(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, Nevada, was host to the PD37: Bladder Cancer: Invasive III Session. Dr. Pratik Kanabur presented PD37-11: Cost-effectiveness of Nivolumab or Pembrolizumab versus surveillance for the adjuvant treatment of patients with high-risk muscle-invasive bladder cancer.
Dr. Kanabur opened the presentation by addressing recurrence in muscle-invasive bladder cancer (MIBC), a persistent challenge despite aggressive treatment. Recurrence rates following neoadjuvant chemotherapy (NAC) and radical cystectomy (RC) range from 20% to 60%. Patients are considered high-risk if they have pT2–pT4 and/or node-positive disease after NAC, or pT3–pT4 and/or node-positive disease without NAC. In line with this, the American Urological Association guidelines currently recommend adjuvant immunotherapy for patients with high-risk MIBC following RC.
Notably, the costs associated with MIBC have skyrocketed in recent years. Urothelial cancer is now among the most expensive cancers to treat, with per-patient costs ranging from $100,000 to $200,000, driven largely by non-cystectomy-related hospital expenses.
Dr Kanabur highlighted that in an observational cohort study, 91.2% of patients who underwent RC still opted for adjuvant therapy, with overall survival and the risk of serious side effects emerging as key factors influencing treatment decisions, as shown below.1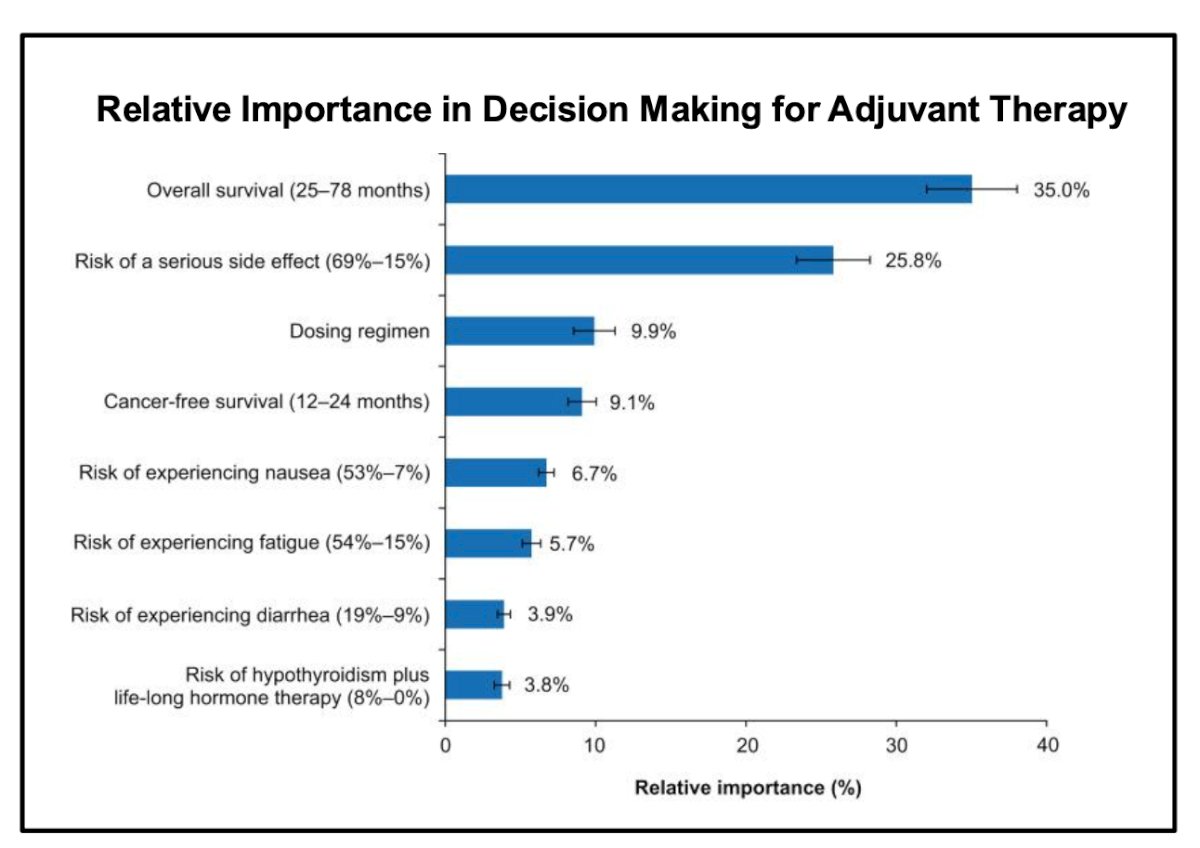
Summary of Supporting Evidence
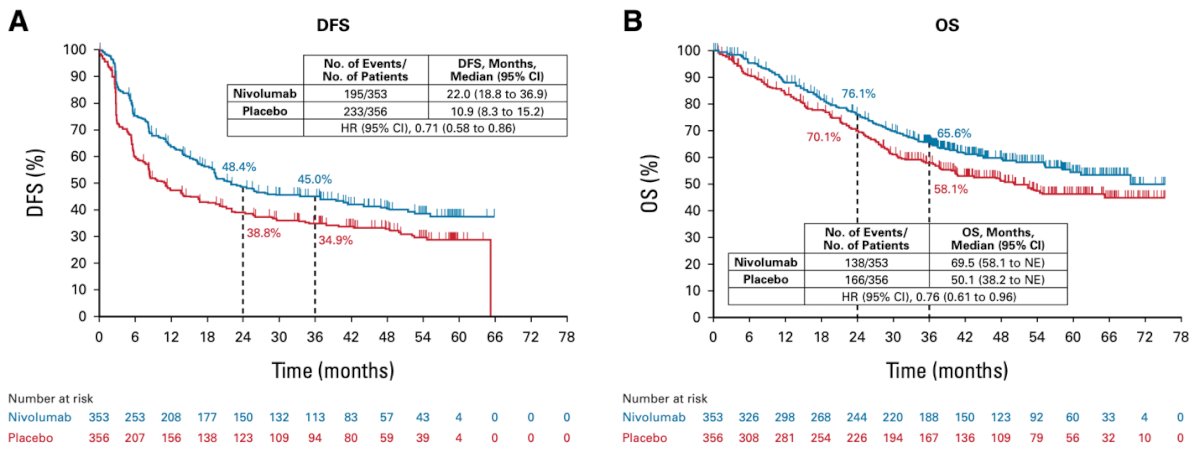
