(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, Nevada, was host to the PD37: Bladder Cancer: Invasive III Session. Dr Reuben Ben-David presented PD37-02: Precystectomy ctDNA Burden is Predictive of Poor Oncological Outcomes
Dr. Ben-David began his presentation by highlighting that tumor-informed circulating tumor DNA (ctDNA) has emerged as a novel prognostic biomarker in bladder cancer. His team sought to evaluate whether pre-cystectomy ctDNA burden could predict disease recurrence and time to progression following radical cystectomy.
The workflow involved resection of the bladder tumor during TURBT, followed by whole genome sequencing (WGS) of the specimen. Sixteen tumor-specific mutations were selected to create a personalized "tumor-informed signature." Blood samples collected from patients were then analyzed against this signature to detect the presence of ctDNA in the serum as illustrated below.
ctDNA assays (Signatera™, Natera Inc.) were collected prospectively and longitudinally from consecutive patients who underwent robotic-assisted radical cystectomy with intracorporeal urinary diversion between 2021 and 2023. ctDNA status was determined from pre-cystectomy specimens, and recurrence-free survival (RFS) was assessed through imaging studies, with biopsy confirmation in equivocal cases.
Dr. Ben-David highlighted that precystectomy ctDNA had previously been shown to be a strong predictor of pathological and oncological outcomes, though it was traditionally categorized qualitatively as either undetectable or detectable. In this study, the investigators further refined the classification by subcategorizing detectable ctDNA into low- or high-burden groups, based on mean tumor molecules per milliliter (MTM/mL), with thresholds set at:
- <2.5: low burden
