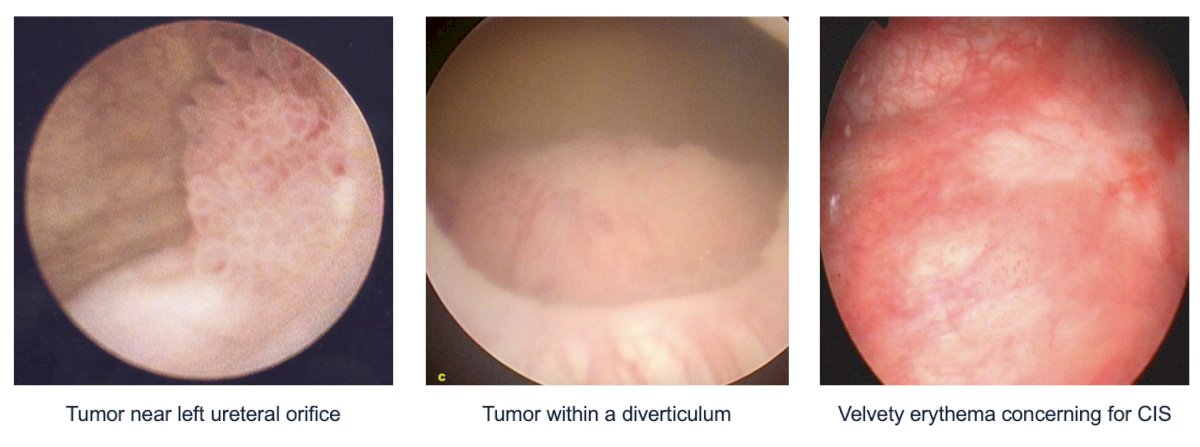
(UroToday.com) The 2025 AUA annual meeting featured the 4th annual IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. William Tabayoyong, with a debate between Drs. Vignesh Packiam and Mark Tyson are discussing what constitutes an optimal TURBT in 2025. Dr. Tabayoyong started by presenting a case of a 66 year old male (former heavy smoker) who presented with gross hematuria. His CT urogram showed normal upper tracts, a 1 cm tumor on the left lateral wall overlying the left ureteral orifice, and a 2 cm tumor within a right diverticulum. A flexible cystoscopy confirmed the tumors seen on the CT urogram and identified a velvety erythematous patch on the posterior bladder wall:
Dr. Tabayoyong then polled the audience based on the following scenario “Choose the FALSE statement regarding high quality TURBT” The following were the options available:
- All visible tumor should be completely resected and include detrusor muscle
- Prior to resection, tumor size, location, and number of tumors should be documented
- Use of blue light cystoscopy has shown reduced recurrence rates
- Use of blue light cystoscopy has been shown to improve overall survival
Dr. Tyson then discussed surgeon factors in an optimal TURBT. Dr. Tyson notes that even with the best and most flashy technology, the success of TURBT ultimately hinges on (i) technique, (ii) judgement, and (iii) adherence to oncologic principles. Historical data have consistently shown that TURBT quality varies dramatically across providers and institutions, even with identical equipment. In his practice, Dr. Tyson knows that he has a preoperative plan that starts before the resection:
- Review cross sectional imaging
- Localize and characterize all the lesions
- Plan access and resection of all tumors
- Anticipate risks
- Align with pathology and a follow-up plan

Dr. Tyson lists the following do’s and don’ts with regard to intraoperative technique:
- Do’s:
- Resect to obtain detrusor muscle
- Control bleeding early
- Resect or biopsy all visible lesions
- Minimize cautery artifact
- Photo-document tumor beds and orifices
- Use a systemic approach (checklist)
- Don’ts:
- Don’t leave tumor behind
- Don’t perforate the bladder
Dr. Tyson also touched on whether TURBT success is secondary to the scope or the surgeon:
- Technology
- Improves visualization (ie. blue light or narrow band imaging)
- Reduces artifact (en bloc or bipolar)
- Assists in teaching
- Surgeon
- Interprets findings
- Decides where to biopsy
- Chooses resection technique
- Manages risks
- Controls energy
- Handles tissue
- Detects subtle lesions like CIS
- Anticipates and avoids complications
- Leads the case, trains the team, prepares for surgery
Dr. Tyson concluded his portion of the debate by stating that the best outcomes don’t come from the most advanced scope, but from the most deliberate surgeon using it well.
