(UroToday.com) The Sunday morning plenary session, presented by Dr. Seth Bechis from the University of California, San Diego, was an informative discussion of the findings from a multicenter prospective study to compare stent usage in patients who underwent ureteroscopy treatment of renal stones. Conducted from 2019 to 2024, the primary objective was to compare complications and outcomes of ureteral stent placement versus stent omission.
Other authors listed were Daniel Wollin, Marcelino Rivera, Johann Ingimarsson, Kymora Scotland, Noah Canvasser, Naeem Bhojani, and Ryan His. The institutions that also participated in this trial were the University of California Davis, Maine Medical Center, Vanderbilt University, the University of California, Los Angeles, Indiana University, and the Centre hospitalier de l'Université de Montréal, which are members of the Collaborative for Research in Endourology group.

After showing his disclosures (Boston Scientific, Karl Storz, Ambu, Dornier, BD Endourology, and Calyxo), Dr. Bechis began by outlining the rationale of the study. Despite the traditional use of ureteral stents in patients undergoing ureteroscopy, stent placement is associated with factors such as pain, urgency, frequency, hematuria, and impact on quality of life. While AUA guidelines recommend the consideration of stent omission in certain uncomplicated cases, in practice, a majority of patients commonly receive stents. High-quality studies examining stent usage are limited, and there have been no prospective trials completed that compare the use of ureteral stents versus stent omission. Therefore, he, along with his colleagues, sought to conduct this interesting randomized controlled trial to shed light on the potential benefits urologists can provide their patients by limiting the use of ureteral stents.
The primary outcome of the study was an evaluation of complications in a 30-day postoperative time window that included emergency department visits, readmissions, and unanticipated provider visits. Secondary outcomes were patient-reported metrics such as answers from the WISQOL and PROMIS 6a questionnaires, as well as data entailing the time it took to return to work, phone calls due to symptoms experienced, postoperative narcotic use, unintentional stent dislodgement, UTI diagnosis, and hydronephrosis at 4 to 8 weeks. Patients greater than 18 years old who were scheduled for a unilateral ureteroscopy with lithotripsy for renal stones no greater than 1.5 centimeters were included. Exclusion criteria consisted of: solitary kidney, eGFR less than 60, ureteral stone, abnormal renal anatomy (such as horseshoe kidney), indwelling nephrostomy tube, planned bilateral ureteroscopy, or intraoperative complication.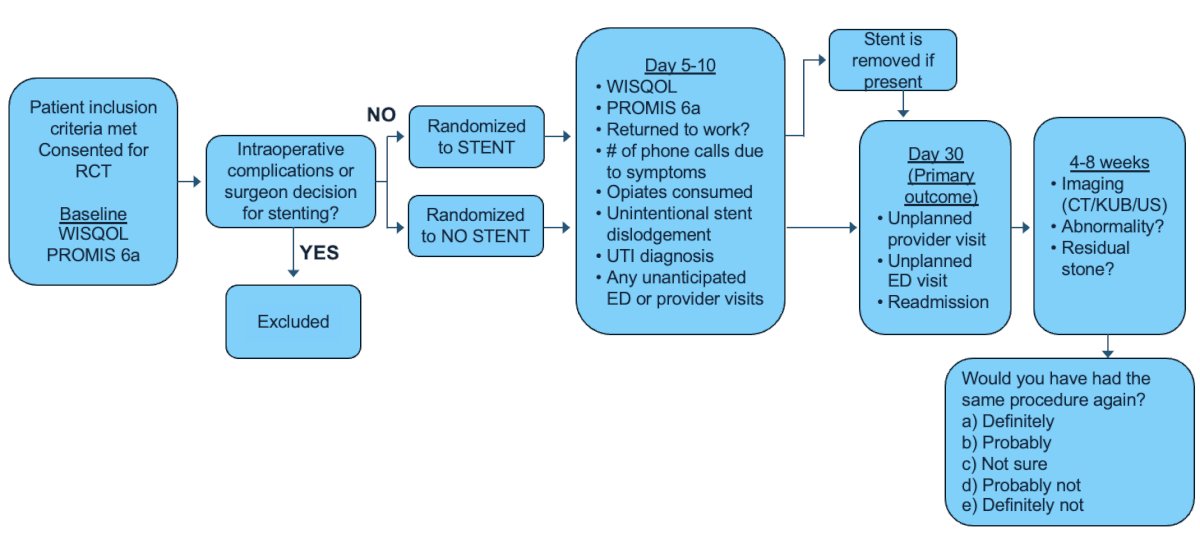
Importantly, Dr. Bechis emphasized that operative decision-making was untouched. Surgeons were left to choose their ureteroscopy technique, laser type and settings preferred, whether they employed a ureteral access sheath, and irrigation methods at their discretion. This was crucial as they clearly were keeping the well-being of consented patients at the forefront of their management, regardless of study participation. Subsequently, once the operation was completed, randomization occurred after stone treatment and ureteral inspection, ensuring the surgeon was blinded to allocation.
