(UroToday.com) Dr. Riemer Kingma and colleagues from Groningen, Netherlands, presented findings from a randomized controlled trial evaluating intraoperative cone beam computed tomography (CBCT) during percutaneous nephrolithotomy (PCNL). Previously, Dr. Kingma and colleagues completed a retrospective cohort study for patients undergoing PCNL between 2015 and 2020. CT scans were obtained and used to assess stone-free status.
Overall, their findings demonstrated fully stone-free status in only 29.4% of patients, with 58.8% having residual fragments ≤4 mm, and 71.4% having fragments >4 mm. These findings highlight a clear need for improved intraoperative detection methods to prevent future stone-related events (SREs)1.
Given that non-contrast computed tomography (NCCT) is considered the gold standard for stone evaluation, Dr. Kingma discussed the potential of adapting CT imaging for intraoperative use. Unlike conventional CT, which requires a full 360-degree rotation and is impractical for surgery, CBCT utilizes a C-arm design with 200–250 degrees of coverage, making it feasible for real-time intraoperative imaging (Figure 1). As such, Dr. Kingma and his team investigated the impact of the detection of residual fragments via utilization of intraoperative CBCT to enhance stone-free rates and reduce long-term stone-related events.

Figure 1: Intraoperative application of CBCT during PCNL.
Dr. Kingma et al. conducted a prospective randomized controlled trial for patients undergoing PCNL. Individuals were enrolled at a tertiary referral center and randomized intraoperatively, following surgeon determination of endoscopic stone-free status. Participants were assigned either to receive an intraoperative CBCT scan while the control group proceed without additional imaging. The CBCT scan was completed in an estimated 6 seconds. Individuals in the CBCT arm had any newly detected residual fragments addressed immediately during the same procedure and removed (Figure 2). NCCT imaging was completed postoperatively at 4 weeks and 1 year. Stone-free status (SFR) is defined by the absence of fragments larger than 4 mm. Additional follow-up over one year captured stone-related events, including reinterventions, symptom recurrence, hospitalizations, and emergency room visits.

Figure 2: CBCT Depiction of residual stone during PCNL.
Among the 154 patients, SFR at four weeks was significantly higher in the CBCT group compared to controls (80% vs 62%, p = 0.01). Long-term follow-up data were available for 133 patients. At one year, the CBCT group had significantly fewer stone-related events (17% vs 35%, p = 0.02) and symptom recurrences (6% vs 19%, p = 0.02) compared to the control group. Although reintervention rates were lower in the CBCT group (8% vs 15%), this difference did not reach statistical significance (p = 0.2) (Figure 3).
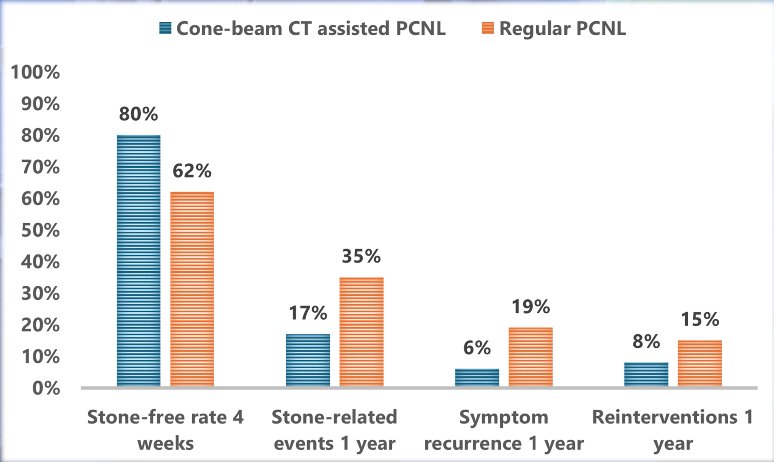
Figure 3: Comparison of stone-free, stone-related events, symptom recurrence, and reinterventions between CBCT and standard PCNL.
One year after surgery, the use of intraoperative CBCT during PCNL significantly improved stone-free rates and reduced the incidence of stone-related morbidity. These findings support the integration of intraoperative imaging to optimize surgical outcomes, particularly in complex or high-stone-burden cases.
Dr. Kingma and colleagues concluded that:
- Intraoperative CBCT during PCNL significantly improves early stone-free rates.
- Patients in the CBCT group experienced lower rates of stone-related events and symptom recurrence at one year.
- Immediate identification and removal of residual fragments during the primary procedure may optimize surgical outcomes.
- Further research is needed to assess the cost-effectiveness and broader feasibility of routine CBCT use in PCNL.
Following his presentation, Dr. Denstedt inquired about the average radiation exposure for patients. In response, Dr. Kingma shared that his team has been able to decrease their radiation from standard settings by a factor of 5, with a dose average between 1.5-2.5 millisieverts.
Presented by: Reimer Adam Kingma, Department of Urology, Urology Resident, UMCG Groningen, The Netherlands
Written by: Mariah Hernandez, Research Specialist, Department of Urology, University of California, Irvine, @mariahch00 on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.
References:- Kingma RA, Doppen C, Bus MTJ, Altobelli E, de Jong IJ, Roemeling S. The significance of clinically insignificant residual fragments after percutaneous nephrolithotomy: an analysis into the relevance of complete stone clearance. World J Urol. 2024 Feb 14;42(1):78. doi: 10.1007/s00345-024-04774-z. PMID: 38353780; PMCID: PMC10866741.).