(UroToday.com) Dr. Lucshman Raveendran from the University of Toronto presented a comprehensive review of a 20-year single-center experience evaluating the diagnostic performance and clinical utility of renal mass biopsy (RMB) for small renal masses (SRMs).
In this retrospective review, Dr. Raveendran and his colleagues analyzed patients who underwent RMB for SRMs (≤4 cm) between 2001 and 2023. Biopsies were performed by experienced interventional radiologists using a coaxial technique, with centralized genitourinary pathology review for consistency. Patient demographics, imaging characteristics, histopathological findings, and final surgical pathology were collected. Diagnostic accuracy was determined by comparing RMB histology with surgical pathology, where available.
A total of 1,482 SRMs were biopsied during the study period (Figure 1). The median patient age was 63.5 years (IQR 55.6–71.7), with a median tumor size of 2.4 cm (IQR 1.8–3.1 cm). The cohort was 64.9% male. The first-pass diagnostic rate was 89.1%, improving to 93.1% after a second biopsy attempt. Notably, tumor size was strongly associated with diagnostic success (OR 1.98, p<0.001).

Figure 1.
Histopathologic results revealed that 68% of SRMs were malignant, 21.3% were benign, and 10.9% were non-diagnostic. Among benign diagnoses, oncocytoma (71.8%) and angiomyolipoma (15.2%) were most common (Figure 2). For malignant tumors, clear cell RCC (60%), papillary RCC (23%), and chromophobe RCC (7.4%) predominated (Figure 3).
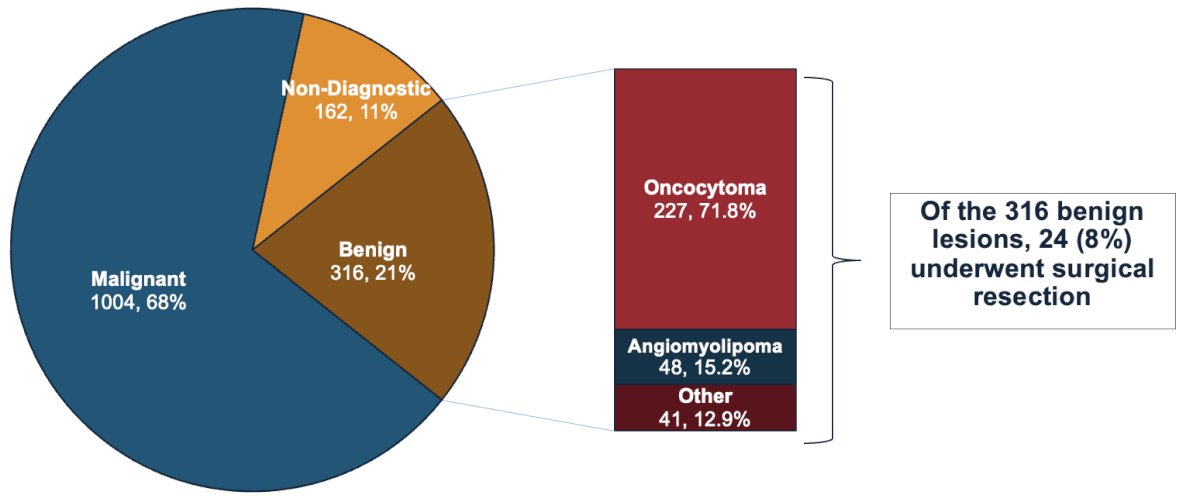
Figure 2.
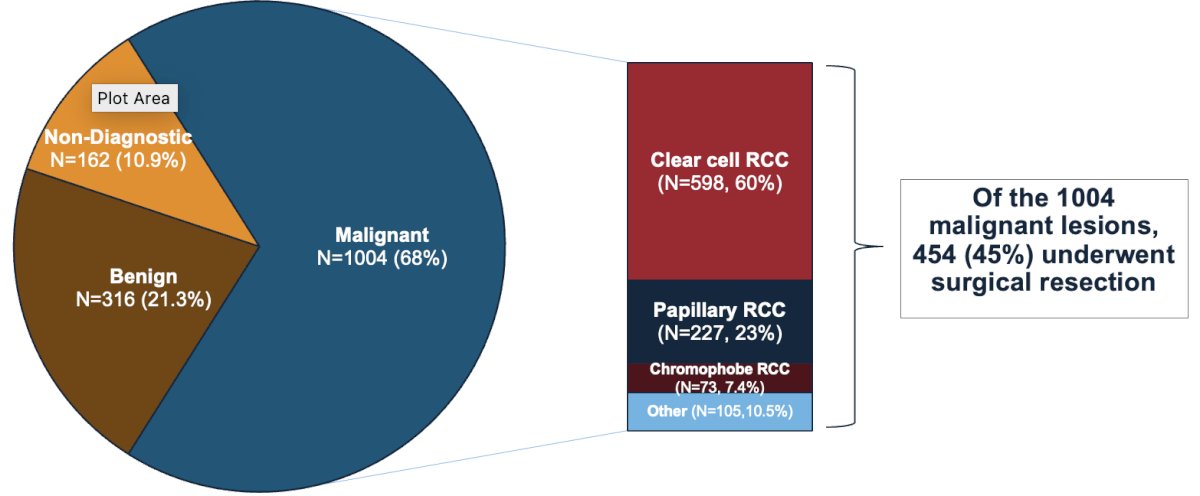
Figure 3.
Of the 1,004 malignant lesions, 454 patients (45%) proceeded to surgical resection. Malignant concordance between biopsy and surgical pathology was high, with clear cell RCC demonstrating ≈99% concordance (Figure 4).
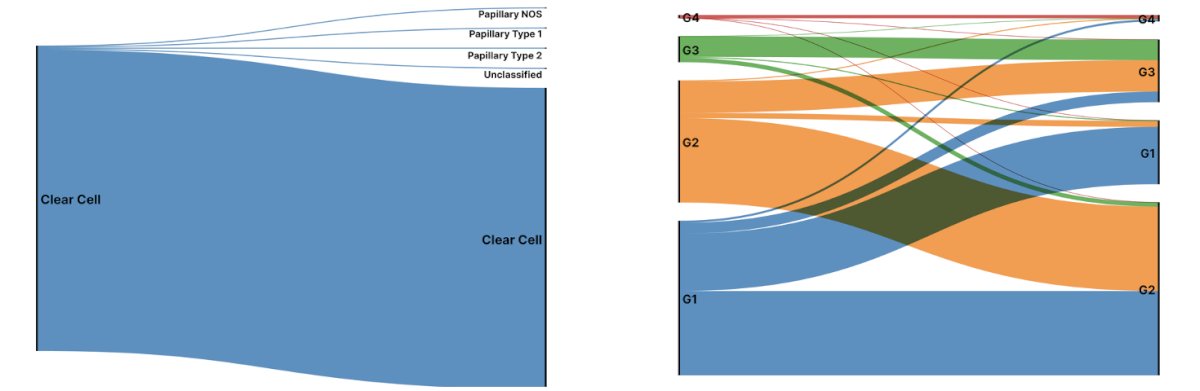
Figure 4.
Chromophobe RCC and papillary RCC showed slightly lower subtype concordance rates of approximately 83% and 72%, respectively (Figures 5 and 6).