Of the 103 patients initially enrolled, 74 patients were included and randomized after 1 patient withdrew from the study, and 28 were excluded intraoperatively. 36 patients were randomized to the stent cohort and 38 to the no-stent cohort. Dr. Bechis noted that 60-80% of patients included had a ureteral access sheath deployed during their operation as a unique finding.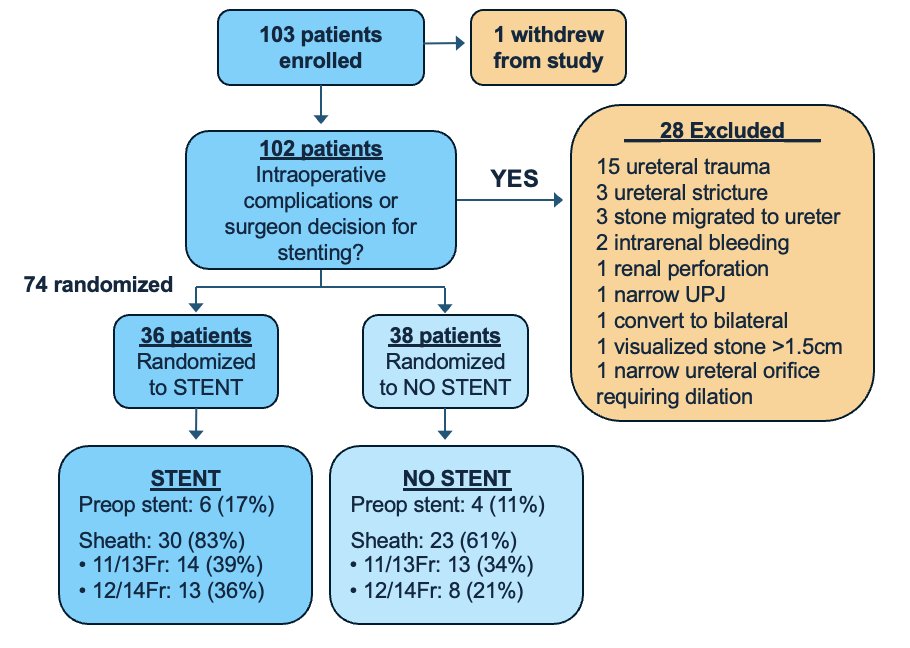
The presentation proceeded to give a detailed demographic and stone-specific breakdown of the cohorts. Dr. Bechis stated that there was no difference between the cohorts in terms of stone size, with an average stone size of 10 millimeters.
In terms of the intraoperative results, ureteral access sheaths were commonly used, with the 11/13 and 12/14 French sizes being the most frequent choices. A variety of stone treatment methods were