(UroToday.com) The 2025 AUA annual meeting featured a kidney cancer session and a presentation by Dr. Toshio Takagi discussing the impact of cytoreductive nephrectomy on immune checkpoint inhibitor therapy. Although the treatment outcomes of metastatic renal cell carcinoma (RCC) have improved since the initiation of immune checkpoint inhibitory therapy, the best treatment methods, including surgical removal of the primary site and appropriate systemic therapies, remain unclear. This study presented at the AUA 2025 annual meeting compared treatment outcomes between ipilimumab plus nivolumab (IO + IO) and immune checkpoint inhibitor plus tyrosine kinase inhibitor (IO + TKI) therapies and examined the impact of cytoreductive nephrectomy for metastatic RCC with primary kidney tumors from Japanese institutions.
The study included 104 patients treated with metastatic RCC with primary kidney tumors between January 2019 and December 2024 from 5 Japanese institutions. Patients were treated with either ipilimumab + nivolumab (IO + IO) or IO + TKI therapy. The timing of cytoreductive nephrectomy was classified as upfront (cytoreductive nephrectomy before systemic therapy), deferred (cytoreductive nephrectomy after systemic therapy), or no cytoreductive nephrectomy. The primary outcome was the comparison of treatment outcomes between IO + IO and IO + TKI therapies. A secondary outcome was the effect of cytoreductive nephrectomy timing on overall survival.
Of the 104 patients, 42 (40%) and 62 (60%) were treated with IO + IO and IO + TKI therapies, respectively. Patients treated with IO + IO were significantly younger than those treated with IO + TKI (63 years versus 68 years, p = 0.033). Other factors, such as IMDC risk group, pathological findings, and metastatic site, were not significantly different:
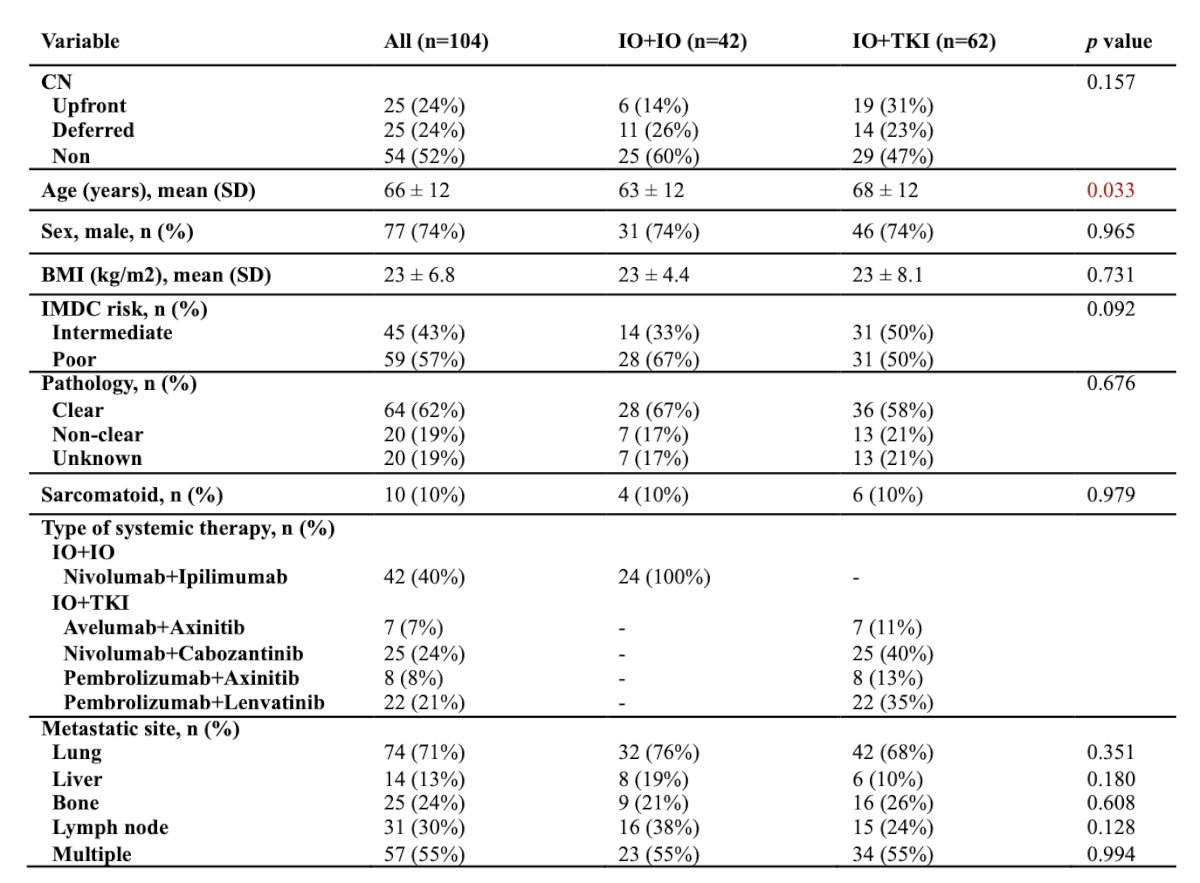
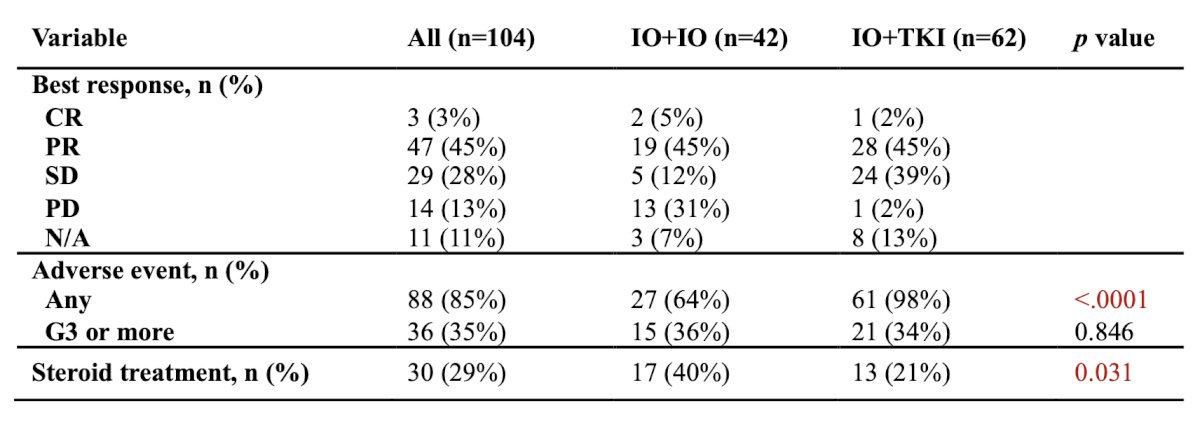
The best objective response was similar in both groups (50% and 47% in the IO + IO and IO + TKI groups, respectively). However, progressive disease tended to be more frequent in the IO + IO group (31%) than in the IO + TKI group (2%):
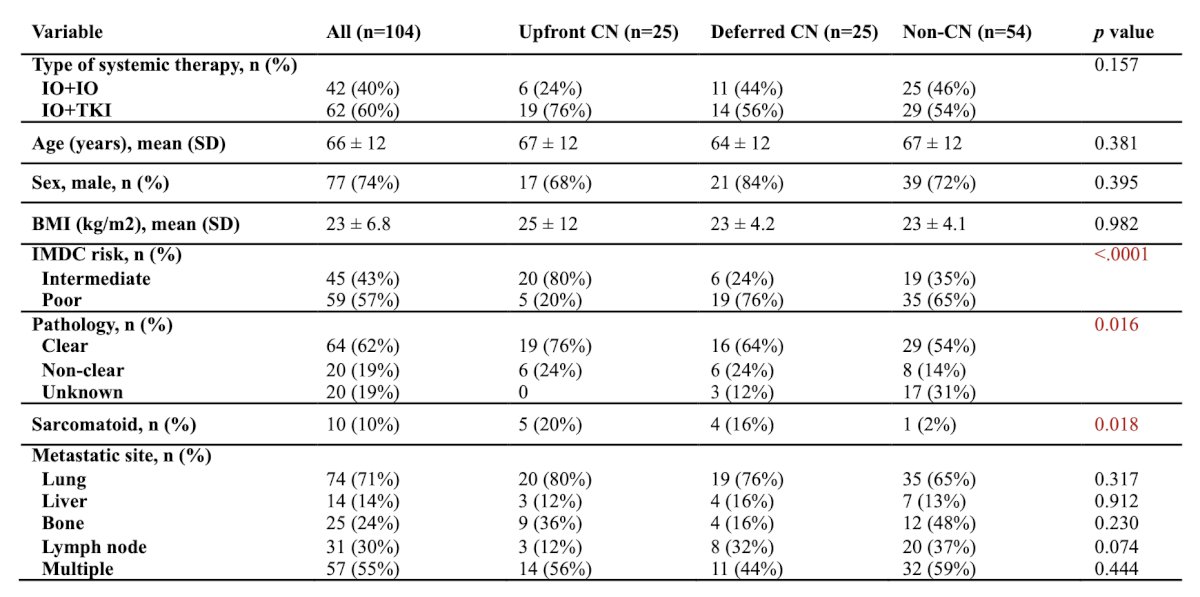
Of the 104 patients, 25 (24%) underwent upfront cytoreductive nephrectomy, 25 (24%) underwent deferred cytoreductive nephrectomy, and 54 (52%) did not undergo a cytoreductive nephrectomy:
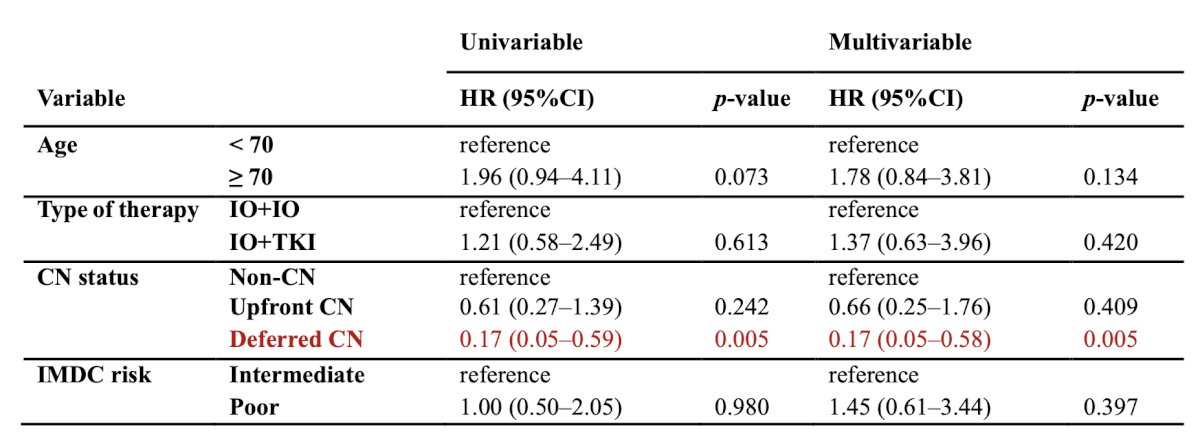
Multivariable analysis showed that deferred cytoreductive nephrectomy was an independent predictive factor for overall survival (versus no cytoreductive nephrectomy, HR 0.17, 95% CI 0.05–0.58), however the type of combination therapy did not show any significance:
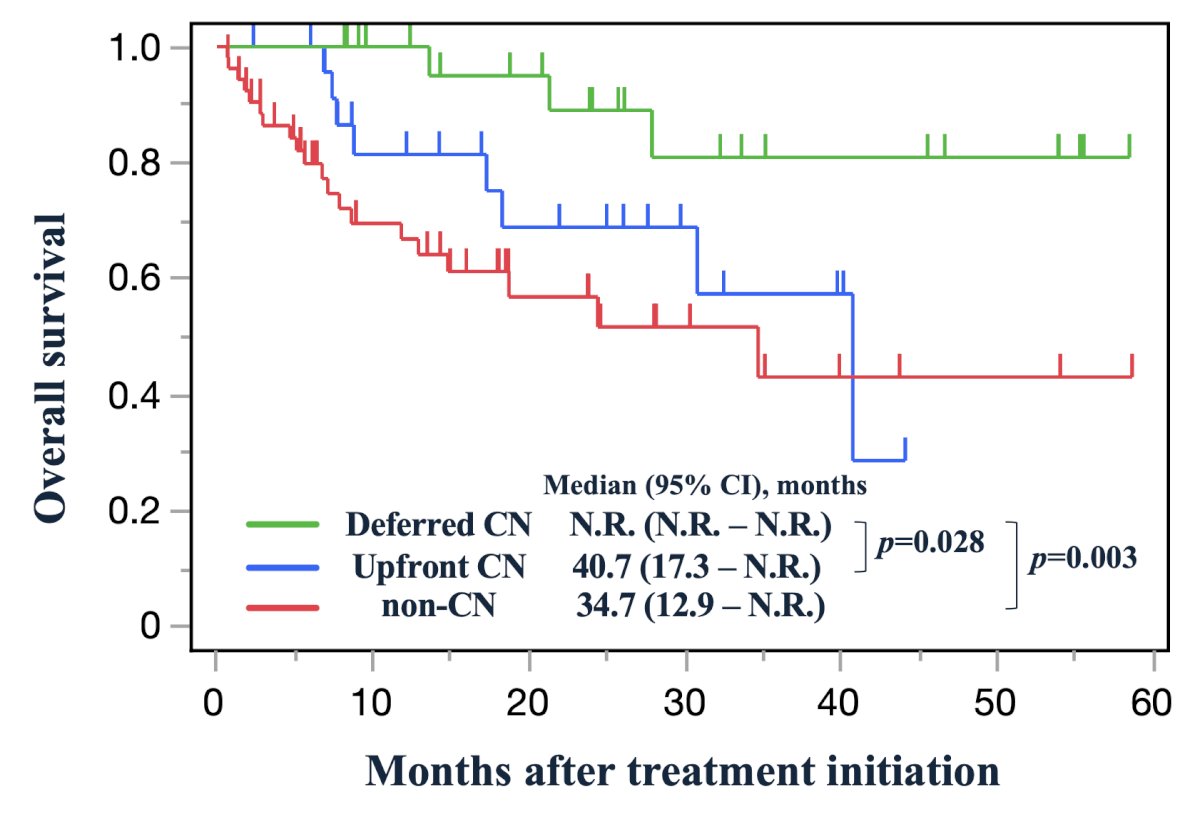
Kaplan Meier analysis demonstrated significantly better overall survival in the deferred cytoreductive nephrectomy group compared to upfront cytoreductive nephrectomy group (median OS: not reached versus 40.7 months, p = 0.028), and no cytoreductive nephrectomy group (median OS: not reached versus 34.7 months, p = 0.003):
Although adverse events of any grade were observed more frequently in the IO + TKI group (98%) than in the IO+TKI group (64%), those requiring steroid replacement therapy occurred more frequently in the IO + IO group (40%) than in the IO + TKI group (21%).
Dr. Takagi concluded his presentation discussing the impact of cytoreductive nephrectomy on immune checkpoint inhibitor therapy with the following take home points:
- IO + IO and IO + TKI therapies showed comparable outcomes for metastatic RCC with primary tumors, although different features, such as more frequent rate of progressive disease in IO + IO and more adverse event in IO + TKI, were observed
- Deferred cytoreductive nephrectomy was an independent predictor for overall survival
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025