(UroToday.com) The 2025 AUA annual meeting featured the 4th annual IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Bernard Bochner, with a debate between Drs. Sia Daneshmand and Matthew Galsky are discussing whether bladder preservation in patients with clinical complete response to neoadjuvant chemotherapy is ready for prime time.
Dr. Bochner started the discussion with a case presentation of a 64 year old man who presented with hematuria and a subsequent in office cystoscopy confirming a solid appearing bladder mass. An MRI was obtained and showed a 7 cm mass, staged cT3N0. A TURBT was then performed, which demonstrated a large mass, but with a palpable and mobile bladder on examination under anesthesia. Pathology from the TURBT was poorly differentiated urothelial carcinoma, with muscle invasion, and suspicion for lymphovascular invasion. This patient’s medical history was significant for hypertension; his creatinine was 1.3 ng/dL (eGFR 61 mL/min), and his MSK-IMPACT test showed an ERCC2 mutation. He then opted for neoadjuvant gemcitabine + cisplatin chemotherapy, receiving 4 cycles of therapy. Post chemotherapy PET/CT showed no evidence of disease, with some bladder wall thickening. A cystoscopy with biopsy was performed, and it also showed no evidence of disease. Dr. Bochner then polled the audience based on the following question: “What percentage of >cT2 bladder cancer patients are reasonable candidates for a chemotherapy alone (bladder sparing) approach if they have clinical complete response after chemotherapy?” The following were the options available:
- Never, always proceed with surgical consolidation unless part of a clinical trial
- <10%
- Up to half of patients
- The majority of patients
- Always
Dr. Galsky then discussed his thoughts on bladder preservation in patients with clinical complete response to neoadjuvant chemotherapy. Dr. Galsky started by highlighting Dr. Harry Herr’s classic 1998 paper1 reporting 10-year outcomes of patients with invasive (T2-3N0M0) bladder cancer who responded completely to MVAC chemotherapy followed by bladder-sparing surgery.1 Among 111 surgical candidates, 60 (54%) achieved a complete clinical response (T0) on transurethral resection of the primary tumor site. Of these, 28 requested follow-up with TUR alone, 15 had a partial cystectomy, and 17 elected a radical cystectomy. These patients were followed up for a median of 10 years (range, 8 to 13 years). Overall, among the 43 patients who had bladder-sparing surgery, 32 (74%) were alive, including 25 (58%) with an intact functioning bladder. Twenty-four patients (56%) developed bladder tumor recurrences from 5 to 96 months, which were invasive in 13 (30%) and superficial in 11 (26%). Ultimately, 13 patients required a salvage cystectomy, of whom 6 died, including 4 (9%) from a new invasive neoplasm. Of the 17 patients who had radical cystectomy, 11 (65%) were alive at the time of last study follow-up. Dr. Galsky stated that retrospective studies and anecdotes tell us what can be achieved, but not necessarily what should be achieved or how it should be achieved.
There are several historical barriers to TURBT + systemic therapy as definitive treatment for muscle invasive bladder cancer, including:
- A paucity of prospective studies
- Lack of uniform and rigorous methods to measure and define clinical complete response
- A limited understanding of the role of delayed cystectomy in patients with local recurrence
- Suboptimal systemic therapeutic regimens
- Absence of biomarkers to refine decision making
Also important is to define what a clinical complete response is. Clinical complete response is a biomarker, and we do not define biomarkers arbitrarily. We pre-specify definitions and prospectively assess performance characteristics. Thus, with regards to a framework, clinical complete response does not necessarily equal pathological complete response. To date, we have been looking for the right answer to the wrong question:
- The biology and treatment history of local recurrence after a clinical complete response are poorly defined
- ‘Salvage’ local therapy has played a key role in organ preservation approaches in other solid tumors
- If cancer control is not compromised, the risk adapted individualized approach is still favorable to upfront cystectomy for all approaches
In HCRN GU16-257, patients received nivolumab + gemcitabine/cisplatin chemotherapy x 4 cycles, after which they were re-staged with cystoscopy + biopsy, urine cytology, and MRI. Those with evidence of a complete clinical response were recommended to forgo cystectomy and received adjuvant nivolumab every 2 weeks for a total of 8 cycles. The primary endpoint was 2-year metastasis free survival or <ypT1N0 in patients with a complete clinical response:
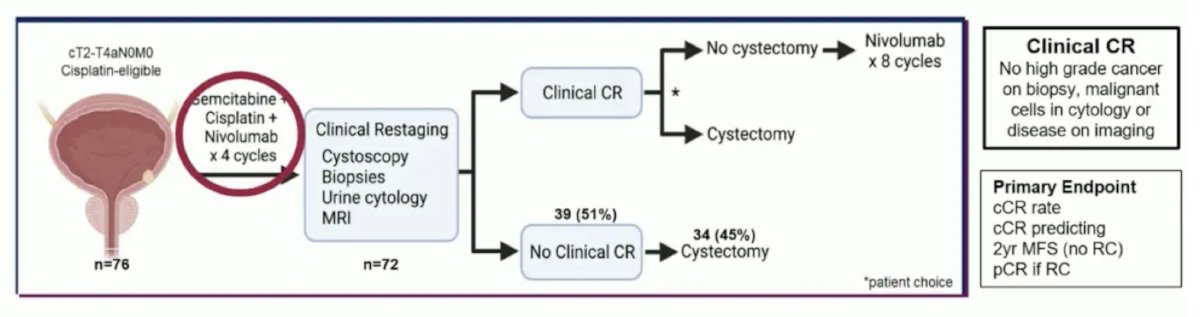
Among the 72 patients who were recruited and subsequently underwent clinical re-staging, 33 patients (46%) had evidence of a complete clinical response. One patient opted for immediate cystectomy, with the remaining 32 proceeding with active surveillance. Overall, 1 patient developed metastases each before and after 2 years follow-up. Of these 2, 1 had died of their metastatic disease, and 9 patients underwent a cystectomy during a minimum follow-up of 19 months:
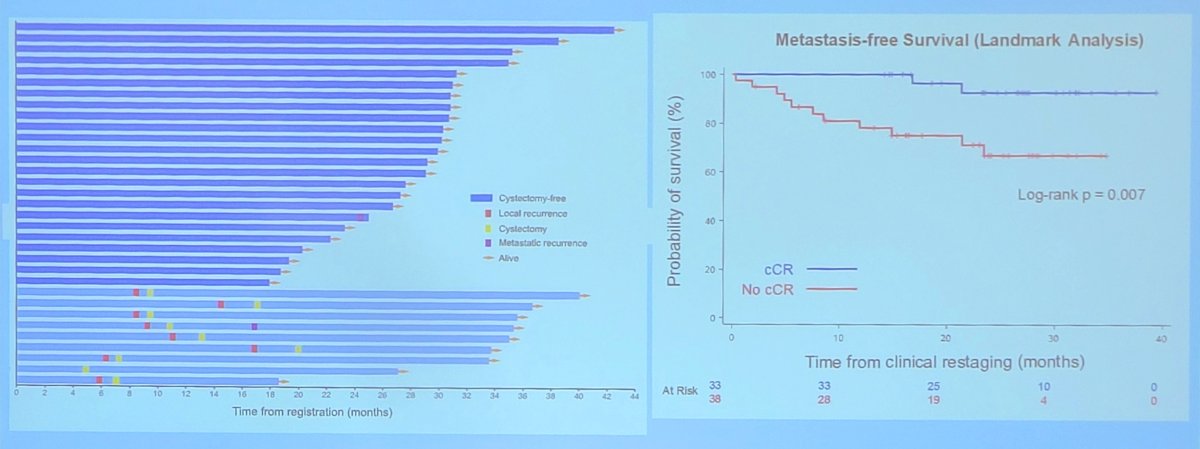
Overall, the positive predictive value of clinical completer response for 2 year metastasis free survival was 0.97 (95% CI 0.91-1.00).
Dr. Galsky concluded his portion of the debate with the following take home messages:
- Bladder preservation in patients with clinical complete response to neoadjuvant therapy is not ready for primetime, but not because we have answered the question that we should not do this
- A foundational set of prospective studies coupled with markedly improved systemic therapies is creating a watershed moment to redefine muscle invasive bladder cancer care
- The stakes are high, and we need to get this right
Dr. Daneshmand then discussed his thoughts on whether bladder preservation in patients with clinical complete response to neoadjuvant therapy is ready for primetime. There are several important questions to answer when deciding whether radical cystectomy can be omitted:
- Does cT0 = pT0?
- Can we use biomarkers to predict response to chemotherapy?
- Is salvage/delayed radical cystectomy = up front cystectomy?
- Are we under-treating metastatic disease?
- What is the financial and emotional stress/toxicity of ongoing surveillance versus radical cystectomy?
Historically, the natural history of pathological complete response (pT0N0) in SWOG87102 is an 85% overall survival rate, 26% lower absolute risk of mortality, 51% absolute lower risk of recurrence compared with residual disease, and a natural history of ypT > 0 residual disease having a 3.4 year overall survival benefit versus an 11 year survival benefit for ypT0. At his institution (USC), Dr. Daneshmand notes that the natural history of ypT0/pT0N0 (n = 234, 2000-2019) is a recurrence free survival rate of 85%/84% for ypT0 and 99%/95% for pT0.3
There is a very important role for accurate clinical staging of these patients. Traditional staging has included CT (or other cross sectional imaging), TURBT (after chemotherapy), physical exam (bimanual), and cytology. The following summarizes the body of literature in this space:
- MD Anderson:
- 35% correct rate of ypT0
- 25% >=T3 or N+ (12.7% N+)
- SWOG 0219:
- 40% correct rate of ypT0
- Multi-institutional:
- 47% correct rate of pT0
- 43% >= T2 and 12% N+
- Columbia:
- 66% correct rate of ypT0
With regards to TURBT accuracy after neoadjuvant chemotherapy, Dr. Daneshmand highlighted the SEE trial at Fox Chase Cancer Center. This was a prospective, single arm trial assessing cystoscopy and systematic bladder tissue sampling in predicting pT0 bladder cancer.4 Overall, 61 patients underwent neoadjuvant chemotherapy, Systematic Endoscopic Evaluation (SEE), and radical cystectomy. On SEE, 31 (50.8%) demonstrated no visual or biopsy-based evidence of disease (SEE T0). However, among these patients, 16/31 (51.6%) harbored residual disease (>pT0), and 8/31 (25.8%) had residual >= pT2 disease at the time of cystectomy. The negative predictive value of SEE predicting pT0 bladder cancer was 48.4% (95% CI 30.2-66.9), which was below the pre-specified hypothesis, thus, the trial was stopped for futility.
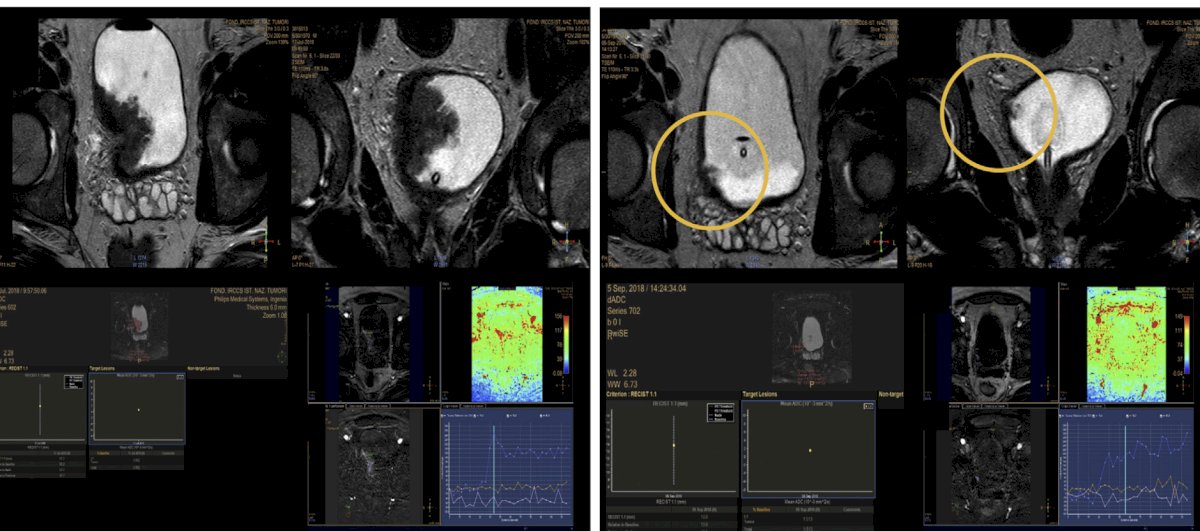
Data from the PURE-01 study,5 assessing 82 patients with 164 total multiparametric MRIs, showed that the agreement between the internal and external mpMRI assessments after therapy was acceptable (κ values ranging from 0.5 to 0.76). The AUC was 0.74 for residual disease, pT0 showed 62-73% accuracy, pT<=1 showed 95% accuracy, with 20% inter-observer disagreement:
Dr. Daneshmand then discussed RETAIN I,6 a phase II, multi-institutional, non-inferiority trial to evaluate a risk-adapted approach to the treatment of muscle invasive bladder cancer. Pre-chemotherapy, the primary tumor is sequenced for ATM, ERCC2, FANCC, or RB1, then the patient is treated with 3 cycles of neoadjuvant accelerated MVAC followed by a restaging TURBT:
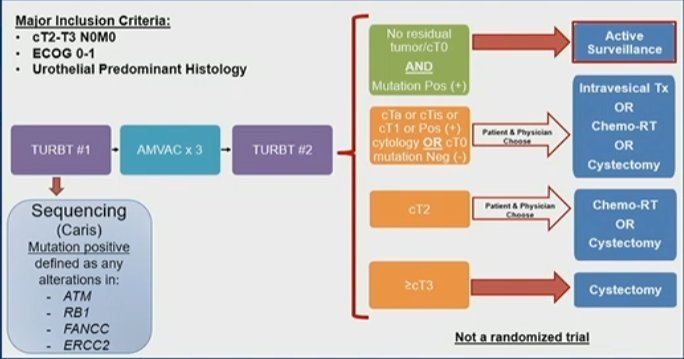
The primary end point of the trial is metastasis free survival at 2 years. There were 70 patients enrolled, 33 (47%) had a mutation, and 25 (36%) began per-protocol active surveillance. With a median follow-up of 40 months, the 2-year metastasis free survival rate for all patients was 72.9% (lower bound exact one-sided 95% CI 62.8). The 2-year metastasis free survival rate was 76.0% in the active surveillance group (95% CI 54.2 to 88.4) and 71.1% (95% CI 55.5 to 82.1) in the remaining patients. In the active surveillance group, 17 patients (68%) had some recurrence, and 12 (48%) were metastasis-free with an intact bladder. The 2-year overall survival rate was 84.3% (95% CI 73.4 to 91.0), including 88.0% (95% CI 67.3 to 96.0) and 82.2% (95% CI 67.6 to 90.7) in the active surveillance and non-active surveillance groups, respectively. Importantly, 48% of the active surveillance group avoided cystectomy without metastatic disease.