used, including pure dusting, fragmenting with basketing, basket only, and a combination of dusting, fragmenting, and basketing. Post-treatment stone status results showed that very few patients still had residual stones. However, these were small in size, with fragments being 1 millimeter at max. Expectedly, the mean operative time was shorter in cases where a stent was ultimately not placed.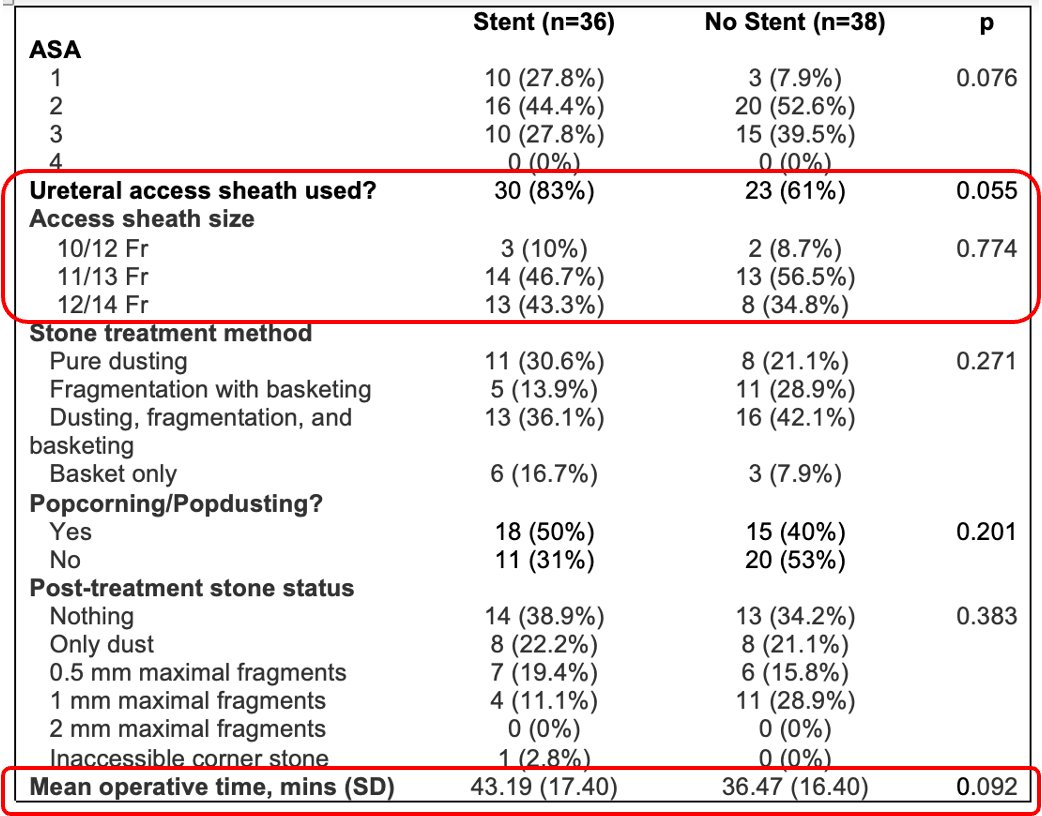
Interestingly, Dr. Bechis and his team noticed that superficial mucosal lesions in the ureter were found after ureteroscopy. Using the PULS grading index, this was seen in approximately 40% of patients.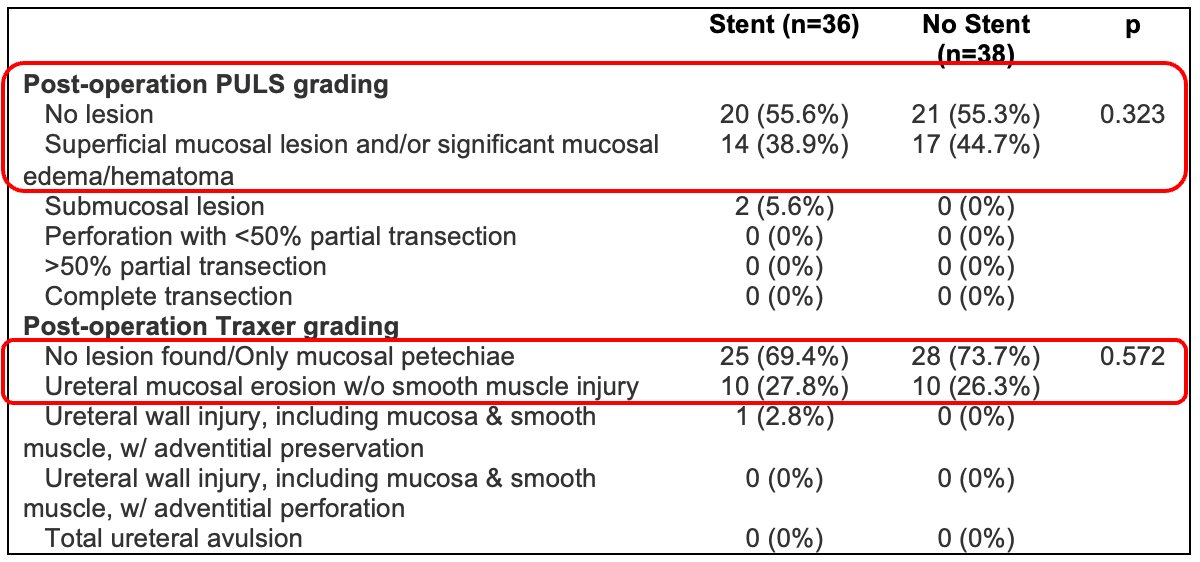
For the primary outcomes, there was no difference between the two groups in terms of emergency department visits, hospitalizations, or unanticipated provider visits.
Dr. Bechis proceeded to discuss the secondary outcomes. The PROMIS 6a Pain Interference tool is designed to assess how pain interferes with a person's daily activities and life which accounts for social activity participation, household chores, leisurely activities, and other factors. In their data, postoperative scores were significantly improved in cases where stents were omitted i.e. patients experienced less pain.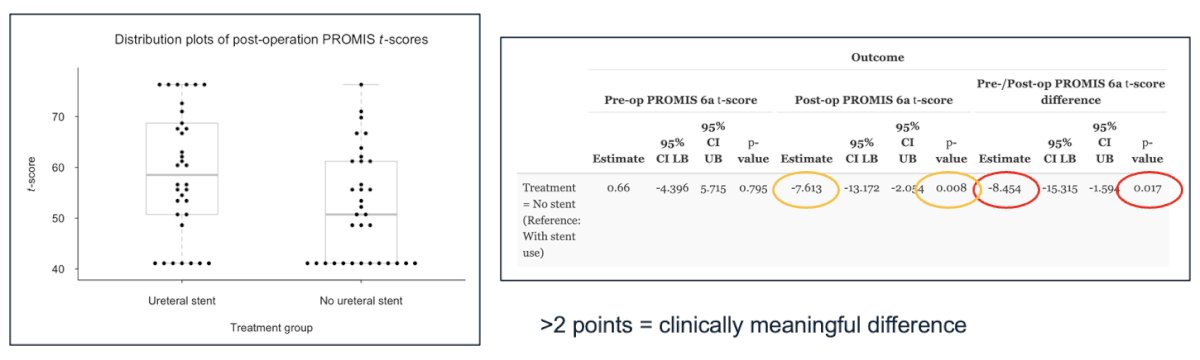
The WISQOL (Wisconsin Stone Quality of Life) questionnaire was additionally employed in outcome. Improved scores were also seen in these administered forms, that demonstrated a decreased impact on a patient’s quality of life if a stent was not used in their operation.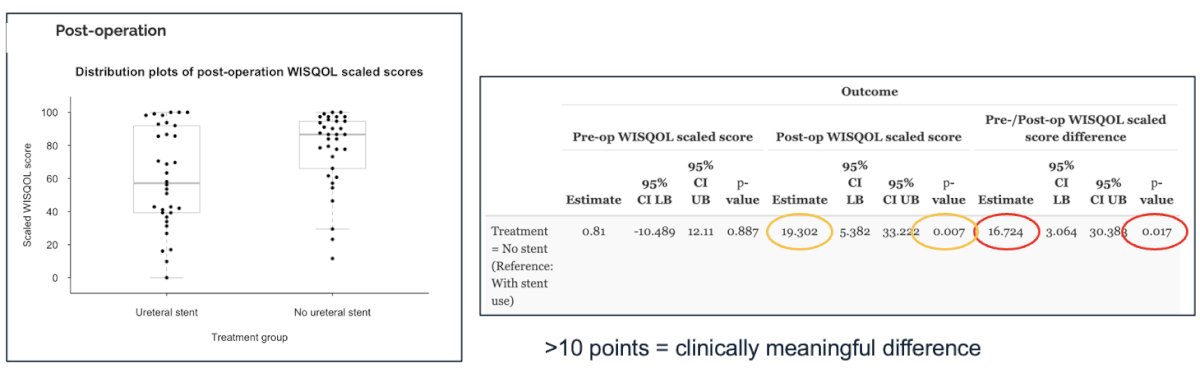
Also seen amongst the data for secondary outcomes was no difference in ability to return to work, postoperative UTI diagnosis, postoperative abnormalities in follow-up imaging, or opiate medication use.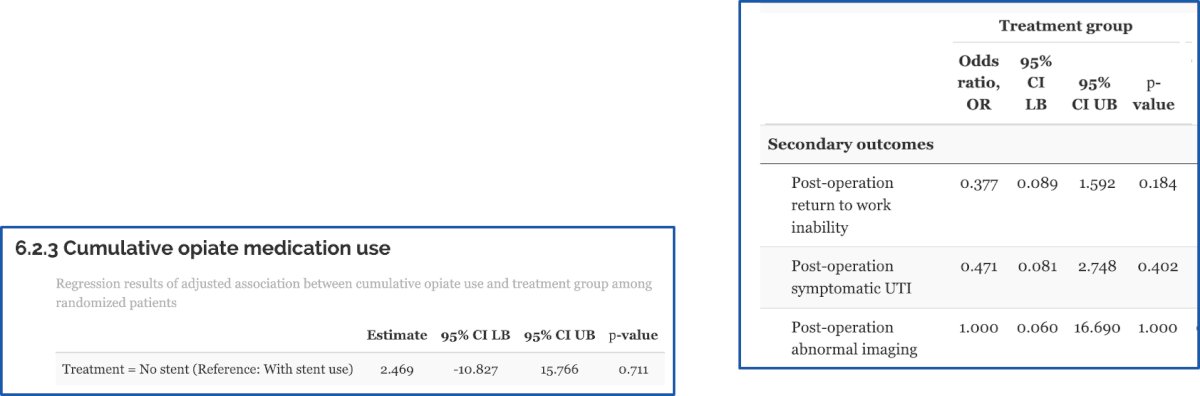
In terms of the stone clearance rates, the research team found that the data was similar. Between the cohorts, there was an approximate 40-58% stone free rate with CT, ultrasound, and KUB imaging used. There was also no difference seen in rates of hydronephrosis, urinoma, or hematoma complications.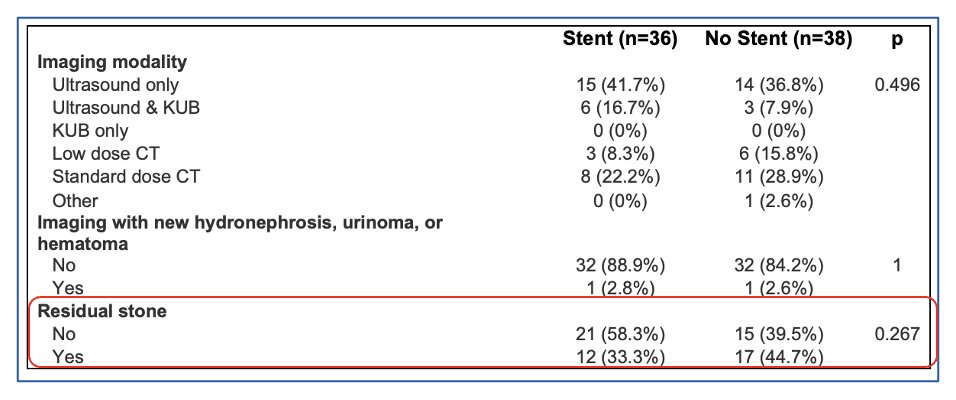
Most striking in this presentation was the patient preference findings. When asked if they would choose the same procedure again, patients overwhelmingly expressed a preference for avoiding a stent. Specifically, patients who underwent stent omission were far more likely to say they would "definitely" undergo the procedure again, compared to those who received a stent.
