(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, Nevada, was host to the PD37: Bladder Cancer: Invasive III Session. Dr. Katharina Oberneder presented PD37-05: Oncologic Outcomes in Patients Undergoing Radical Cystectomy for non–muscle-invasive bladder cancer (NMIBC) Following BCG Therapy Failure.
Dr. Oberneder highlighted that the U.S. FDA has approved several new agents for patients with high-risk non–muscle-invasive bladder cancer who experience recurrence after intravesical bacillus Calmette-Guérin (BCG) therapy. These include intravesical nadofaragene firadenovec, a gene therapy that delivers interferon alfa-2b via a non-replicating adenoviral vector; pembrolizumab, a systemic PD-1 checkpoint inhibitor; and nogapendekin alfa inbakicept (NAI), an intravesical IL-15 receptor agonist recently approved for use in this setting.
Despite this growing therapeutic landscape for BCG-unresponsive NMIBC, radical cystectomy remains the standard of care for patients with high-risk disease who experience recurrence after BCG and is endorsed and recommended by international clinical practice guidelines. Nevertheless, data on oncologic outcomes in patients with recurrent high-grade NMIBC following BCG therapy who undergo RC are still limited.
The investigators used data from a prospective multicenter registry to identify 141 patients across three centers who underwent early RC for non-muscle-invasive bladder cancer (NMIBC) recurrence following BCG failure. A descriptive analysis was performed on the treated population, followed by an evaluation of surgical complications within 30 and 90 days, categorized using the Clavien-Dindo classification. Additionally, cancer-specific survival (CSS) and overall survival (OS) were analyzed using the Kaplan-Meier method, with point estimates reported for survival rates.
A total of 141 patients were included in this analysis. Of these, 118 (84%) were male, with a median age of 73 years (IQR 66–77). Clinical staging prior to radical cystectomy included 67% with cT1 disease, 21% with cCIS, and 11% with cTa. All patients had N0 and M0 disease.
Final pathology revealed no residual tumor (pT0) in 9 patients (6.4%), pTa in 14 (9.9%), pTis in 31 (22%), and pT1 in 31 (22%). Muscle-invasive disease (≥pT2) was identified in 49 patients (34.8%), while lymph node metastases were found in 23 patients (16.3%), underscoring the significant rate of pathological upstaging in this high-risk clinical NMIBC population. Additionally, 13 patients (8%) had positive surgical margins, lymphovascular invasion was observed in 33 (23%), and 77 patients (50%) had concomitant carcinoma in situ (CIS).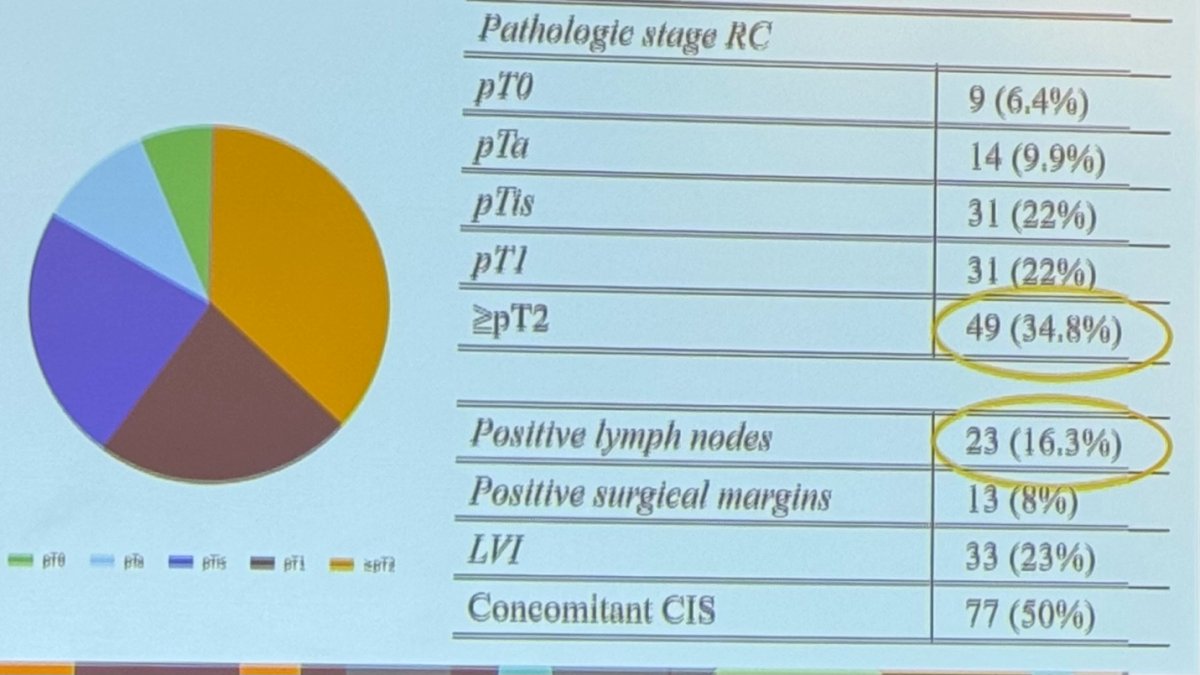
Progression to metastatic disease occurred in 3 patients (2.1%) following radical cystectomy. CSS rates at 12, 24, and 60 months were 95.9%, 90.5%, and 90.5%, respectively.
OS rates at 12, 24, and 60 months were 94.5%, 86.7%, and 74.4%, respectively. The OS Kaplan-Meier curve is shown below.

Regarding 30- and 90-day complications, within 30 days, 51 patients (36%) experienced minor complications (Clavien-Dindo <2), while 14 patients (9.9%) experienced major complications (Clavien-Dindo ≥3). The 30-day mortality rate was 0.7%. At 90 days, 10 patients (7.1%) developed minor complications, and 7 (5%) had major complications, with no additional mortalities reported. In this retrospective cohort, 15 patients (11%) received adjuvant treatment with either cisplatin-based chemotherapy or nivolumab. The relatively low rate of adjuvant therapy may be a limitation of the study, especially given the observed high incidence of lymph node metastases.
Dr. Oberneder concluded the presentation with the following key points:
- Clinical understaging in patients with high-risk, BCG-refractory NMIBC remains a challenge
- Overall, the investigators reported favorable oncologic outcomes for NMIBC patients receiving RC after BCG exposure
- RC remains a viable treatment option for patients experiencing recurrence following BCG therapy
Presented by: Katharina Oberneder, MD, Urology Resident, Sigmund Freud University of Vienna, Vienna, Austria.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.