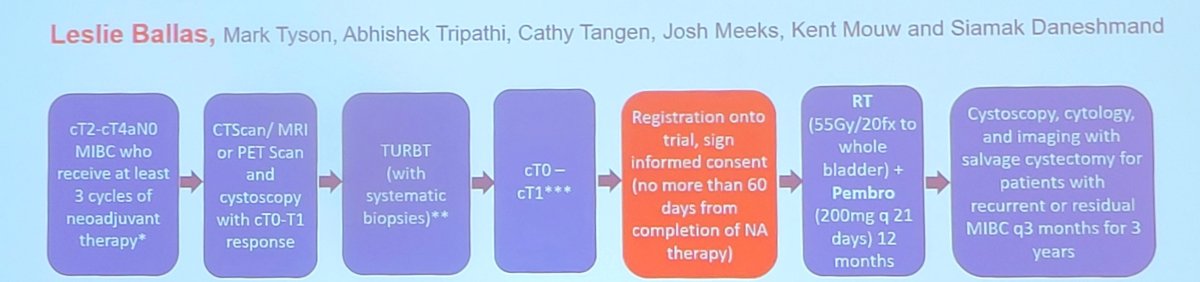
Dr. Daneshmand also cautioned that we have to be careful of ypT0 but N+ disease, which has been as high as ~13% in population level studies, and 3.6% in their USC series of patients. To conclude his discussion, Dr. Daneshmand noted the SWOG S2427 BRIGHT trial assessing bladder preservation with immunoradiotherapy after a clinically meaningful response to neoadjuvant therapy in patients with muscle invasive bladder cancer:
The debate concluded by highlighting the pre- and post-debate answers to the polling question “What percentage of >cT2 bladder cancer patients are reasonable candidates for a chemotherapy alone (bladder sparing) approach if they have clinical complete response after chemotherapy?”
- Never, always proceed with surgical consolidation unless part of a clinical trial
- Pre-debate: 46%
- Post-debate: 51%
- <10%
- Pre-debate: 30%
- Post-debate: 33%
- Up to half of patients
- Pre-debate: 13%
- Post-debate: 8%
- The majority of patients
- Pre-debate: 11%
- Post-debate: 5%
- Always
- Pre-debate: 0%
- Post-debate: 3%
Presented by:
- Sia Daneshmand, MD, University of Southern California, Los Angeles, CA
- Matthew Galsky, MD, Icahn School of Medicine at Mount Sinai, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Herr H, Bajorin DF, Scher HI. Neoadjuvant Chemotherapy and Bladder-Sparing Surgery for Invasive Bladder Cancer: Ten-Year Outcome. J Clin Oncol. 1998;16:1298-1301.
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349(9):859-866.
- Douglawi A, Ghoreifi A, Lee R, et al. Recurrence patterns in bladder cancer patients with no residual disease (pT0N0) at radical cystectomy: A 20-year experience. Urol Oncol. 2023 Feb;41(2):107.e9-107.e14.
- Zibelman M, Asghar AM, Parker DC, et al. Cystoscopy and systematic bladder tissue sampling in predicting pT0 Bladder Cancer: A Prospective Trial. J Urol. 2021 Jun;205(6):1605-1611.
- Necchi A, Bandini M, Calareso G, et al. Multiparametric Magnetic Resonance Imaging as a Noninvasive Assessment of Tumor Response to Neoadjuvant Pembrolizumab in Muscle-invasive bladder cancer: Preliminary findings from the PURE-01 Study. Eur Urol. 2020 May;77(5):636-643.
- Geynisman DM, Abbosh PH, Ross E, et al. Phase II trial of risk-enabled therapy after neoadjuvant chemotherapy for muscle-invasive bladder cancer (RETAIN 1). J Clin Oncol. 2025 Mar 20;43(9):1113-1122.