(UroToday.com) Dr. Leilei Xia, Clinical Oncology Fellow at the University of Southern California Norris Comprehensive Cancer Center, presented institutional data examining the impact of the level of nodal metastasis (N⁺) and the incidence of skip metastases in patients with muscle-invasive bladder cancer (MIBC) who underwent radical cystectomy (RC) with super-extended lymph node dissection (ELND) in the era following the S1011 trial. While S1011 showed no survival benefit of ELND compared to standard lymph node dissection (SLND), this study aimed to assess whether certain patterns of nodal disease might still inform outcomes or justify extended dissection.
Using a prospectively maintained IRB-approved institutional cystectomy database, the investigators identified 738 patients with cT2–4aN0M0 urothelial carcinoma who underwent RC and super-extended LND between 2002 and 2023, with or without neoadjuvant chemotherapy (NAC). Lymph node levels were defined anatomically as follows: Level 1 (SLND) – external/internal iliac and obturator nodes; Level 2 (ELND) – common iliac, presacral, and pre-sciatic nodes; and Level 3 (ELND) – paraaortic and paracaval nodes. Patients were stratified by the highest level of nodal metastasis, and skip metastasis was defined as positive nodes in level 2 or 3 in the absence of level 1 involvement.
Out of the 738 patients, 159 (21.5%) were node positive. Among them, 100 (62.9%) had their highest or only nodal disease at level 1, 22 (13.8%) at level 2, and 37 (23.3%) at level 3. Skip metastasis was rare, occurring in only 7 patients (4.4%) — 3 (1.9%) at level 2 and 4 (2.5%) at level 3. The authors emphasized that this low rate of skip metastasis questions the diagnostic value of routinely extending the dissection.

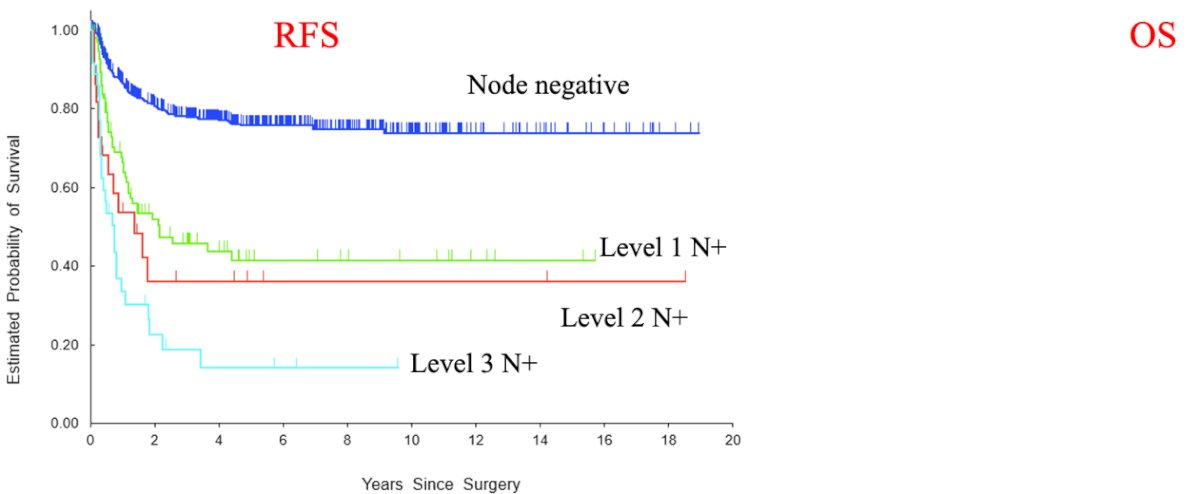
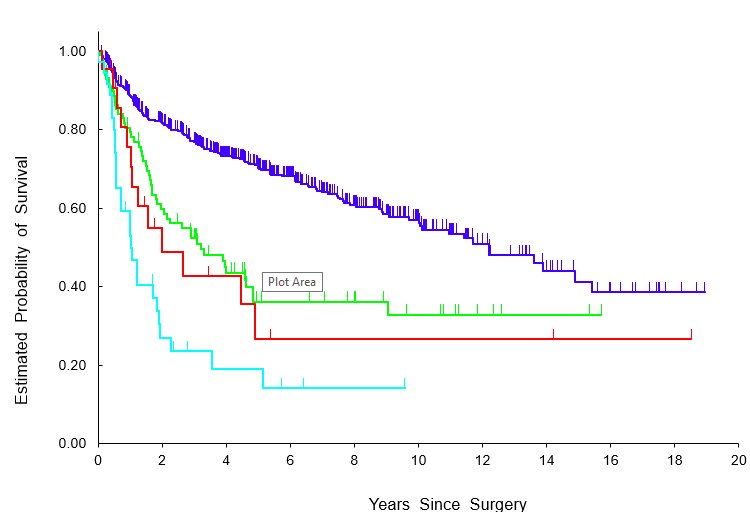
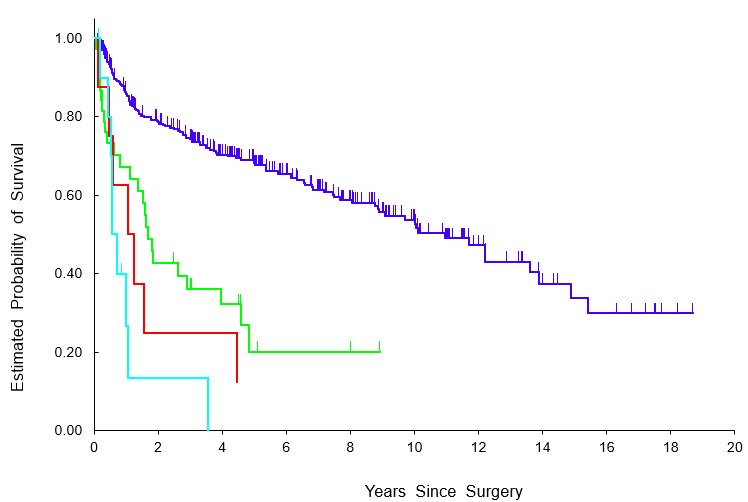
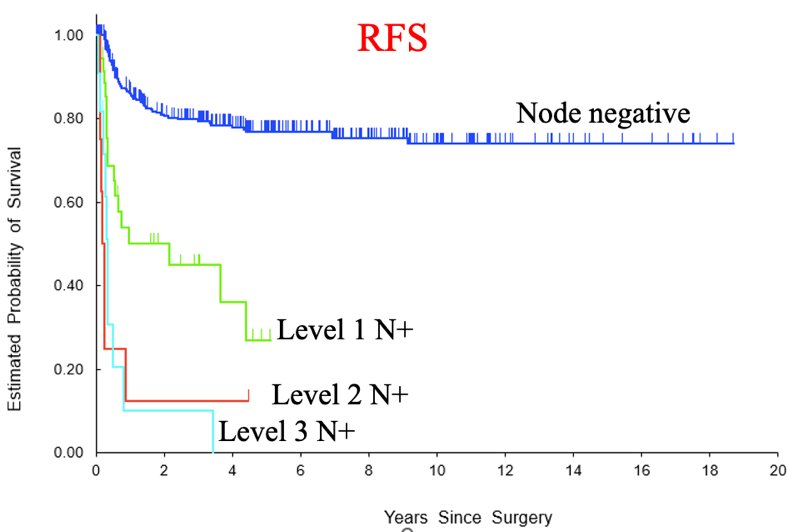
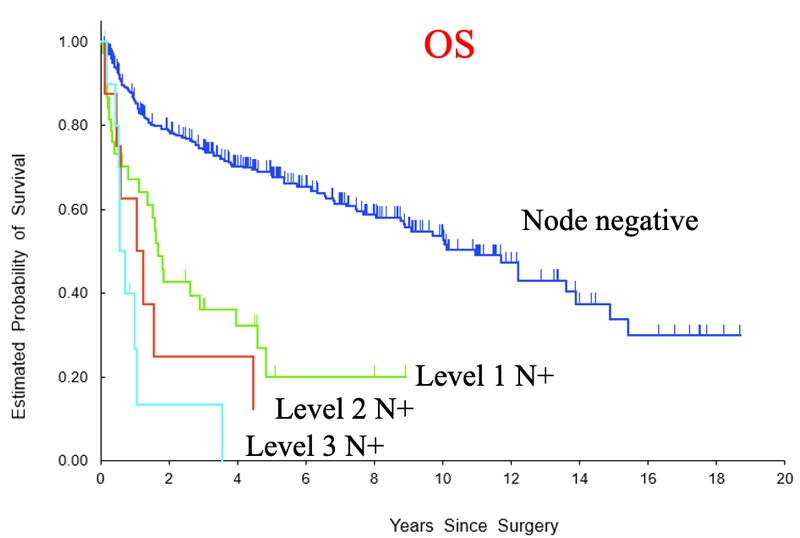
As shown in the Kaplan-Meier analyses, survival outcomes worsened progressively with increasing nodal level. Two-year recurrence-free survival (RFS) was 81% in node-negative patients, 52% in level 1 N⁺, 36% in level 2 N⁺, and 23% in level 3 N⁺. Corresponding 2-year overall survival (OS) rates were 82%, 60%, 49%, and 27%, respectively.