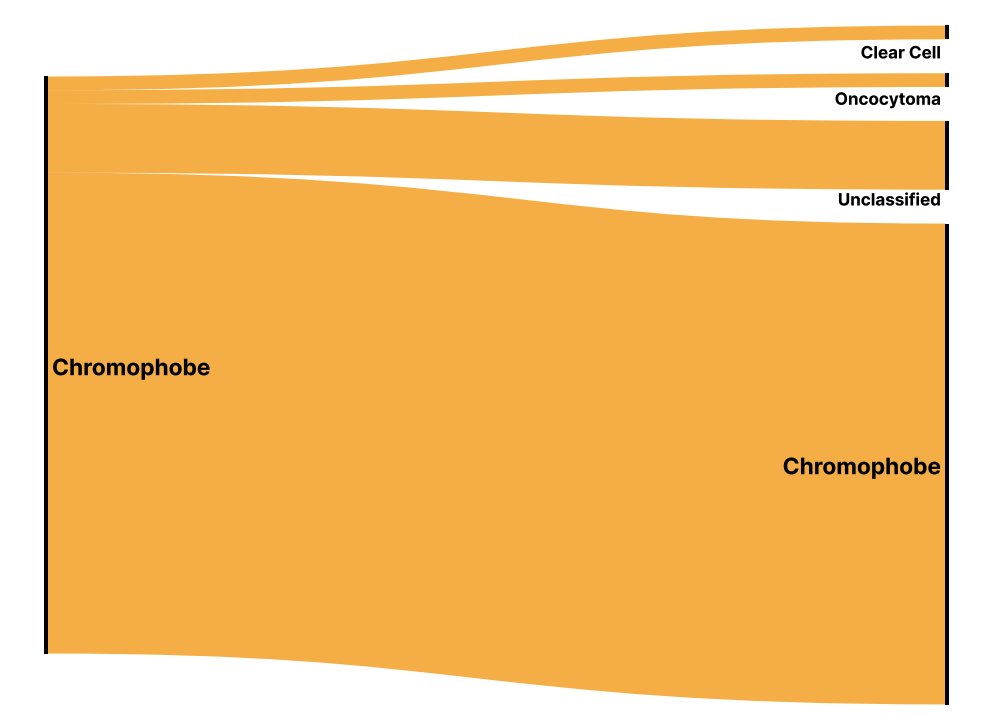
Figure 5.
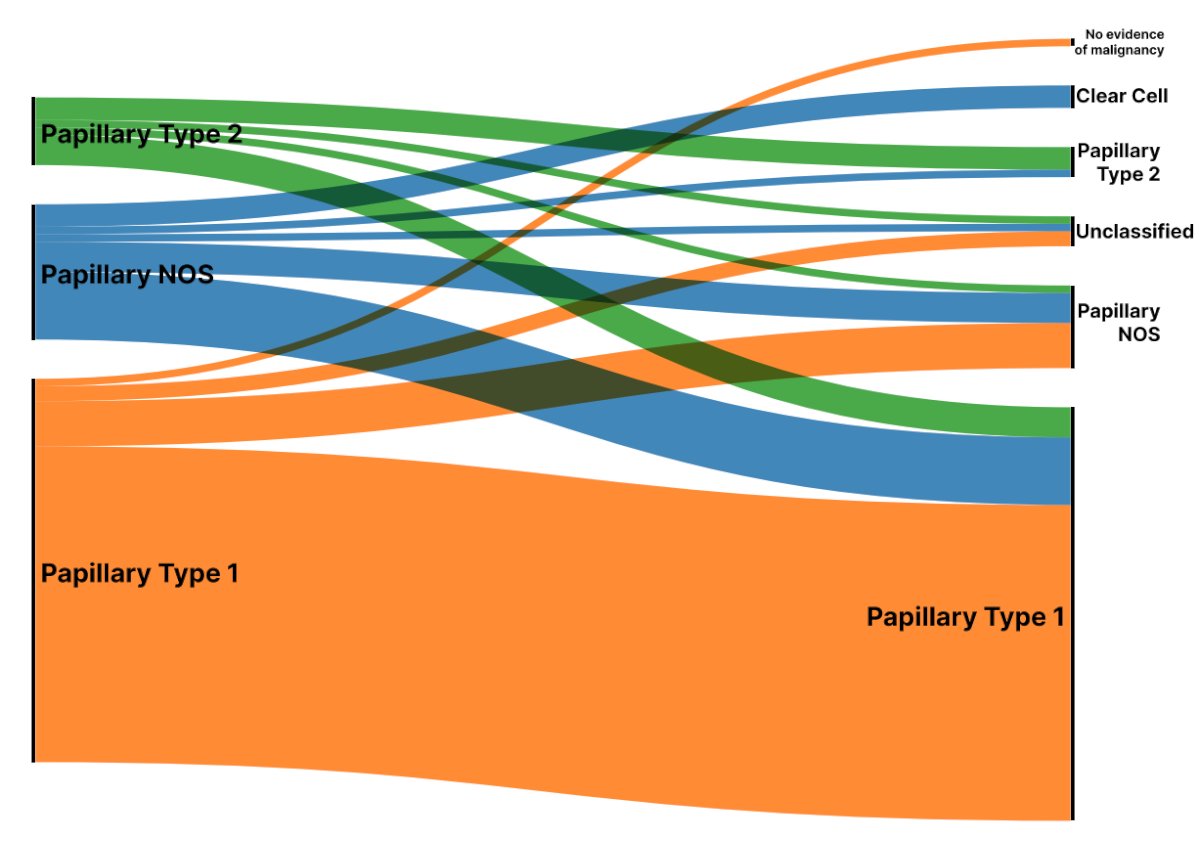
Figure 6.
Among 24 surgically resected benign lesions, five (20.8%) were found to harbor malignant histology on final pathology, representing 1.6% of the total benign biopsy cohort. Dr. Raveendran noted that they included eosinophilic RCC, chromophobe RCC, and unclassified