Next, Dr. Packiam discussed that surgeon + technology factors are key to the optimal TURBT. Dr. Packiam notes that the success of TURBT ultimately hinges on the surgeon, as well as utilizing contemporary technology. This includes:
- Enhanced resection (ie. bipolar resection, etc)
- Optimizing pathologic sampling
- Safety
- Enhanced visualization (ie. blue light cystoscopy, etc)
- Accurate disease characterization
- (More) complete resection of CIS
Dr. Packiam emphasized that contemporary non muscle invasive bladder cancer outcomes are improving, with historic BCG 2 year recurrence free survival rates of ~60% compared to more contemporary BCG 2 year recurrence free survival rates of ~80-85%:

Why this is happening is likely multifactorial: better TURBTs may be occurring because of better quality surgeons, and improved technology (bipolar, blue light). Moreover, even in BCG unresponsive non muscle invasive bladder cancer, outcomes are improving: historic 1 year recurrence free rates of ~20%, compared to contemporary BCG recurrence free survival rates of ~70%. And, with both outcomes using nearly identical BCG regimens.
Bipolar TURBT and laser techniques allow more accurate pathology (better muscle sampling, less char), a safer resection, and a more complete resection. Blue light cystoscopy allows for more complete detection, with consistent randomized clinical trial data showing accurate disease characterization. Blue light cystoscopy also allows for a more complete resection, detecting occult CIS and small papillary lesions and margins, contributing to better outcomes over time for BCG-unresponsive disease.
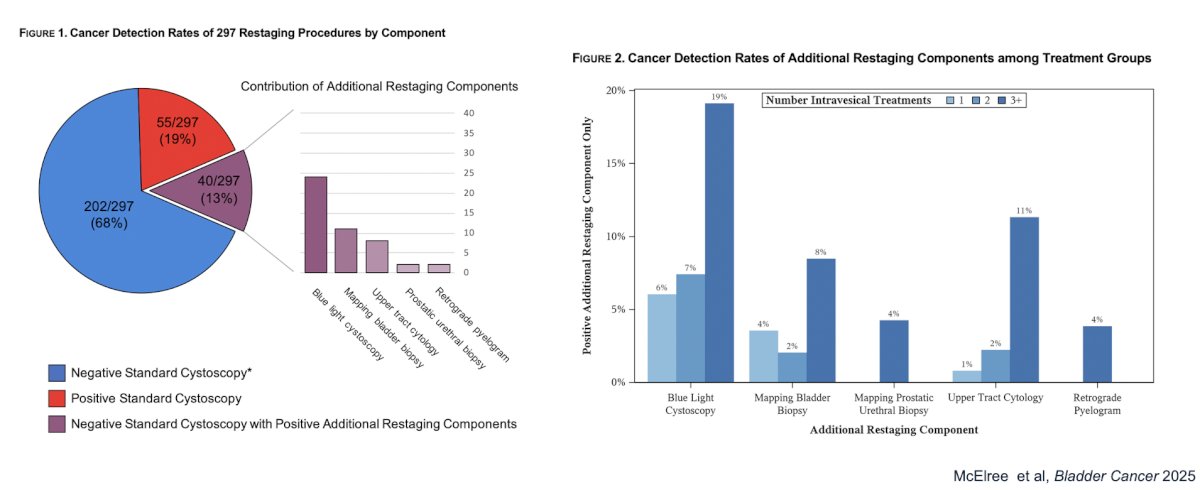
Blue light cystoscopy also leads to better surveillance. In a retrospective review of 297 patients with enhanced restaging after induction therapies (161 received 1 treatment, 63 received 2 treatments, and 73 received 3+ treatments). Enhanced procedures included standard cystoscopy + blue light cystoscopy, mapping bladder biopsies, retrograde pyelograms, upper tract cytology, and prostatic urethral biopsies. Importantly, these enhanced staging techniques led to 13% more cancers being detected:
Dr. Packiam concluded his portion of the debate by stating that the best outcomes come from an excellent surgeon using contemporary technology.
The debate concluded by highlighting the pre- and post-debate answers to the polling question “Choose the FALSE statement regarding high quality TURBT”
- All visible tumor should be completely resected and include detrusor muscle
- Pre-debate: 12%
- Post-debate: 18%
- Prior to resection, tumor size, location, and number of tumors should be documented
- Pre-debate: 3%
- Post-debate: 0%
- Use of blue light cystoscopy has shown reduced recurrence rates
- Pre-debate: 7%
- Post-debate: 3%
- Use of blue light cystoscopy has shown to improve overall survival
- Pre-debate: 78%
- Post-debate: 79%
Presented by:
- Vignesh Packiam, MD, Rutgers Cancer Institute, New Brunswick, NJ
- Mark Tyson, MD, MPH, Mayo Clinic, Phoenix, AZ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025