In his concluding remarks, Dr. Bechis summarized the clinical implications of this thorough randomized clinical trial. Firstly, Stent omission after uncomplicated ureteroscopy for renal stones less than 1.5 centimeters is safe without an increased risk of postoperative complications or unplanned healthcare utilization. Additionally, stent omission results in improved quality of life metrics, and patient satisfaction is markedly higher. He then stressed that several important criteria when considering stent omission: uncomplicated cases with stone burdens of 1-1.5 centimeters, use of ureteral access sheaths is acceptable, and no significant residual stone fragments (greater than 1 millimeter) at the end of the procedure. Lastly, superficial mucosal ureteral lesions should not preclude stent omission. Dr. Bechis was thoughtful in encouraging urologists to empathetically apply the findings from this study in clinical practice. Overall, this study demonstrates that stent omission is not only safe but also beneficial in improving patients’ experiences following ureteroscopy procedures for renal stones.
Presented by: Seth Bechis, MD, University of California, San Diego
Moderated by:
Jorge Gutierrez-Aceves, MD, Center Director for Endourology and Stone Disease at the Cleveland Clinic Department of Urology.
Roger Sur, MD, Director of the Comprehensive Kidney Stone Center at the University of California, San Diego.
Sam Chang, MD, Chief Surgical Officer at the Vanderbilt Ingram Cancer Center and Urologic Oncology Division Chief.
James Lingeman, MD, Professor Emeritus of Clinical Urology at Indiana University.
Written by: Yezan Hadidi, BS, Department of Urology, University of California Irvine. @yezanhadidi on X during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.