RCC. These discordant cases were often identified through interval imaging changes such as rapid growth, increased lesion heterogeneity, or development of new tumor thrombus (Figures 7 and 8). Notably, some discordant cases required re-biopsy due to suspicious progression before surgical intervention.
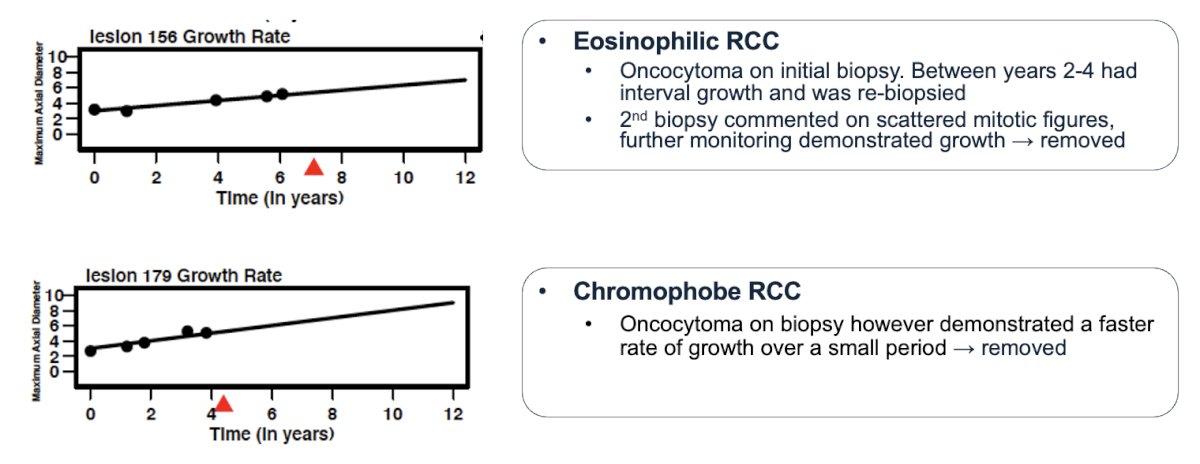
Figure 7.