CheckMate-274 was a Phase III, randomized trial evaluating nivolumab (240 mg every two weeks) versus placebo in patients with high-risk MIBC. Notably, median disease-free survival was significantly longer with nivolumab at 22.0 months compared to 10.9 months with placebo. The trial demonstrated that adjuvant therapy improves both disease-free and overall survival in this population.2
The AMBASSADOR study was a Phase III randomized trial evaluating pembrolizumab 200 mg every three weeks versus observation in patients with high-risk MIBC. The median DFS was 29.6 months in the pembrolizumab arm compared to 14.2 months in the observation group (hazard ratio [HR], 0.73; 95% CI, 0.59–0.90). These findings demonstrate that adjuvant pembrolizumab significantly improves DFS in patients with high-risk MIBC.3
![The AMBASSADOR study was a Phase III randomized trial evaluating pembrolizumab 200 mg every three weeks versus observation in patients with high-risk MIBC. The median DFS was 29.6 months in the pembrolizumab arm compared to 14.2 months in the observation group (hazard ratio [HR], 0.73; 95% CI, 0.59–0.90). These findings demonstrate that adjuvant pembrolizumab significantly improves DFS in patients with high-risk MIBC](/images/com-doc-importer/207-aua-2025/aua-2025-pd37-11-cost-effectiveness-of-nivolumab-or-pembrolizumab-versus-surveillance-for-the-adjuvant-treatment-of-patients-with-high-risk-muscle-invasive-bladder-cancer/image-2.jpg)
The aim of this study was to evaluate the cost-effectiveness of adjuvant nivolumab versus pembrolizumab, compared to surveillance, for the treatment of patients with high-risk MIBC from a U.S. healthcare payer perspective.
