(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, Nevada, was host to the PD37: Bladder Cancer: Invasive III Session. Dr. Joshua Meeks presented the first report of disease-free survival analyses from the NIAGARA trial of perioperative durvalumab plus neoadjuvant chemotherapy in muscle-invasive bladder cancer.
Dr. Meeks began his presentation by highlighting that NIAGARA is the first global, randomized Phase 3 trial to evaluate perioperative immunotherapy (IO) with durvalumab in combination with neoadjuvant chemotherapy (NAC) in cisplatin-eligible muscle-invasive bladder cancer (MIBC).
The trial enrolled adult patients with cisplatin-eligible MIBC (cT2–T4aN0/1M0), including those with divergent differentiation or histologic subtypes. All participants were confirmed as suitable candidates for radical cystectomy (RC). In the experimental arm, patients received durvalumab 1500 mg IV every 3 weeks (Q3W) with gemcitabine plus cisplatin (GC) for 4 cycles, followed by RC and adjuvant durvalumab 1500 mg IV every 4 weeks (Q4W) for up to 8 cycles.1 In the control arm, patients received GC followed by RC, with no adjuvant therapy. Based on the trial results, perioperative durvalumab in combination with NAC is now approved by the U.S. FDA for use in MIBC and has been designated a Category 1 recommendation by the National Comprehensive Cancer Network® (NCCN®).2
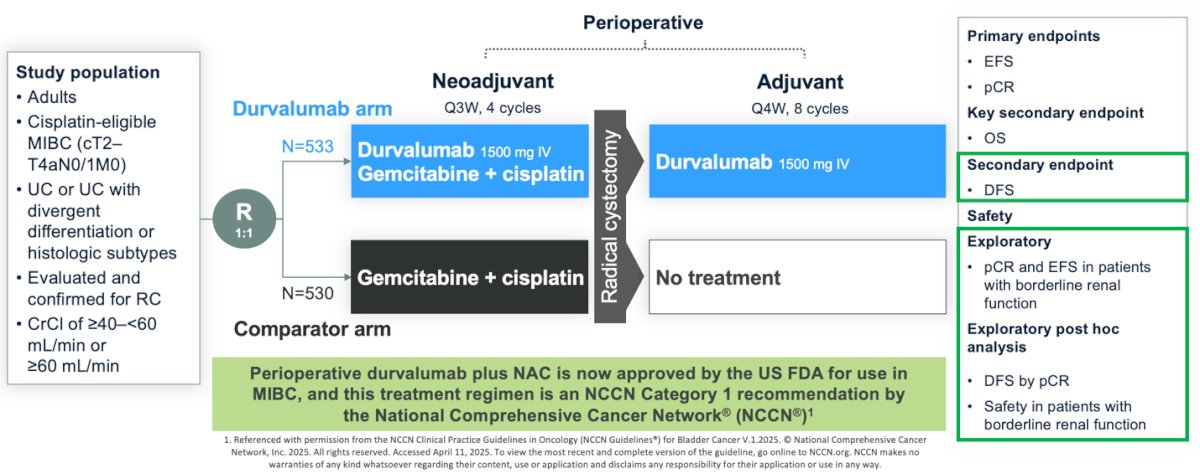
Perioperative durvalumab in combination with NAC demonstrated a statistically significant and clinically meaningful improvement in event-free survival (EFS) (HR, 0.68; 95% CI, 0.56–0.82; P < 0.0001) and overall survival (OS) (HR, 0.75; 95% CI, 0.59–0.93; P = 0.0106) compared to the standard-of-care arm.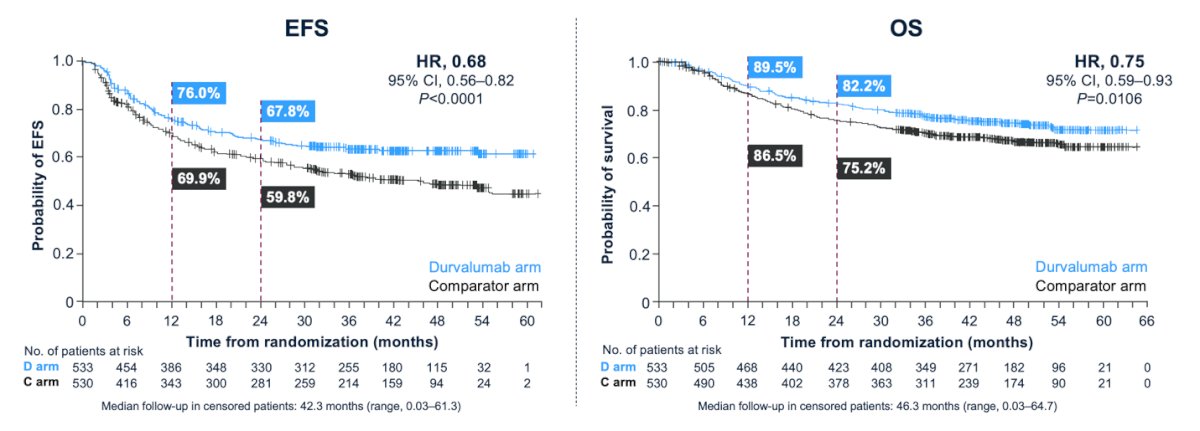
Moreover, the time to radical cystectomy and the rate of surgical complications were similar between treatment arms, further supporting the safety of the perioperative NAC plus immunotherapy combination in this setting.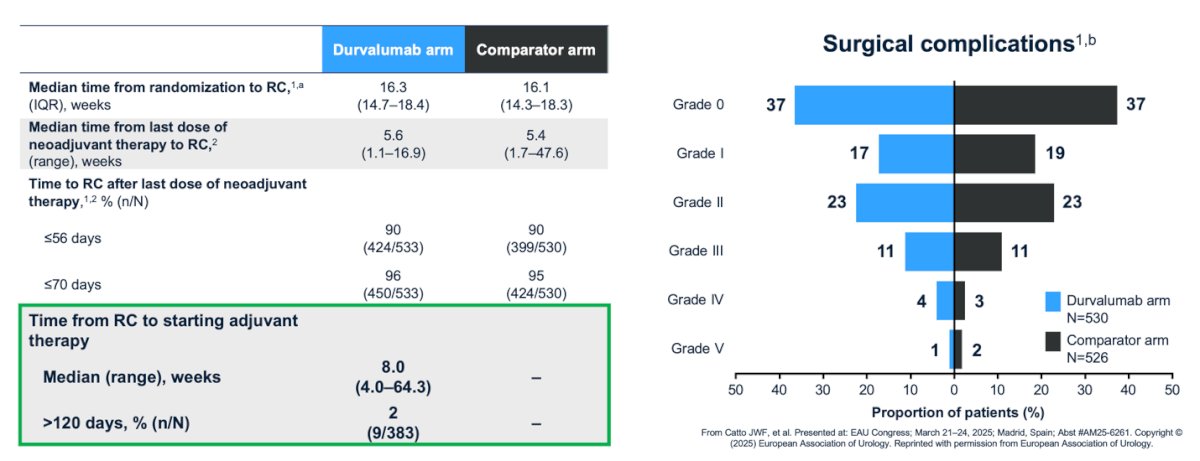