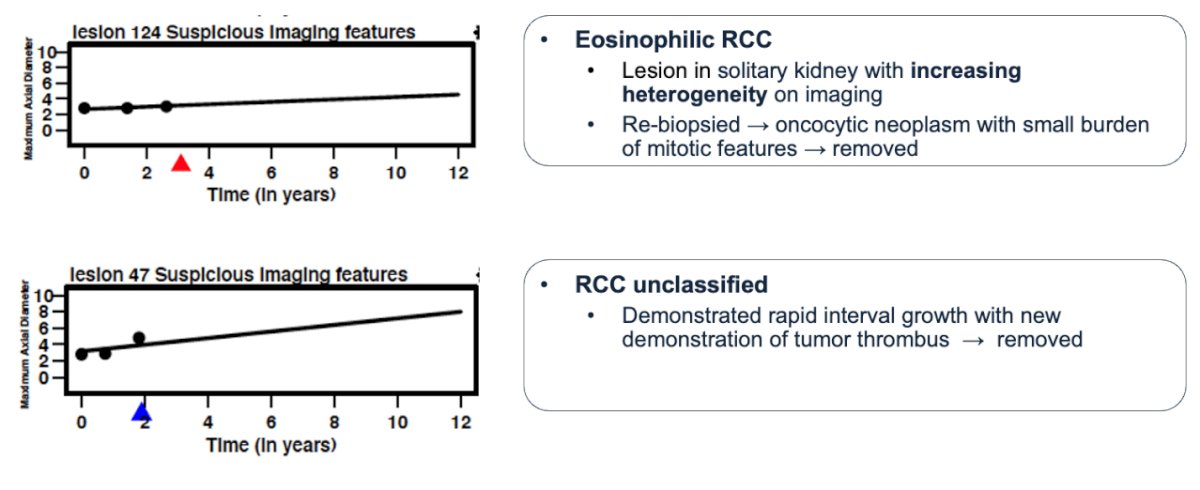
Figure 8.
Ultimately, Dr. Raveendran concluded that RMB demonstrated a high diagnostic yield (89–93%), strong concordance with final pathology for malignant lesions, and a meaningful ability to detect benign disease, potentially reducing unnecessary interventions.
During the Q&A session, Dr. Raveendran addressed several important audience questions regarding RMB's evolving role in SRM management.
One audience member asked about the indications for biopsy and how often RMB results influence clinical management. Dr. Raveendran explained that they do not routinely biopsy all SRMs; rather, biopsy is discussed and performed if it is deemed helpful after shared decision-making. He noted that this cohort was focused on surgical numbers, and the study did not specifically evaluate how biopsy results changed management. However, he highlighted that approximately 50% of patients underwent surgery after biopsy, while the other 50% were managed with surveillance or minimally invasive treatment. He agreed that future analysis on the clinical impact of RMB findings would be a valuable area for exploration.
The discussion then shifted when Dr. J. Stuart Wolf from the moderator table complimented the study, suggesting that it would be interesting to analyze whether diagnostic accuracy and pathology concordance have improved over time. Dr. Raveendran agreed, emphasizing that a time-based analysis would be insightful given changes in pathology classifications and clinical practice over the past two decades.
Concerns about tumor seeding were also raised by the audience, a common fear among patients considering RMB. Dr. Raveendran acknowledged that while theoretical risk exists, it remains extremely rare. In their experience, RMB complication rates were approximately 2–4%, with 80% being Grade 1 events. Only two cases demonstrated 2–3 mm extension beyond the surgical capsule along the biopsy tract, but these did not result in adverse clinical outcomes. Moreover, rates of pathological upstaging to pT3 disease were not significantly affected by prior biopsy. Dr. Raveendran also noted that an upcoming manuscript will further detail their findings on complications and tumor seeding risk.
Moderated by: Ithaar Derweesh (UC San Diego School of Medicine), Rahul Bansal (Division of Urology, McMaster University), J. Stuart Wolf (Dell Medical School, University of Texas at Austin).
Presented by: Lucshman Raveendran, MD, MSc, PGY- 4 Urology, University of Toronto
Written by: Tiffany Huang, MS3, University of California Irvine School of Medicine, @tiffvnyhuang on X during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025