(UroToday.com) The 2025 AUA annual meeting featured a kidney cancer session and a presentation by Dr. Keita Tamura discussing a Tokai Urologic Oncology Research Study (TOURS) database study assessing combination of tyrosine kinase inhibitors (TKIs) with immunotherapy (IO) versus dual combination IO as first-line treatment for patients with advanced renal cell carcinoma (RCC). Therapeutic agents for advanced RCC have dramatically developed in recent years, however, it can be difficult to decide which treatment option is better in patients with advanced RCC. The objective of this study, presented at the AUA 2025 annual meeting, was to compare oncological outcomes between advanced RCC patients receiving the combinations of TKI with IO agents (IO-TKI group) versus dual combination IO agents (IO-IO group) as first line treatment.
This retrospective study included 416 consecutive patients with intermediate- and poor-risk advanced RCC according to the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC). These patients received IO-TKI or IO-IO at four institutions participating in the TUORS Group, and were comparatively analyzed for oncological outcomes and safety between the two groups.
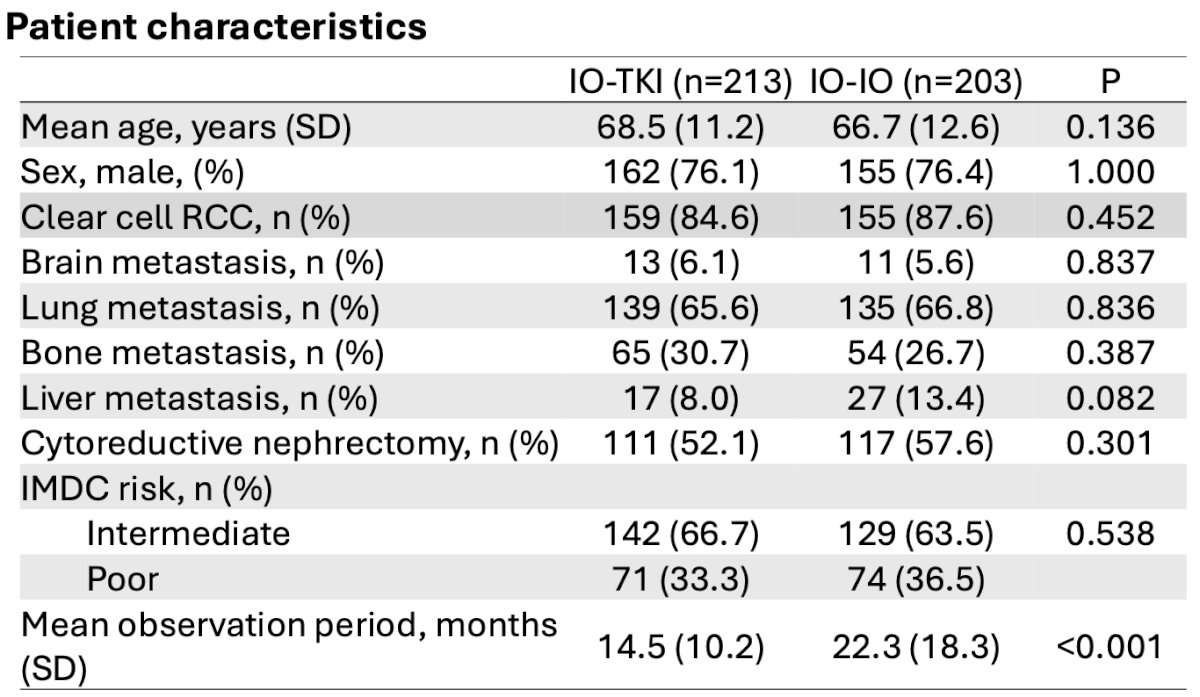
The advanced RCC patients consisted of 213 and 203 who received IO-TKI and IO-IO treatment, respectively. The number of intermediate risk groups was 142 (66.7%) / 129 (63.5%) in the IO-TKI / IO-IO groups, respectively, and the majority of patients had clear cell RCC (84.6% versus 87.6%):
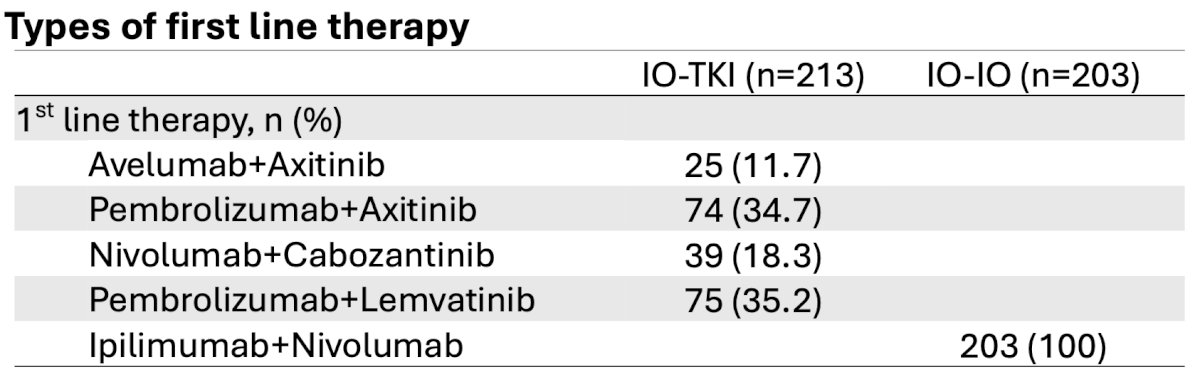
The most common first line therapy for the IO-TKI group was pembrolizumab + lenvatinib (35.2%) followed by pembrolizumab + axitinib (34.7%):
Treatment outcomes showed a significantly higher objective response rate in the IO-TKI group compared with the IO-IO group (65.7% versus 43.1%, p < 0.01) and a lower progressive disease rate (6.6% versus 21.3%, p < 0.01), respectively:

Median progression free survival and overall survival in the therapeutic groups (IO-TKI vs IO-IO) were 16.9 versus 8.6 months (HR 0.54; p < 0.01) and not reached versus not reached (HR 0.61; p = 0.02):

Despite the lack of significant difference in severe adverse events between the two groups (48.0% versus 39.8%, p = 0.075), immune-rerated adverse events in the IO-TKI group were significantly lower than those in the IO-IO group (37.6% versus 63.5%, p < 0.01):

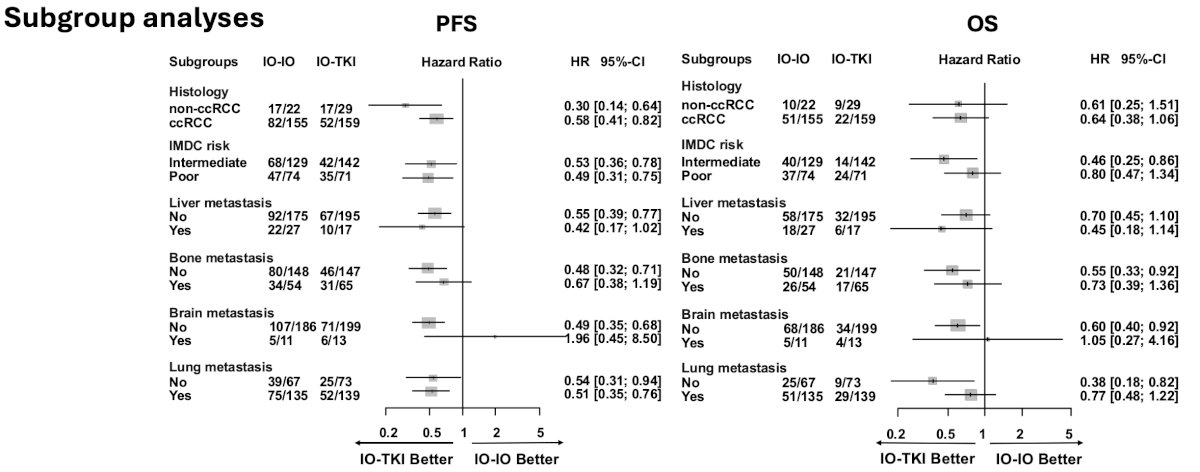
Subgroup analysis regarding progression free survival showed that IO-TKI therapy favored patients with any histology, lung metastasis, and IMDC risk classification, without liver, bone or brain metastases:
Dr. Tamura concluded this presentation, stating that these findings suggest that IO-TKI group showed significantly superior progression free survival and overall survival compared to IO-IO group, demonstrating the advantage of IO-TKI combination therapy in the real-world setting.
Presented by: Keita Tamura, Hamamatsu University School of Medicine, Hamamatsu, JapanWritten by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025