- ≥2.5: high burden.
The cutoff of 2.5 MTM/mL provided a balance between sensitivity (51.2%) and specificity (81.3%). The area under the curve (AUC) was 67%, and the Youden Index was 32.5%. The group distribution according to different cutoff values is shown below, supporting the selection of 2.5 MTM/mL as the optimal threshold for this study.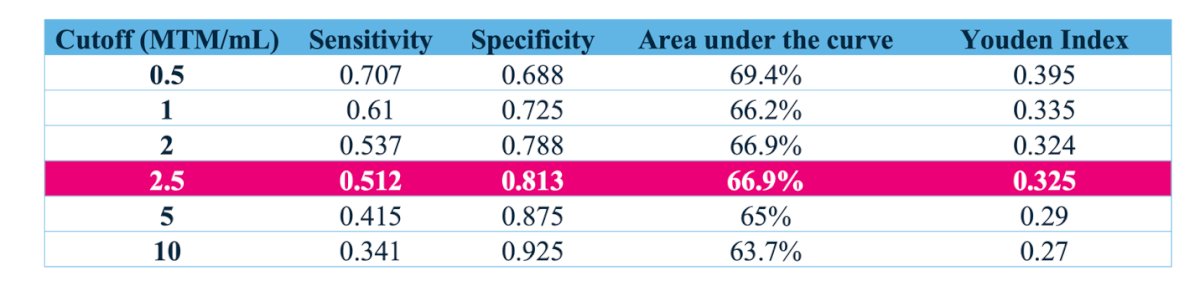
The cohort consisted of 162 patients, of whom 120 had sufficient follow-up (≥3 months) and a precystectomy ctDNA status to assess recurrence.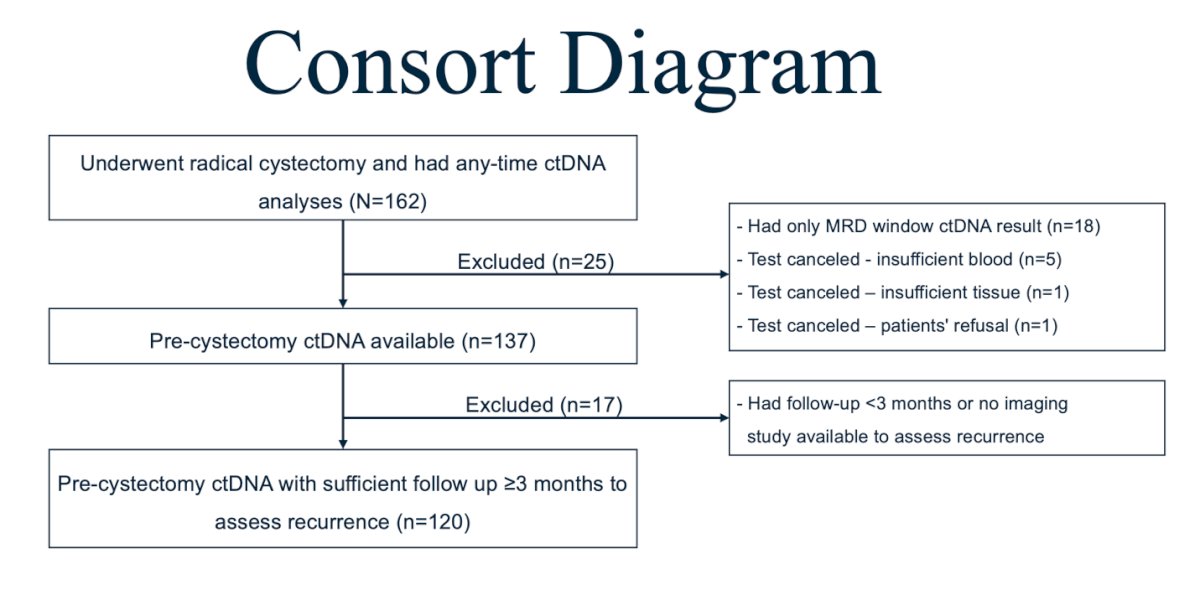
Overall, 823 ctDNA analyses were collected. The median age of the cohort was 71 years (IQR 64–77), with a median follow-up period of 11 months (IQR 6–18). Baseline characteristics are summarized in the table below. After applying the 2.5 MTM/mL cutoff, the group distribution was: undetectable precystectomy ctDNA (n=53), detectable low-burden ctDNA (n=31), and detectable high-burden ctDNA (n=36).

Dr. Ben-David noted that significant differences (p<0.001) were observed between the undetectable precystectomy ctDNA group and the detectable groups in terms of pathological T stage (pT), nodal status (pN), distant recurrence, and time to recurrence, as illustrated below.
A total of 40 patients (33.3%) experienced recurrence. Detectable precystectomy ctDNA had a significantly worse RFS; median RFS was not reached in the undetectable group vs. 11.5 months in the low ctDNA burden group, and 5.2 months in the high ctDNA burden group, as shown in the RFS curves below.
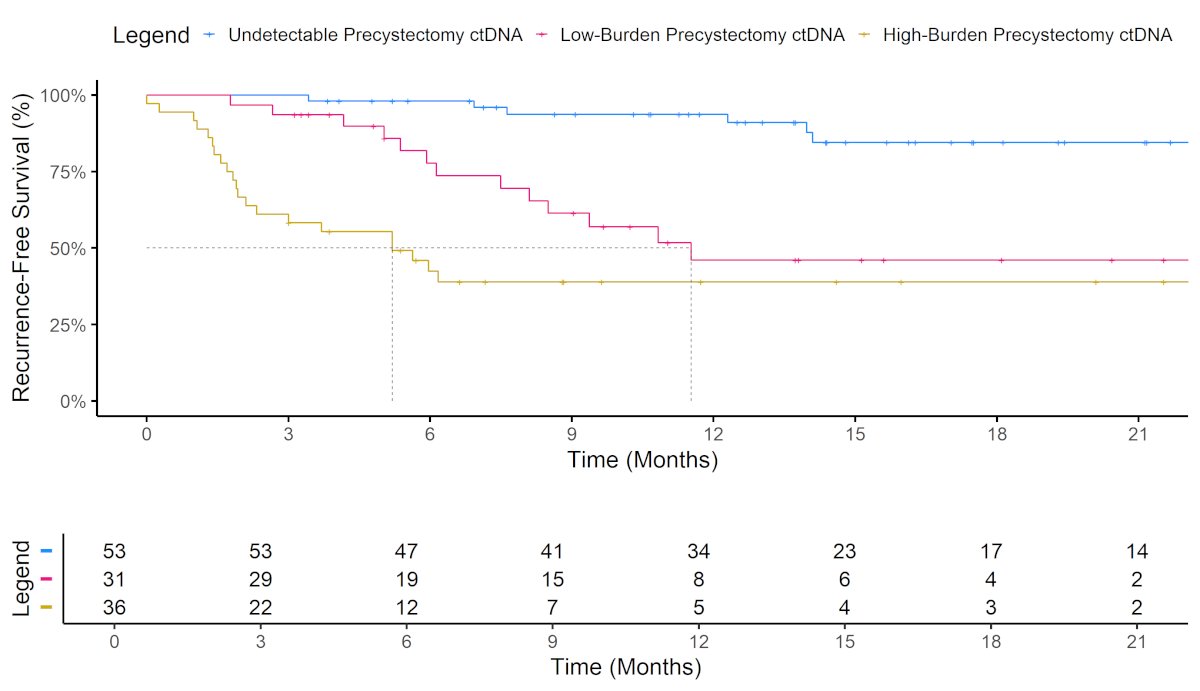
The 3-, 6-, and 12-month recurrence-free survival (RFS) rates in the undetectable ctDNA group were 100%, 98%, and 94%, respectively, and were significantly higher compared to both the low-burden and high-burden ctDNA groups.
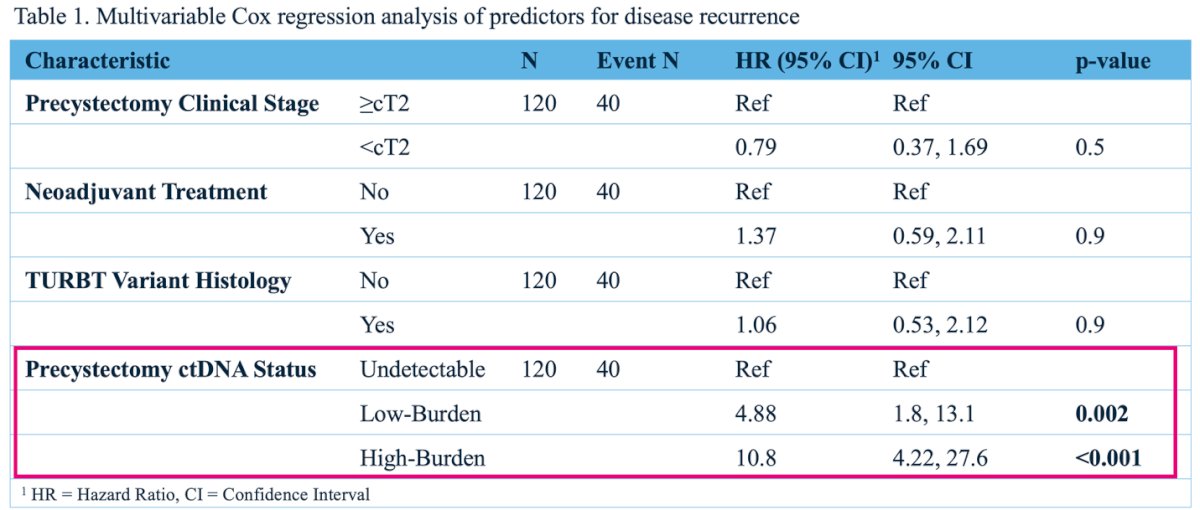
On multivariate analysis, adjusting for precystectomy clinical stage, variant histology on TURBT, and neoadjuvant treatment, only detectable precystectomy ctDNA status remained predictive of disease recurrence. Patients with low ctDNA burden had a hazard ratio (HR) of 4.88 (95% CI, 1.8–13.1; p=0.002), and those with high ctDNA burden had an HR of 10.8 (95% CI, 4.2–27.6; p<0.001).
Dr. Ben-David concluded his presentation with the following key takeaways:
- ctDNA burden offers a novel method to further sub-categorize patients with detectable precystectomy ctDNA.
- Precystectomy ctDNA burden, measured in MTM/mL, successfully defined distinct groups with different oncological outcomes.
- Given the high risk of rapid progression in patients with high-burden ctDNA (3-month RFS of 58.3%), treatment intensification should be considered.
- Patients with undetectable precystectomy ctDNA may be candidates for treatment de-escalation.
Presented by: Reuben Ben-David, MD, Society of Urologic Oncology (SUO) Fellow at Icahn School of Medicine, Mount Sinai Hospital, New York, NY
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.