The investigators developed a three-transition Markov model to compare the cost-effectiveness of adjuvant nivolumab and pembrolizumab versus surveillance, followed by treatment for metastatic disease. Model inputs included drug costs based on average sale prices from the Centers for Medicare and Medicaid Services, adverse event costs derived from published literature, and administration costs from the Medicare physician fee schedule. Health utility values were also sourced from literature and converted to quality-adjusted life years (QALYs) on a 0–1 scale. Transition probabilities were informed by disease-free to metastatic progression from the CheckMate 274 and AMBASSADOR trials,2,3 disease-free to death using U.S. Life Tables, and metastatic to death based on published data. DFS was extrapolated from the literature and expressed as hazard ratios. Below is an example of an extrapolation curve for DFS.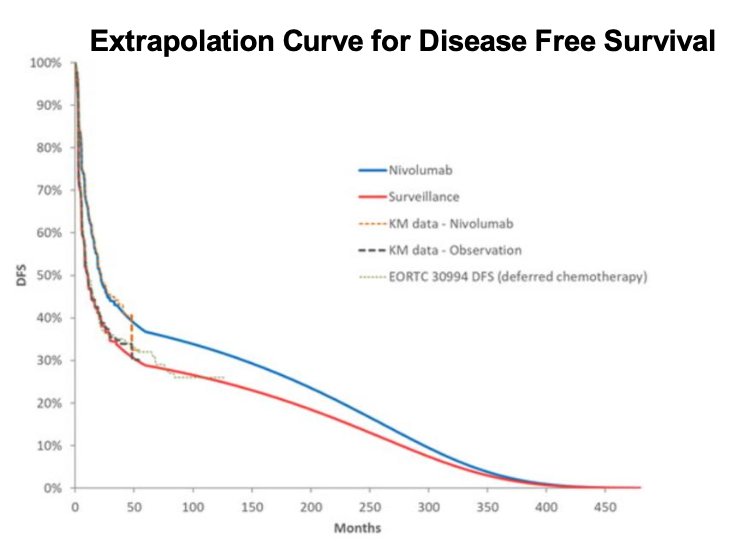
Probabilistic sensitivity analyses were conducted using 1,000 Monte Carlo simulations, in which model parameters were simultaneously varied according to predefined statistical distributions. Cost variables, such as the price of nivolumab ($10,000–$18,000 USD), followed a gamma distribution, while utility values, such as the utility assigned to metastatic disease (0.71), followed a beta distribution. The willingness-to-pay threshold was set at $100,000 per QALY.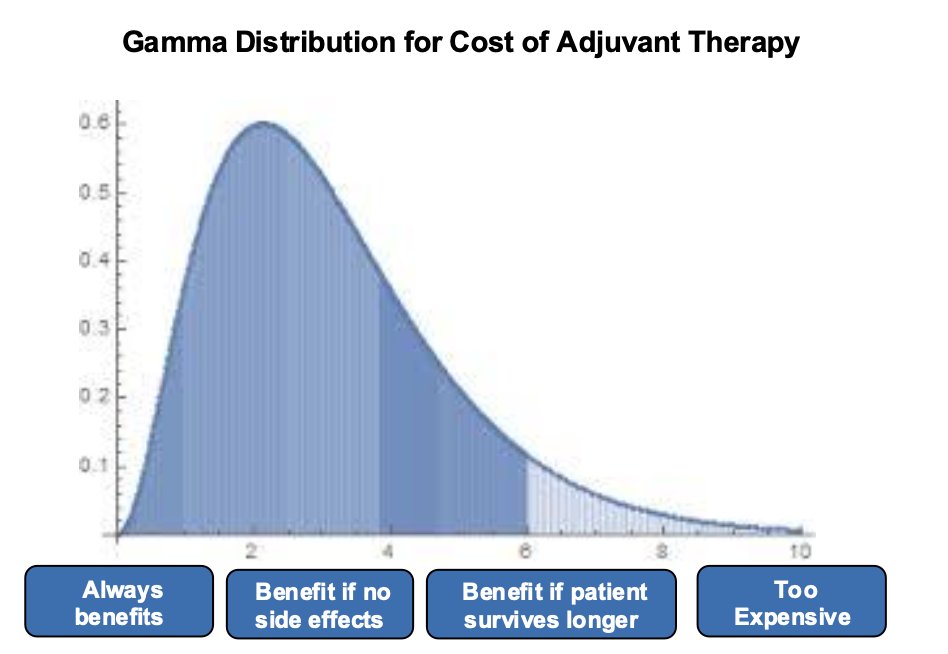
In the base-case analysis, the investigators found that total costs were higher for pembrolizumab ($190,161 USD) and nivolumab ($218,091) compared to surveillance ($93,846). However, both adjuvant therapies improved DFS and QALYs. Notably, pembrolizumab demonstrated the lowest incremental cost-effectiveness ratio (ICER) at $50,476 per QALY and was the dominant strategy among the three, as shown in the table below.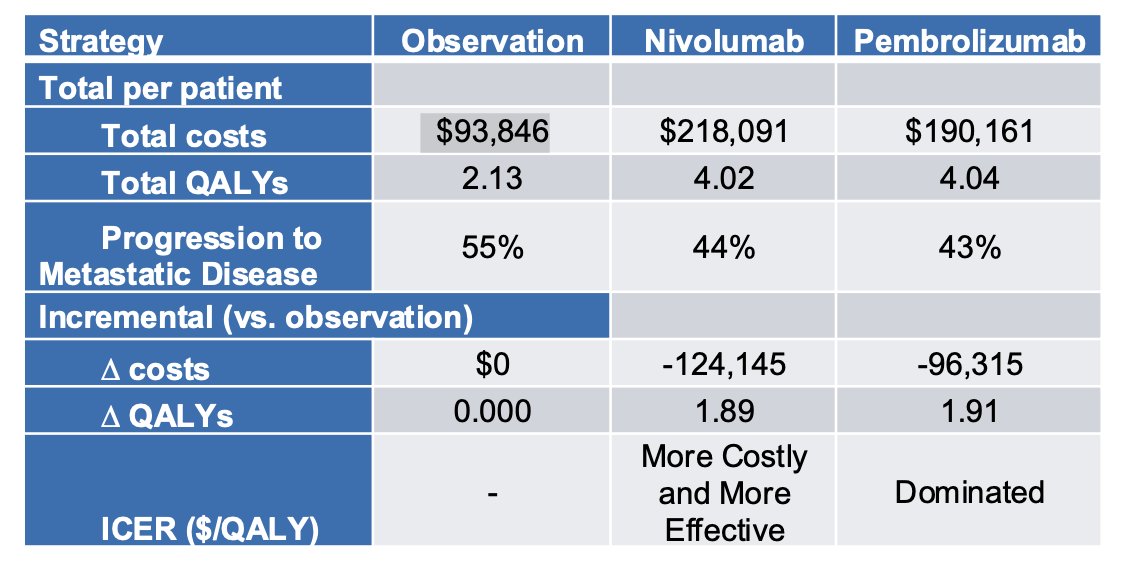
The probabilistic sensitivity analysis demonstrated that pembrolizumab had the highest probability of being the most cost-effective strategy across a broad range of commonly accepted willingness-to-pay (WTP) thresholds. At WTP values above $100,000, pembrolizumab consistently emerged as the most cost-effective option. However, at lower WTP thresholds, observation remained the more cost-effective strategy.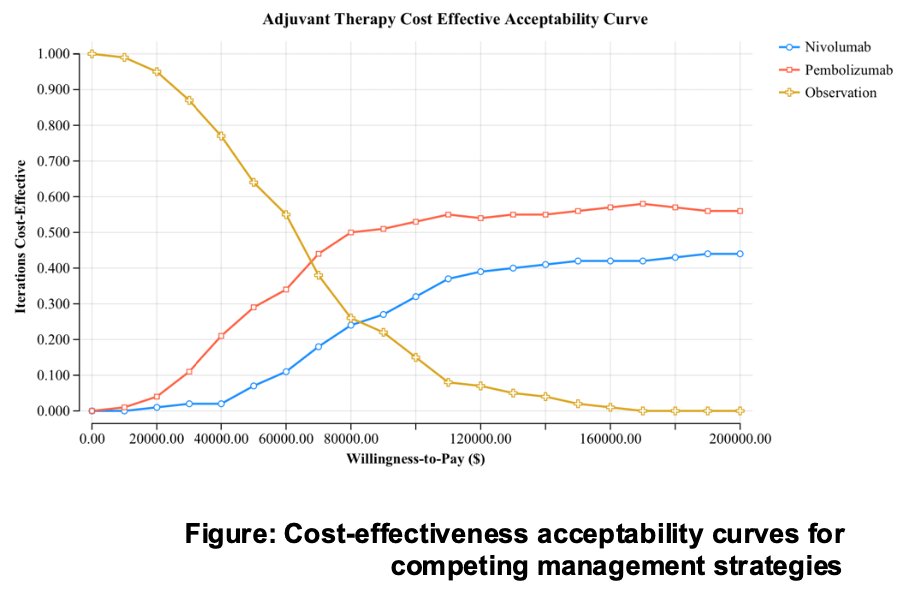
Dr Kanabur concluded his presentation with the following key takeaways:
- Both pembrolizumab and nivolumab are effective adjuvant therapies that improve disease-free survival in high-risk muscle-invasive bladder cancer.
- Pembrolizumab demonstrated greater cost-effectiveness compared to nivolumab and observation.
- Probabilistic sensitivity analysis favored pembrolizumab across a range of willingness-to-pay thresholds.
- These findings support value-based decision-making in selecting adjuvant therapies.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