Dr. Meeks highlighted that event-free survival (EFS) captures events occurring at any point during or after perioperative treatment in the intent-to-treat (ITT) population, whereas disease-free survival (DFS) is assessed in patients who underwent radical cystectomy (RC), as illustrated in the graphic below. Notably, 63 patients in the durvalumab group did not undergo RC due to patient decision (n = 32), disease progression (n = 9), adverse events (n = 6), death (n = 5), investigator decision (n = 5), study discontinuation (n = 3), unfitness for surgery (n = 2), and one abandoned procedure. In the comparator group, 84 patients did not undergo RC due to patient decision (n = 36), study discontinuation (n = 12), disease progression (n = 9), death (n = 8), adverse events (n = 7), investigator decision (n = 6), and unfitness for surgery (n = 6).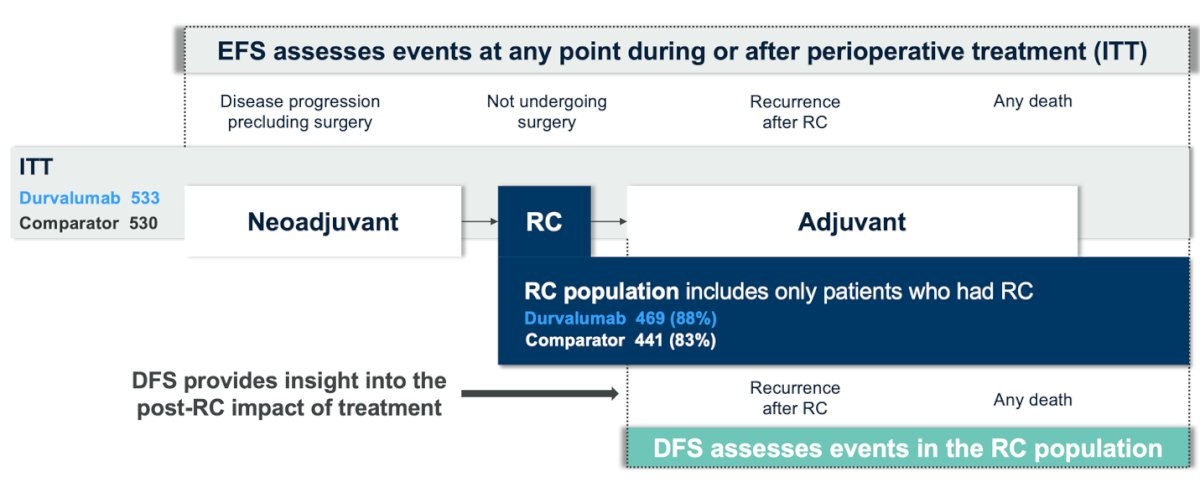
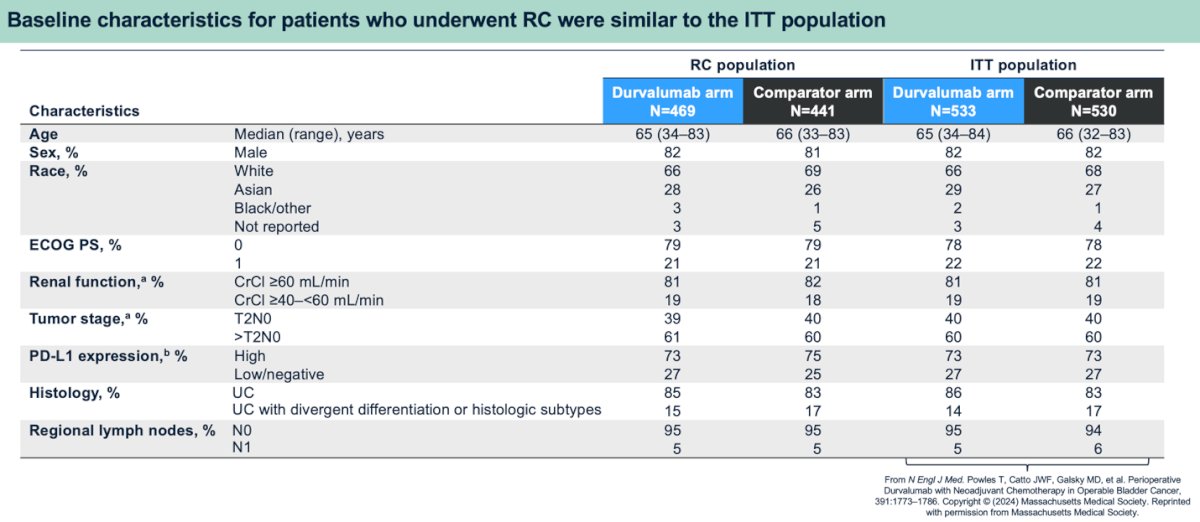
For the DFS analysis, baseline characteristics of patients who underwent RC were similar to those of the ITT population, as shown in the table below. Notably, the study design capped enrollment of patients with tumor stage T2 at 40% and those with a creatinine clearance (CrCl) <60 mL/min at 20%. The ITT population data referenced here is derived from the previously published results of the NIAGARA trial.1
The pathological complete response (pCR) rate in the radical cystectomy (RC) population was 42% with perioperative durvalumab plus neoadjuvant chemotherapy (NAC), compared to 33% with NAC alone. The odds ratio for achieving a pCR with the combination was 1.56 (95% CI, 1.18–2.06; nominal P = 0.0017).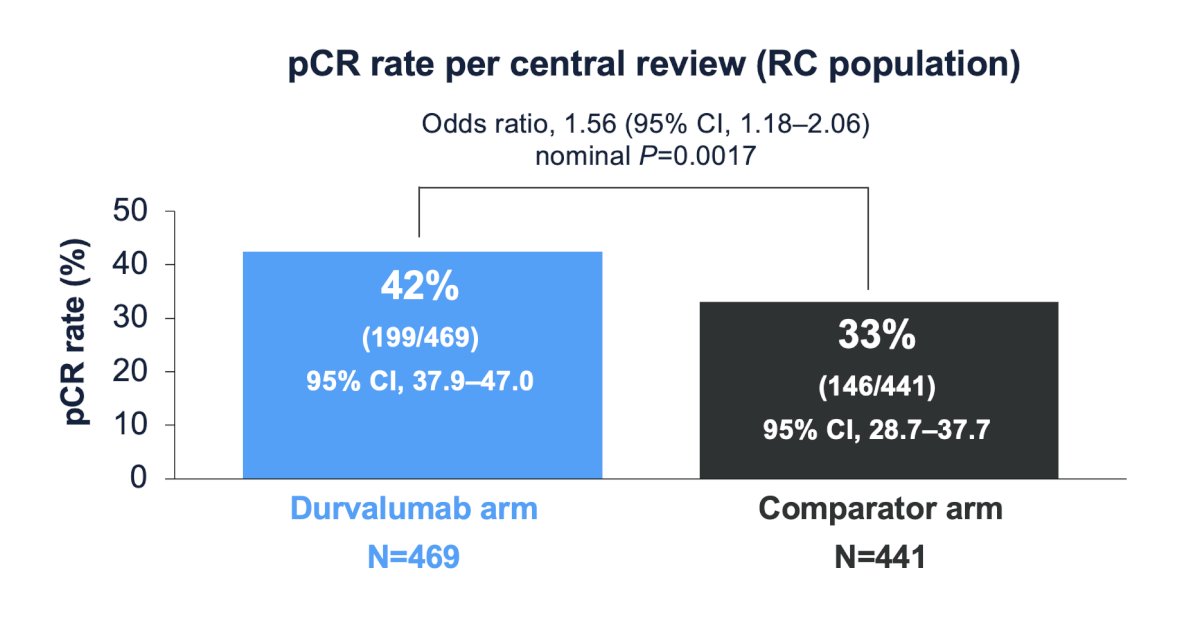
Perioperative durvalumab plus NAC reduced the risk of recurrence or death following RC by 31%, with a hazard ratio of 0.69 (95% CI, 0.51–0.93; nominal P = 0.0143).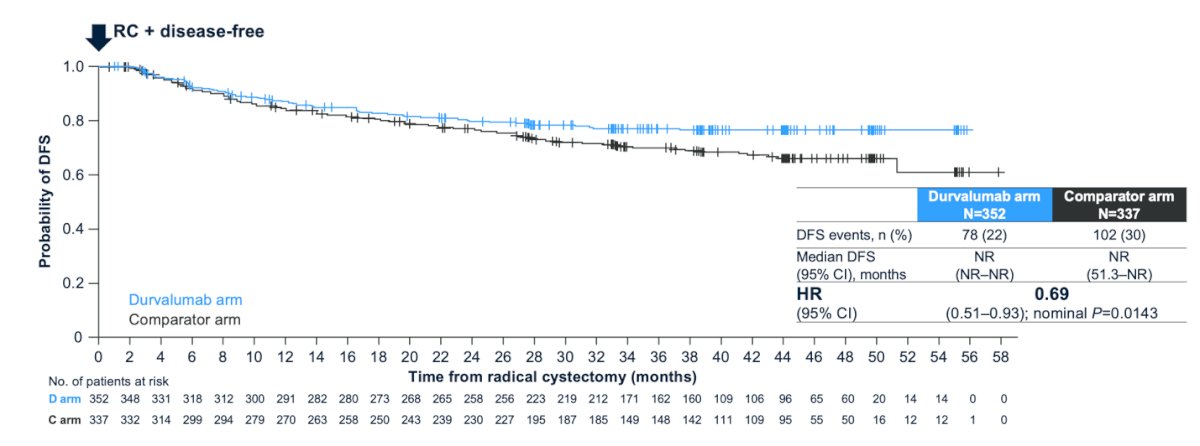
Notably, perioperative durvalumab plus NAC improved DFS in both the pCR group (HR, 0.58; 95% CI, 0.33–1.00) and the non-pCR group (HR, 0.82; 95% CI, 0.64–1.05), with both DFS curves separating early.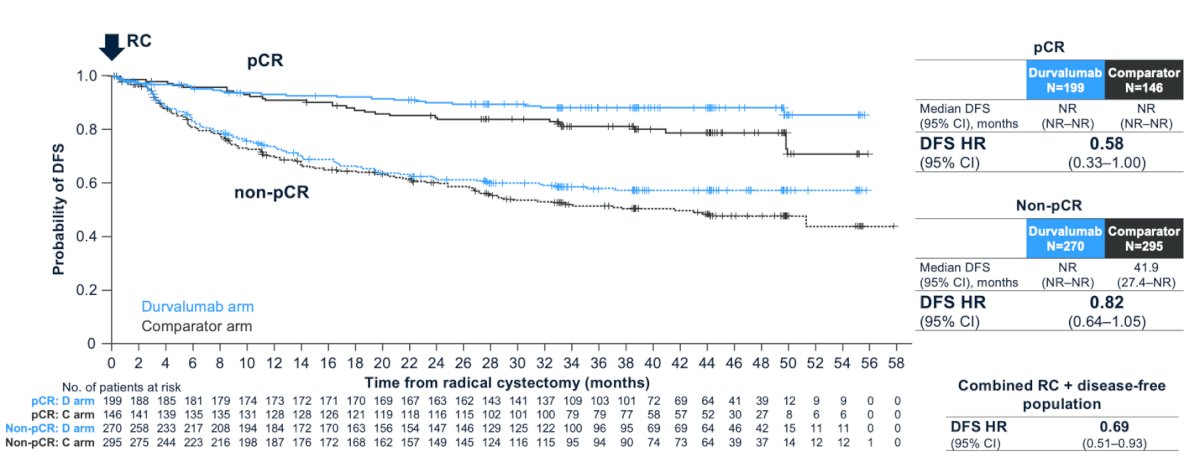
Dr. Meeks highlighted that the DFS benefit with perioperative durvalumab was consistently observed across prespecified subgroups when compared to the comparator arm, and patients with borderline renal function (CrCl ≥40–<60 mL/min) had DFS benefit with perioperative durvalumab vs comparator as shown in the forest plot below.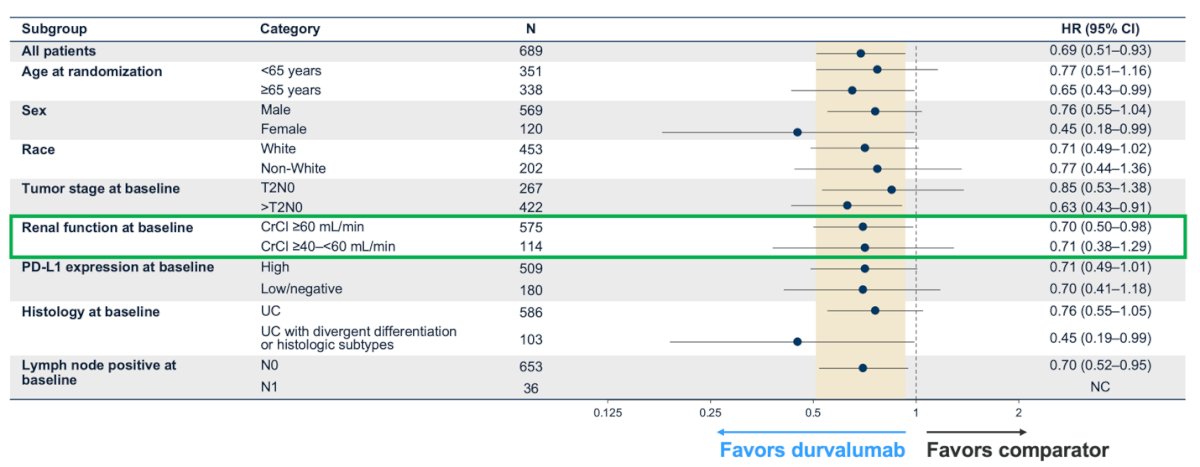
Furthermore, Dr. Meeks presented an analysis of pCR and EFS outcomes in the borderline renal function population (CrCl ≥40–<60 mL/min). He highlighted that perioperative durvalumab plus NAC improved both the pCR rate (32% vs. 16%) and EFS (median 53.3 vs. 22.8 months) in this subgroup, as illustrated in the graphics below.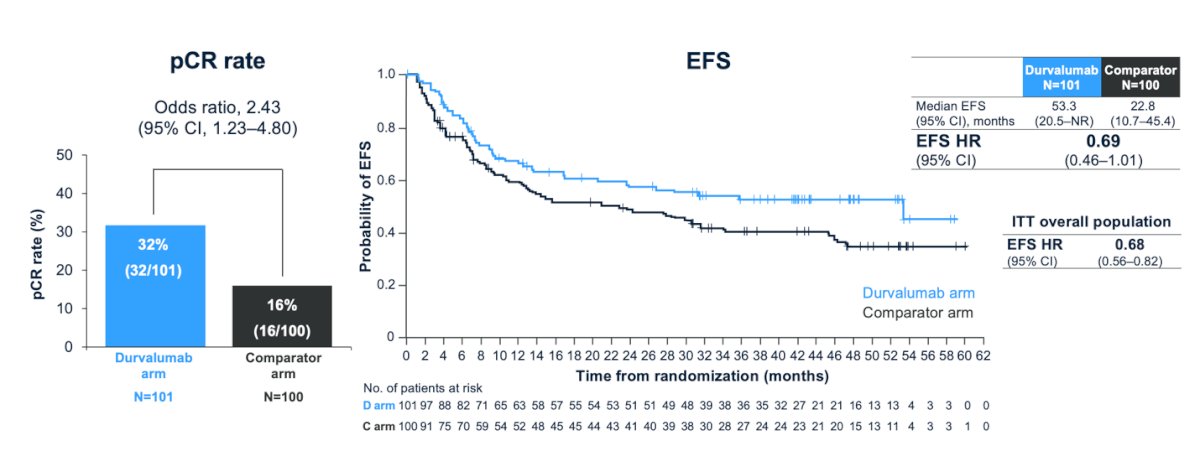