Further stratification based on receipt of perioperative chemotherapy highlighted its critical impact. For level 1 N⁺ patients who did not receive chemotherapy (n = 38), 2-year RFS and OS were 45% and 43%, respectively. In contrast, among those with level 2 or 3 N⁺ who did not receive chemotherapy (n = 16), 88% died within 2 years, and 63% died within 1 year.
An additional finding from multivariable analysis was that lymphovascular invasion significantly increased the likelihood of harboring higher-level nodal disease (levels 2–3), with an odds ratio of 9.4 (95% CI: 4.5–21.4). This suggests potential predictive utility for identifying patients at greater risk of advanced nodal spread.
In conclusion, Dr. Xia emphasized that the therapeutic benefit of ELND appears minimal in patients with higher-level nodal metastasis, especially in the absence of systemic chemotherapy. Furthermore, due to the low incidence of skip metastasis (<5%), the diagnostic benefit of ELND is also likely limited. In the post-S1011 era, the routine use of ELND may be unnecessary for most patients, and a template-based standard LND remains appropriate. However, prospective studies are warranted to clarify whether any MIBC subgroups may still derive benefit from ELND.
During the post-presentation discussion, panelists and attendees raised thoughtful questions regarding the implications of level 3 nodal involvement and the evolving role of extended lymph node dissection (ELND) in the adjuvant therapy era.
One panelist noted the unexpectedly higher proportion of level 3 (N3) nodal metastasis compared to level 2 (N2) and questioned whether this finding should prompt reconsideration of sampling level 3 nodes, not just for diagnostic purposes but for potential therapeutic benefit, particularly given the increased availability of effective adjuvant therapies.
Dr. Xia acknowledged that many patients with level 3 nodal disease likely had clinically evident nodal involvement at baseline and were referred for RC despite this. He emphasized that these patients require systemic therapy regardless of surgical findings and that in many cases, ELND may not provide significant additional information. He also pointed out that selection bias and historical practice patterns may account for the chemotherapy-naive subgroup, particularly given that neoadjuvant chemotherapy use at USC has increased significantly over the past decade.
Another discussant expanded on this point, suggesting that patients with undetected nodal disease who went straight to surgery were likely cisplatin-ineligible or had other comorbidities. The group acknowledged that prior to 10 years ago, NAC was used less frequently at USC, and historical bias may explain the large number of non-chemotherapy patients in the cohort.
Reflecting on surgical training and philosophy, panelists highlighted that many surgeons previously believed in the therapeutic value of extended dissections, especially when taught under leaders like Dr. Don Skinner. While some expressed skepticism about the survival benefit of removing positive level 3 nodes, others argued that macroscopic disease should be removed whenever feasible, even if adjuvant therapy now provides the main therapeutic effect. One surgeon stated, “If I have a positive node there, I want to remove it. We're surgeons—we aim to remove maximal disease and rely on adjuvant therapy for micrometastatic disease.”
However, there was consensus that current data do not demonstrate a clear therapeutic benefit for level 3 dissections. Instead, panelists agreed that systemic therapy has likely eclipsed any marginal benefit from extended surgical resection in these patients. As one discussant summarized, "There may be a very small therapeutic value, but systemic therapy is so powerful now, it probably overshadows any benefit from extended dissection.”
Presented by: Leilei Xia, MD, Clinical Oncology Fellow, Department of Urology, University of Southern California Norris Comprehensive Cancer Center, Los Angeles, CA
Written by: Seyedamirvala Saadat B.S., Research Specialist at Department of Urology, University of California Irvine, @Val_Saadat on X during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References: