In a prospective randomized study of 20 patients undergoing Endoscopic Combined Intrarenal Surgery (ECIRS), the team compared two laser platforms: a 60W Super-Pulse Thulium Fiber Laser (TFL) and a 120W pulse-modulated Holmium:YAG laser. Using a Multi-Point Thermal Sensor (MTS) needle (Boston Scientific), they directly measured fluid and tissue temperatures at various depths from the calyx into the renal parenchyma.
Each patient underwent sequential laser activation in three commonly used modes: fragmentation (low power), dusting (moderate power), and pop-dusting (high power), with temperatures recorded throughout (Figure 1). Lasering was halted if parenchymal temperatures exceeded 43°C — a threshold associated with risk of renal damage.
The findings were striking. Low-power fragmentation remained below the danger threshold in all patients. However, during higher-powered dusting and pop-dusting modes, calyceal and parenchymal temperatures exceeded 43°C in as little as 15 seconds. During pop-dusting, calyceal temperatures exceeded 43°C in a majority of cases (10/10 TFL and 8/10 Ho:YAG), with the TFL group showing significantly higher maximum temperatures (Figures 2 and 3; T-max 52.9°C vs 45.1°C, p=0.027). Parenchymal temperatures also exceeded 43°C in several patients, raising concerns about the risk of thermal injury.
In her concluding remarks, Dr. Gupta emphasized that low-energy settings did not cause temperature elevations above 43°C, but during high-powered settings, both calyceal and parenchymal temperatures could rise dangerously in as little as 15 seconds. These findings suggest that tissue damage can occur during high-power laser lithotripsy, though the extent to which this injury affects renal function and whether it is recoverable remains to be determined.
During the Q&A session, Dr. Ryan Hsi, professor of Urology at Vanderbilt University, posed a question regarding the experimental setup. Dr. Gupta clarified that the study was deliberately designed as a "worst-case scenario" — using gravity irrigation without suction or access sheaths — to maximize the potential for heat buildup, ensuring that any risks would not be underestimated.

Figure 1. Flowchart describing ECIRS laser lithotripsy settings. Patients were randomized to receive Thulium fiber laser (TFL; n=10) or Holmium:YAG (Ho:YAG, n=10) laser lithotripsy.

Figure 2. Mean max temperatures at each renal landmark by laser and setting.
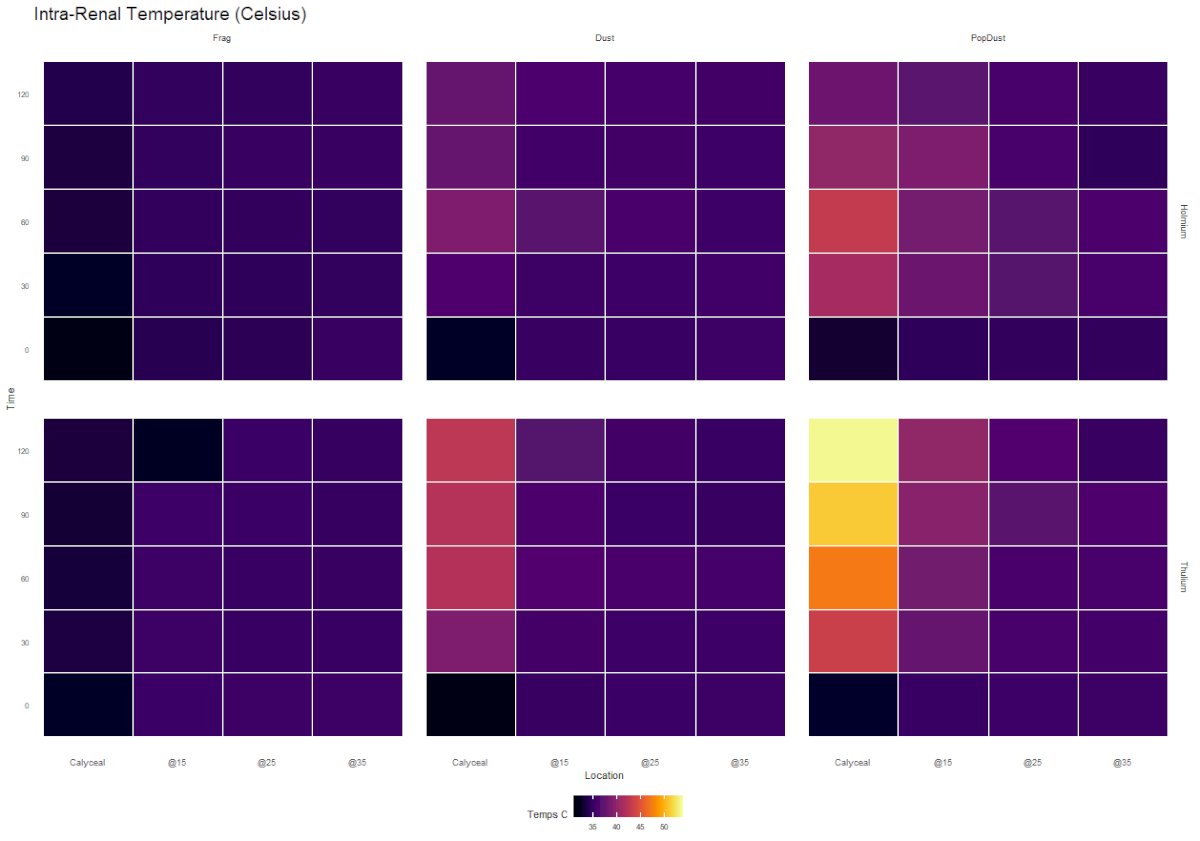
Figure 3. Heat map representation of calyceal and parenchymal temperatures for both pulse-modulated Ho:YAG and SuperPulse TFL for all settings.
Written by: Brandon Camp, MS3 UCI School of Medicine, during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025