Lastly, the safety profile was generally similar between treatment arms and across subgroup populations. Notably, adverse events (AEs) leading to discontinuation of neoadjuvant durvalumab occurred in 11% of patients in the borderline renal function group (CrCl ≥40–<60 mL/min) and in 9% of the overall safety analysis population (CrCl ≥40 mL/min). Discontinuation of adjuvant durvalumab due to AEs was reported in 6% of patients in the borderline renal function group and in 8% of the overall safety population.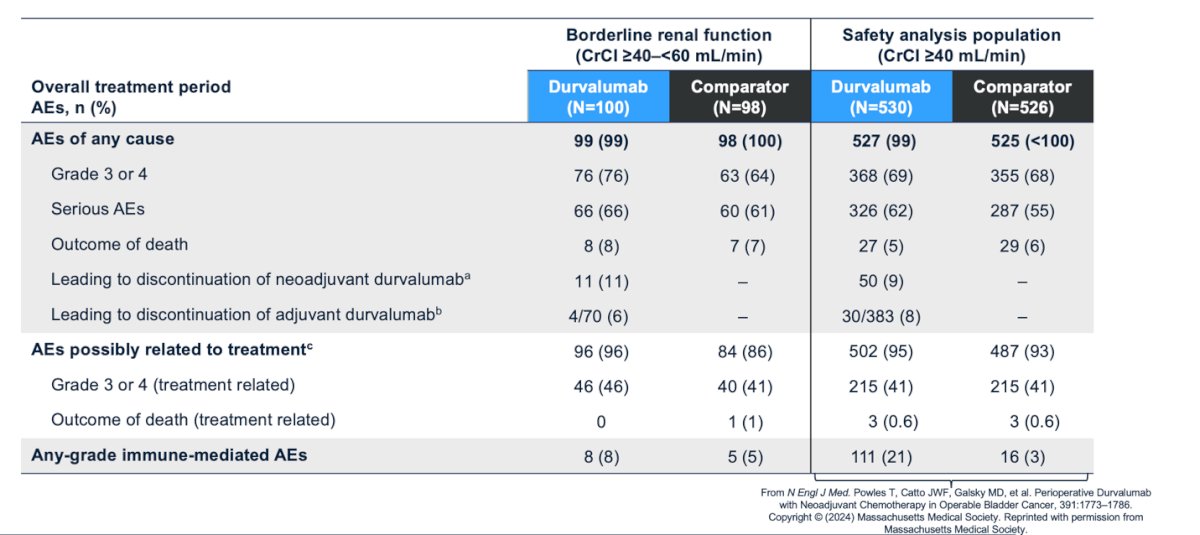
Dr. Meeks concluded his presentation with the following take-home messages:
- The NIAGARA trial demonstrated a statistically significant and clinically meaningful improvement in EFS (HR, 0.68; 95% CI, 0.56–0.82) and OS (HR, 0.75; 95% CI, 0.59–0.93).
- In the radical cystectomy population, perioperative durvalumab:
- Improved the pathological complete response rate (42% vs. 33%)
- Reduced the risk of recurrence or death post-RC by 31%
- Demonstrated a DFS benefit across prespecified subgroups and in both pCR and non-pCR groups
- Patients with borderline renal function (CrCl ≥40–<60 mL/min) experienced improvements in both pCR and EFS with perioperative durvalumab, with a safety profile consistent with the overall study population.
Presented by: Joshua Meeks, MD, PhD, Associate Professor of Urology, Biochemistry and Molecular Genetics at the Northwestern University Feinberg School of Medicine and Section Chief of Robotic Surgery at the Jesse Brown VA Medical Center. Chicago, IL
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
Related content: NIAGARA Study: Durvalumab Improves DFS in Muscle-Invasive Bladder Cancer Post-Cystectomy - Joshua Meeks
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Flaig TW, Spiess PE, Abern M, Agarwal N, Bangs R, Buyyounouski MK, et al. NCCN Guidelines® Insights: Bladder Cancer, Version 3.2024. JNCCN Journal of the National Comprehensive Cancer Network. 2024;22(4):216–225.