References:- King-Concialdi K, Beusterien K, Senglaub SS, Will O, Jaffe DH, Patel MY, Harrison MR. Patient Preferences for Adjuvant Treatment in Muscle-Invasive Urothelial Carcinoma: A Multi-Country Discrete Choice Experiment. Patient Prefer Adherence. 2023 Sep 8;17:2237-2248. doi: 10.2147/PPA.S411751. PMID: 37706208; PMCID: PMC10497056.
- Galsky MD, Witjes JA, Gschwend JE, Milowsky MI, Schenker M, Valderrama BP, Tomita Y, Bamias A, Lebret T, Shariat SF, Park SH, Agerbaek M, Jha G, Stenner F, Ye D, Giudici F, Dutta S, Askelson M, Nasroulah F, Zhang J, Brophy L, Bajorin DF. Adjuvant Nivolumab in High-Risk Muscle-Invasive Urothelial Carcinoma: Expanded Efficacy From CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21. doi: 10.1200/JCO.24.00340. Epub 2024 Oct 11. PMID: 39393026; PMCID: PMC11687940.
- Apolo AB, Ballman KV, Sonpavde G, Berg S, Kim WY, Parikh R, Teo MY, Sweis RF, Geynisman DM, Grivas P, Chatta G, Reichert ZR, Kim JW, Bilen MA, McGregor B, Singh P, Tripathi A, Cole S, Simon N, Niglio S, Ley L, Cordes L, Srinivas S, Huang J, Odegaard M, Watt C, Petrylak D, Hoffman-Censits J, Wen Y, Hahn O, Mitchell C, Tan A, Streicher H, Sharon E, Moon H, Woods M, Halabi S, Perez Burbano G, Morris MJ, Rosenberg JE. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55. doi: 10.1056/NEJMoa2401726. Epub 2024 Sep 15. PMID: 39282902; PMCID: PMC11698643.