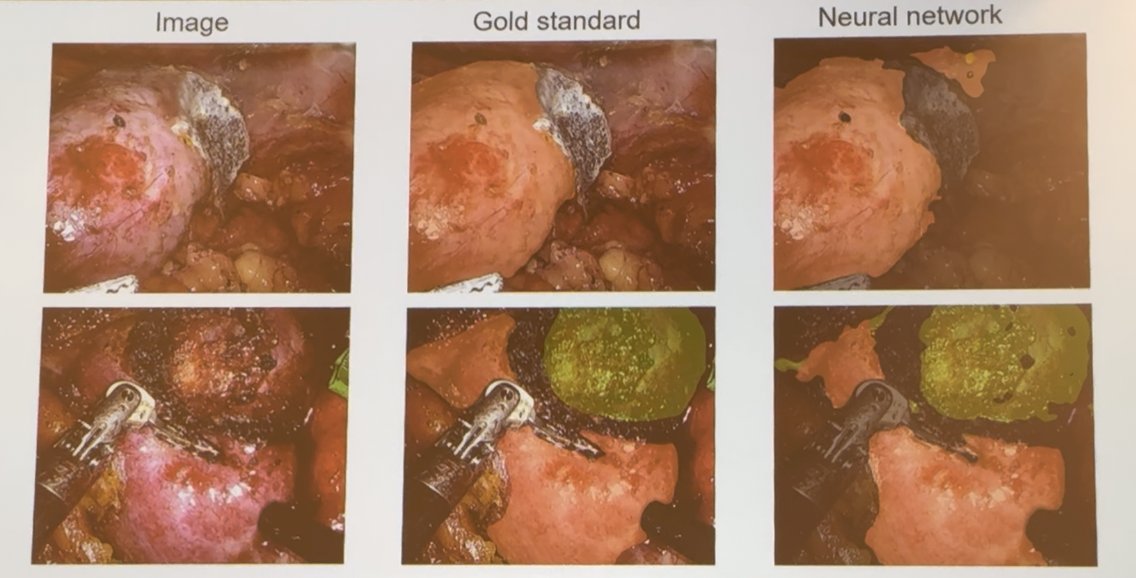
Figure 1: Provided example of trained NN with recognition of the parenchymal region.
A dataset of 47,956 images was composed based on 51 RAPN surgical videos. A subset of 9 surgeries was curated for detailed review by a physician evaluator via performance of image-by-image corrections of non-medical segmentations. Across surgical phases, further categories were created among renal dissection, dissection of the hilum, tumor dissection, tumorectomy, and reconstruction.
Among 5459 images, the mean proportion of correctly segmented images was 69.83% (IQR 51.01-78.39%). Moreover, two surgeries within the sample achieved greater than 80% correctness, an optimal threshold. When stratified by surgical phase, renal dissection showed the highest segmentation reliability with 95.3% (±5.96) correct labeling, and the second highest in the reconstruction phase with 78.14% (±25.86). However, tumor dissection and tumorectomy phases had lower accuracy rates, 61.61% (±28.61) and 64.66% (±31.60), respectively. Most challenging proved to be hilum dissection for non-physician annotators, with a lowered 54% correctness rate (Table 1).

Such work underscores the feasibility of building neural network training datasets through non-physician annotators, albeit with important variability depending on the surgical phase.
Dr. Pitout concluded her study with the following statements:
- Segmentation quality by trained non-physician annotators is reliable but varies across surgical phases, further highlighting the need for improved accuracy during more challenging surgical phases.
- Segmentation is a time-consuming task that may be delegated to a non-physician reviewer, though currently, medical evaluation remains essential prior to AR application in RAPN.
Following her presentation, Dr. Li-Ming Su, University of Florida College of Medicine, inquired about the use of non-physician annotators and their role in the study. Dr. Pitout explained that due to the time constraints on physicians, annotation tasks were outsourced to trained non-medical personnel. These annotators underwent a training and correction process. She also clarified that all segmentations were performed based on surgical video footage, not radiographic imaging. Dr. Su noted that it may still be valuable to involve individuals with clinical background knowledge in the segmentation process.
Dr. Jaya Sai Chavali, Medical University of South Carolina, asked whether tumor complexity or patient characteristics influenced segmentation errors. Dr. Pitout and her colleague acknowledged this as a challenge and emphasized that such variability would be difficult to account for, even for physicians. Nonetheless, the current dataset appears promising for training their neural network.
Finally, Dr. William Hung (NYU Urology Associates) raised a question about improving overall segmentation accuracy. Dr. Pitout responded that future strategies would include refining annotator training and increasing the diversity of surgeries included in the dataset.
Presented by: Alice Pitout, MD, Bordeaux, FranceWritten by: Mariah Hernandez, Research Specialist, Department of Urology, University of California Irvine, @mariahch00 on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
References: